



Case Report - Year 2019 - Volume 34 -
Cryptotia in a Western adult patient: A case report
Criptotia em paciente ocidental adulto: relato de caso
Jonathan Augusto Vidal Oliveira1,2,* ; Alberto Ferraz de Melo3; Luiz Alberto de Souza Leite3; Carlos Lacerda De Andrade Almeida2; Letícia Kelly Domingos Brito1; Evelliny Gomes da Silva1; Antônio Lucas do Nascimento Silva1; José Igor Moura de Arruda1
; Alberto Ferraz de Melo3; Luiz Alberto de Souza Leite3; Carlos Lacerda De Andrade Almeida2; Letícia Kelly Domingos Brito1; Evelliny Gomes da Silva1; Antônio Lucas do Nascimento Silva1; José Igor Moura de Arruda1
ABSTRACT
Introduction: Cryptotia is a congenital ear deformity common
in Easterners and rare in Westerners, with most studies
addressing Eastern surgical techniques applied to children.
In this pathology, the cartilage of the upper pole of the ear is
lodged subcutaneously in the temporal region, which prevents
individuals from using glasses due to lack of support and
prevents esthetic definition of the upper pole.
Objective: The
present study aimed to report the case of an adult patient
with cryptotia undergoing surgical treatment using a mastoid
subcutaneous pedicle flap and review the main techniques
described for the treatment of this involvement.
Conclusion: The subcutaneous pedicle flap described by Yoshimura proved
to be adequate for correcting cryptotia in a Western adult patient.
Keywords: Adult; Congenital abnormalities; External ear; Ear cartilage; esthetic
RESUMO
Introdução: criptotia é uma deformidade auricular congênita
comum em orientais e rara em ocidentais, sendo a grande
maioria dos estudos de técnicas cirúrgicas orientais e
aplicados em crianças. Nesta patologia, a cartilagem do polo
superior da orelha encontra-se alojada embaixo da pele na
região temporal, o que impossibilita o uso de óculos, devido à
falta de apoio e torna o polo superior sem definição estética.
Objetivo: o presente estudo tem por objetivo relatar o caso de
um paciente adulto com criptotia, submetido ao tratamento
cirúrgico com retalho de pedículo subcutâneo mastóideo,
revisando as principais técnicas descritas para o tratamento
deste acometimento.
Conclusão: o retalho de pedículo
subcutâneo descrito por Yoshimura, mostrou-se adequado
para a correção da criptotia em paciente ocidental e adulto.
Palavras-chave: Adulto; Anormalidades congênitas; Orelha externa; Cartilagem da orelha; Estética
INTRODUCTION
Although cryptotia is a common congenital ear deformity in Easterners with an incidence of 1:400 in the Japanese population, it is very rare in Westerners1. Its exact cause is not well understood, but the different hypotheses include poor embryonic development, intrauterine mechanical pressure, and ear muscle abnormalities2,3.
In cryptotia, an invagination of the upper pole of the ear under the skin of the temporal region develops. Consequently, the auriculocephalic sulcus is lost2,4. In 19853, Hirose et al. classified cryptotia by type of cartilage constriction and abnormal development of the intrinsic musculature into type I (transverse muscle or superior crus) and type II (oblique muscle or inferior crus)3.
Secondary abnormalities that may coexist with cryptotia include cartilage deformity, underdeveloped scapha, and a markedly curved crus of the antihelix3. Esthetic and functional impairments in patients with this pathology include the inability to wear glasses due to a loss of support and a very apparent esthetic stigma.
The present study aimed to report the case of a Western adult patient with cryptotia undergoing reconstruction using a mastoid subcutaneous pedicle flap and review the main techniques described for its treatment.
CASE REPORT
A 53-year-old male patient, S.M.S., born in Pernambuco, Brazil, visited the plastic surgery outpatient clinic of Agamenon Magalhães Hospital - PE in November 2014. He reported having difficulty supporting his glasses on his right ear, thus requiring the use of a strap between the temples of the glasses. He also complained about the unesthetic appearance caused by adherence of the ear to the temple. He had no history of a previous surgical procedure.
Examination revealed that the upper pole of the right ear was covered by the skin of the temporal region and the right auriculotemporal sulcus was absent. The auricular cartilage had a slightly anteroposterior constriction compatible with the type II classification described by Hirose et al. in 19853(Figure 1).


