



Original Article - Year 2019 - Volume 34 -
Analysis of Training in Plastic Surgery by the Brazilian Society of Plastic Surgery as Reported by Final Year Trainees
Análise dos serviços de Cirurgia Plástica da Sociedade Brasileira de Cirurgia Plástica sob o ponto de vista dos cirurgiões do último ano do curso de especialização em Cirurgia Plástica
ABSTRACT
Introduction: Much has been discussed about the training of a plastic surgeon nationally and internationally. There is a need to improve and standardize training to ensure the future of this specialty.
Methods: Questionnaires were filled by third year trainees at the Brazilian Congress of Plastic Surgery (Belo Horizonte).
Results: A total of 230 questionnaires were distributed and 113 were included in the study. The respondents included 71 men and 41 women; 34 were from institutions recognized by the Brazilian Society of Plastic Surgery (SBCP) and 71 were from institutions recognized by the Ministry of Education and the SBCP. Ninety-six respondents revealed that purely aesthetic procedures were conducted in their institutions, with an average of 54.3% of aesthetic procedures. The respondents had the least confidence in performing hair transplants and the most confidence in performing an abdominoplasty. The topic most requested for training was rhinoplasty and the least requested was abdominoplasty. The trainees were fairly satisfied with their programs, with an average satisfaction level of 3.89, on a scale of 1 to 5. The procedure that needed to be performed more frequently was rhinoplasty (more than 10 procedures). Most trainees felt that the program prepared them to practice surgeries, with an average of 3.8 on a scale of 1 to 5. Further, 65% found it necessary to have a fellowship, with mastology being the most requested. The most common procedure was reduction mammoplasty. Most of the trainees wanted to work in a private clinic.
Conclusion: In order to improve the level of education, the accredited institutions should meet the requirements necessary for good preparation of the trainees.
Keywords: Plastic Surgery; Continuing education; Education; Work; Aesthetics
RESUMO
Introdução: Muito se discute sobre a formação do cirurgião plástico na especialização
médica nacional e internacionalmente. Há necessidade da busca por melhoras e
padronização na formação visando o futuro da especialidade.
Métodos: Foi avaliado protocolo preenchido no Congresso Brasileiro de Cirurgia
Plástica (Belo Horizonte) por especializandos do terceiro ano.
Resultados: Foram distribuídos 230 protocolos. 113 protocolos foram incluídos. A amostra
incluiu 71 homens e 41 mulheres. 34 eram de serviços cadastrados pela
Sociedade Brasileira de Cirurgia Plástica (SBCP) e 71 eram de serviços
cadastrados pelo Ministério da Educação e SBCP. 96 afirmaram que em seus
serviços são realizados procedimentos puramente estéticos, com média de
54,3% de procedimentos estéticos. O procedimento com menos confiança em
realizar foi transplante capilar, e mais confiança foi abdominoplastia. Área
de interesse mais requisitada foi rinoplastia e a menos foi abdominoplastia.
Os especializandos estão regularmente satisfeitos com seus programas, com
média de 3,89, em uma escala de 1 a 5. O procedimento que deve ser mais
realizado foi rinoplastia, sendo necessário, do ponto de vista deles,
realizar mais de 10 procedimentos. Os especializandos sentem-se bem
preparados pela programa, com média de 3,8 em uma escala de 1 a 5. 65% deles
acham necessário fazer fellow, sendo o mais requisitado de mastologia. O
procedimento mais realizado foi mamoplastia redutora. A maioria dos
especializandos quer trabalhar em clínica privada.
Conclusão: Visando aprimorar a formação acadêmica, é necessário que os serviços
credenciados se adequem aos requisitos necessários para a boa formação dos
especializandos.
Palavras-chave: Cirurgia plástica; Educação continuada; Educação; Trabalho; Estética
INTRODUCTION
Recently, there has been much discussion about the training of plastic surgeons that have to choose between aesthetic and reconstructive surgery, and with the current market demands, most end up choosing aesthetic surgery. Unlike aesthetic plastic surgery, reconstructive plastic surgery aims at correcting congenital and/or acquired deformities (trauma, developmental changes, post-oncologic surgery, accidents, and others) and partial or total functional deficits where plastic surgery is required for treatment and is considered as necessary as any other surgical intervention1.
Given this scenario, one might assume that surgeons with experience in reconstructive surgery will be lacking in order to teach their residents, as Rohrich stated, “who will be the future educators as more and more of us are diverted to cosmetic surgery as soon as we form?” Thus, it is important to know the type of surgeries performed in the SBCP-accredited institutions and the surgical evolution of the final year students of the Specialization Course in Plastic Surgery of the Brazilian Society of Plastic Surgery (SBCP) to ensure that measures are taken for the future of the specialty.
OBJECTIVES
This study analyzed a questionnaire answered by plastic surgery trainees in their last year of the Specialization Course in Plastic Surgery of the SBCP, evaluated the quality of services and trainees, identified strengths and weaknesses of the course, and developed a profile of the research participants and their future interests. The study compared procedures in which the trainee feels less confident, the numbers of procedures performed during training, and the numbers necessary to gain confidence in performing them. In addition to describing the characteristics of the group, the study identified surgical areas that need additional training, trainee objectives after the course, and initiatives to modify the plastic surgery program.
METHODS
This was a retrospective, descriptive, cross-sectional study. The study evaluated questionnaires (Appendix 1) answered by plastic surgery trainees in their last year of the Specialization Course in Plastic Surgery of the SBCP, who attended the Brazilian Congress of Plastic Surgery in Belo Horizonte - Minas Gerais, held on November 11, 2015. The questionnaire consisted of 15 objective, closed qualitative questions for which responses were obtained from the participants; each question had sub-items, and confidentiality and anonymity were guaranteed.
The data from the questionnaire were collected, organized, and calculated using Excel. Relevant statistical calculations were then carried out using simple averages and percentages. Finally, the variables were analyzed and compared with published data, when available. A p value ≤0.05 using the student’s t-test was considered statistically significant.
Inclusion criteria
Partially or completely filled questionnaires answered by plastic surgery trainees in their last year of the Specialization Course in Plastic Surgery of the SBCP who attended the Brazilian Congress of Plastic Surgery in Belo Horizonte, Minas Gerais, in 2015 were included in this study. The questionnaire was based on a paper by Morrison et al.3 , and was adapted for Brazil.
Questionnaires answered by trainees enrolled in courses recognized by the Ministry of Education and Culture (MEC) and/or the SBCP were included.
RESULTS
A total of 230 questionnaires were distributed, out of which 113 (49.1%) were answered.
The respondents included 71 men (63%) and 41 women (37%) (Figure 1). Out of these, 34 indicated that their course was recognized by the SBCP, 75 responded that their course was recognized by the MEC and SBCP, and 4 respondents did not answer this question.

Most courses included training on aesthetic procedures (87.27%), with an average of 53.36% of purely aesthetic procedures compared to purely reparative surgery techniques (Figure 2).

The participants were asked whether they received training in specific areas that involve reparative surgery, with the results shown in Table 1.
| Procedure | Reconstruction of lower limbs | Pressure ulcers | Local flaps | Breast Recon-struction (TRAM/LD) |
|---|---|---|---|---|
| Yes | 70 (61.94%) | 85 (75.22%) | 101 (89.38%) | 98 (86.72%) |
| No | 43 (38.06%) | 28 (24.78%) | 12 (10.62%) | 15 (13.28%) |
| Total | 113 | 113 | 113 | 113 |

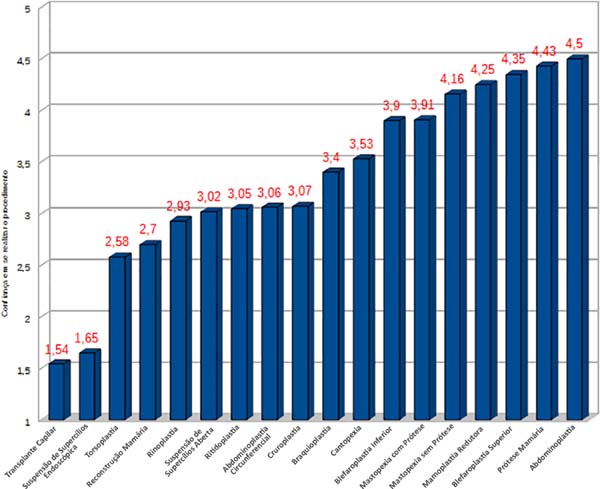
The results indicated that the trainees had the most confidence in performing an abdominoplasty, and the least confidence in performing a hair transplant (Figure 3), with 5 representing “very confident” and 1 representing no “confidence” levels.
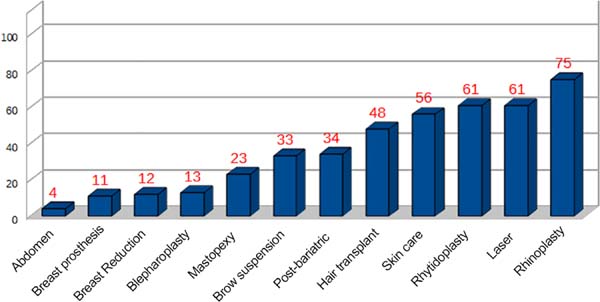
The area where the respondents indicated the most interest in deepening their knowledge and skills was rhinoplasty, followed by laser resurfacing techniques and rhytidoplasty (Figure 4).
The level of satisfaction with the training course was high; 41.07% of respondents were satisfied with the training, 22.34% were very satisfied, and only 3.57% were dissatisfied.
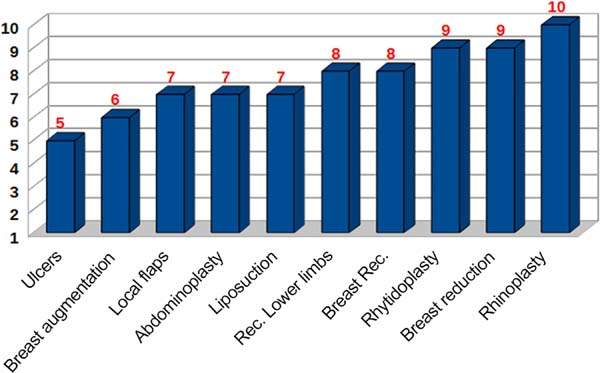
The number of procedures needed to develop confidence according to the trainee is shown in Figure 5.
The procedure performed most frequently during training was reduction mammoplasty, followed by local flaps. In contrast, lower limb reconstructions were performed with the least frequency (Figure 6).
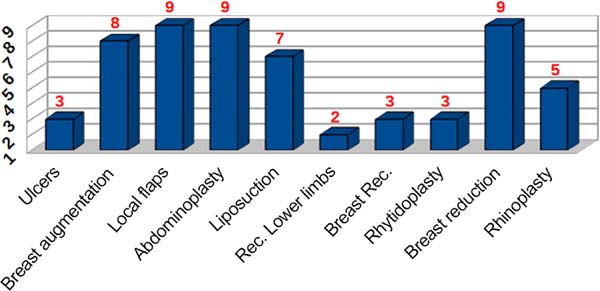
A comparison of the number of procedures considered necessary to perform a surgery with the actual number of procedures performed, including the p value, is shown in Table 2 (statistically significant differences are highlighted in red).
| Necessary | Performed | p value | |
|---|---|---|---|
| Pressure ulcers | 5 | 3 | 0.0011 |
| Breast augmenta-tion | 6 | 8 | 0.0125 |
| Local flaps | 7 | 9 | 0.0001 |
| Abdominoplasty | 7 | 9 | 0.0001 |
| Liposuction | 7 | 7 | 0.5731 |
| Rec. Lower limbs | 8 | 2 | 0.0001 |
| Breast Rec. | 8 | 3 | 0.0001 |
| Rhytidoplasty | 9 | 3 | 0.0001 |
| Breast reduction | 9 | 9 | 0.3670 |
| Rhinoplasty proce-dure | 10 | 5 | 0.0001 |

Most trainees claim to be prepared to perform aesthetic procedures, and none reported being not prepared, while only 4.6% reported being poorly prepared.
Working in a private clinic with a group of surgeons was the most frequently chosen option, followed by working in only a private clinic and academic institutions.
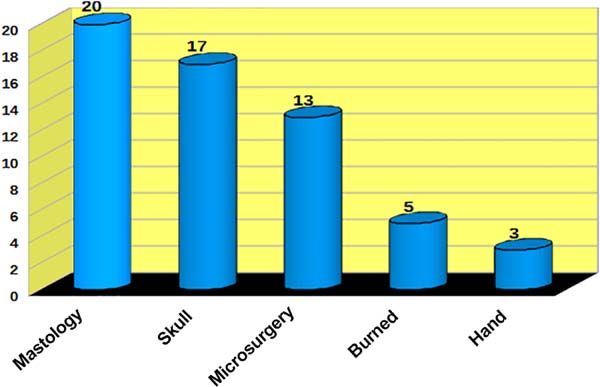
A fellowship was deemed to be necessary by 64.54% of the respondents, and the most desired subspecialties are shown in Figure 7.
DISCUSSION
The number of unanswered questionnaires reveals the level of disinterest of the trainees and their frustrations with their residency, and only those who were satisfied with their training answered the questionnaire4.
According to a study by Scheffer & Cassinote5, a culture of male hegemony is present in surgical fields. A paper published in 2012 revealed that out of a total of 4,012 plastic surgeons, 799 were female (19.9%) and 3,213 were male (80.1%), which was similar to our study, but with an increase in the number of female surgeons.
Most plastic surgery specialization courses are recognized by the MEC and by the SBCP.
In Brazil, medical specialization programs are regulated by Law Nº. 11.381 of December 1, 20066, by the Resolution of the National Commission of Medical Residency (CNRM) of May 17, 20067, and by the internal regulations of the Department of Education of Accredited Services of the Brazilian Society of Plastic Surgery (SBCP) 8.
The SBCP has 899 accredited areas of specialization which require 6 years of medical training, 2 years of specialization in general surgery and 3 years of training in plastic surgery.
The internal regulations of the Department of Education of Accredited Services (DESC) of the SBCP, 1997, consist of 23 articles, which cover the areas necessary to learn about the specialty, including the following:
a. Inpatient unit: 10% of the minimum annual workload;
b. Outpatient: 15% of the minimum annual workload;
c. Surgical center: 30% of the minimum annual workload;
d. Emergency: 15% of the minimum annual workload;
e. Mandatory internships: cranio-maxillo-facial surgery, hand surgery, burns unit, orthopedics and traumatology, dermatological surgery and mastology;
f. Optional internships: dermatology, surgical technique and microsurgery, medical psychology, hematology, ophthalmology and otorhinolaryngology;
g. The PRM must offer a minimum of 85% of reparative surgeries and a maximum of 15% of solely aesthetic surgeries.
Thus, training for aesthetic procedures is included in the regulations for medical specialization courses in plastic surgery, which must contain at least 85% of reparative surgeries and a maximum of 15% of solely aesthetic surgeries.
Most hospitals that focus on reparative surgery (reference hospitals for the treatment of tumor sequelae, burns, and congenital malformations) train their residents in aesthetics through mandatory internships in other services, for which the resident undergoes training in all the areas of plastic surgery, according to the DESC regulations. However, the responses of the trainees indicate that there are deficiencies in the system, which may be explained by the lack of supervision of internships or even the lack of completion of these internships. The same occurs with training focused on cosmetic surgery, and residents have to train in reparative areas through internships in reconstructive surgery. Another point that