The surgical procedure was performed under local anesthesia and sedation with 0.5% lidocaine solution and 1:200,000 adrenaline. The technique described by Yoshimura et al. in 20007 was performed, with the retroauricular sulcus being caudally demarcated and the skin island being projected on the mastoid with its central portion positioned in the sulcus. After an incision was made and the cartilage from the upper pole was removed, the superficial mastoid fascia was identified and dissected posteriorly and anteriorly. The skin island was incised with the fascia in its caudal region, which was cranially displaced until the flap rotation arc was reached (Figures 2 and 3).




Radial incisions were made on the posterior concave surface of the helix to release the cartilaginous constriction. The flap was positioned in the area of the defect and fixed with separate 5-0 nylon sutures (Figure 4).
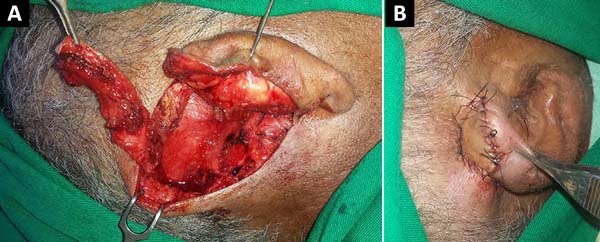

The flap remained well perfused in the postoperative period, with a slight area of epidermolysis in the distal portion, but no esthetic or functional damage. After 2 weeks, the stitches were removed and the patient could support the glasses on the flap. The results were satisfactory, both esthetically, with definition of the contour of the upper pole of the ear, and functionally, with better support of the glasses on the ear (Figure 5).


DISCUSSION
Splints or tapes are used in the non-surgical management of cryptotia. Non-surgical management is indicated for patients with mild deformities, usually children aged 1 week to 6 months2. Matsuo et al. reported in 19845that correction can be achieved using compression and fixation appliances in the first 6 months of life. Residual deformities frequently persist, requiring minor surgical intervention5.
All surgical techniques used to treat cryptotia aim at correcting the lack of skin in the upper pole of the ear and the existing cartilage defects4. However, most of the described techniques result in visible scars on the capillary line of the temporal and pre-auricular regions, even lowering the capillary line of the temple, taking hair follicles to the auriculotemporal sulcus and helix as in the V-Y technique6,7.
Thus, the techniques described to correct cryptotia can be divided into local flaps, skin grafts, and tissue expansion. The use of local flaps is the most common technique with the description of several flaps, such as the V-Y flap and its variations6, rotation flaps3, transposition flaps8, z-plasties2, and subcutaneous pedicle flaps7. They generally have a good esthetic result, with the scarring result depending on the technique used and low complication rates6. Recurrence may occur with these techniques due to the skin defect cause by this pathology and the need for large skin segments, resulting in extensive scars and significant changes in the temporal and mastoid capillary regions2.
Although skin grafts have the advantage of covering larger wounds, they heal more slowly. The texture and color of the region change, which is often unacceptable, and healing problems generally occur9. The correction of cryptotia using a skin expander has the advantage of providing a good amount of skin for reconstructing the auriculotemporal sulcus10. However, it is rarely used because it requires two surgical sessions and skin expansion for weeks and causes discomfort in the region in which it is placed.
Thus, the technique chosen for the patient was that described by Yoshimura et al. in 20007: A mastoid fascia island flap supplied by the posterior branch of the superficial temporal artery and/or the superior auricular artery7. This technique allows the correction of skin defects without requiring changing of the capillary implantation line or resulting in very apparent scars in the mastoid or temporal regions, resulting only in a scar hidden in the retroauricular sulcus.
CONCLUSION
Therefore, although most studies to date have described cryptotia correction in children and Easterners, in the current study, use of the mastoid subcutaneous pedicle flap corrected cryptotia in a Western adult patient.
COLLABORATIONS
|
JAVO |
Analysis and/or data interpretation, Conception and design study, Data Curation, Final manuscript approval, Methodology, Project Administration, Supervision, Visualization, Writing - Original Draft Preparation, Writing - Review & Editing |
|
AFMN |
Analysis and/or data interpretation, Analysis and/or data interpretation, Data Curation, Final manuscript approval, Methodology, Supervision, Visualization, Writing - Original Draft Preparation |
|
LASL |
Analysis and/or data interpretation, Data Curation, Final manuscript approval, Methodology, Supervision, Visualization, Writing - Original Draft Preparation |
|
CLAA |
Analysis and/or data interpretation, Data Curation, Final manuscript approval, Methodology, Project Administration, Supervision, Visualization, Writing - Original Draft Preparation, Writing - Review & Editing |
|
LKDB |
Analysis and/or data interpretation, Data Curation, Final manuscript approval, Methodology, Writing - Original Draft Preparation, Writing - Review & Editing |
|
EGS |
Analysis and/or data interpretation, Data Curation, Final manuscript approval, Methodology, Writing - Original Draft Preparation, Writing - Review & Editing |
|
ALNS |
Analysis and/or data interpretation, Final manuscript approval, Methodology, Writing - Original Draft Preparation, Writing - Review & Editing |
|
JIMA |
Analysis and/or data interpretation, Final manuscript approval, Methodology, Writing - Original Draft Preparation, Writing - Review & Editing |
REFERENCES
1. Fukuda O. Otoplasty of cryptotia. Keisei Geka. 1968 Apr;11(2):117-125.
2. Hikiami R, Kakudo N, Morimoto N, Hihara M, Kusumoto K. A new modified method of correcting cryptotia with a subcutaneous pedicled flap. Plast Reconstr Surg Glob Open. 2017 Oct:5(10):e1548. PMID: 29184751 DOI: https://doi.org/10.1097/GOX.0000000000001548
3. Hirose T, Tomono T, Matsuo K, et al. Cryptotia: our classification and treatment. Br J Plast Surg. 1985 Jul;38(3):352-60. PMID: 4016423 DOI: https://doi.org/10.1016/0007-1226(85)90241-3
4. Kim SK, Yoon CM, Kim MH, Kim MS, Lee KC. Considerations for the management of cryptotia based on the experience of 34 patients. Arch Plast Surg. 2012 Nov;39(6):601-5. PMID: 23233884 DOI: https://doi.org/10.5999/aps.2012.39.6.601
5. Matsuo T, Hirose T, Tomono T, et al. Nonsurgical correction of congenital auricular deformities in the early neonate: a preliminary report. Plast Reconstr Surg. 1984 Jan;73(1):38-51. DOI: https://doi.org/10.1097/00006534-198401000-00010
6. Chang SO, Suh MW, Choi BY, Park MH, Oh SH, Kim CS. A new technique for correcting cryptotia: V-Y swing flap. Plast Reconstr Surg. 2007 Aug;120(2):437-441. DOI: https://doi.org/10.1097/01.prs.0000267423.72239.a0
7. Yoshimura K, Ouchi K, Wakita S, Uda K, Harii K. Surgical correction of cryptotia with superiorly based superficial mastoid fascia and skin paddle. Plast Reconstr Surg. 2000 Mar;105(3):836-841. DOI: https://doi.org/10.1097/00006534-200003000-00002
8. Ono I, Gunji H, Suda K, Tateshita T, Kaneko F. A new operative method for treating severe cryptotia. Plast Reconstr Surg. 1995 Aug;96(2):461-8. PMID: 7624424 DOI: https://doi.org/10.1097/00006534-199508000-00033
9. Park S, Takushima M, Minegishi M. Reconstruction of cryptotia using a skin graft. Ann Plast Surg. 1994 Apr;32(4):441-4. PMID: 8210169 DOI: https://doi.org/10.1097/00000637-199404000-00023
10. Mutimer KL, Mulliken JB. Correcting of cryptotia using tissue expansion. Plast Reconstr Surg. 1988 Apr;81(4):601-4. DOI: https://doi.org/10.1097/00006534-198804000-00021
1. Universidade Federal de Pernambuco, Caruaru, PE, Brazil.
2. Hospital Agamenon Magalhães, Recife, PE, Brazil.
3. Sociedade Brasileira de Cirurgia Plástica, São Paulo, SP, Brazil.
Corresponding author: Jonathan Augusto Vidal Oliveira Avenida República do Líbano, 251, Riomar Trade Center, Salas 2005 e 2006, Recife, PE, Brazil. Zipe Code: 51110-160. E-mail: jvidalplastica@gmail.com
Article received: October 20, 2018.
Article accepted: February 10, 2019.
Institution: Hospital Agamenom magalhaes, Recife, PE, Brasil.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket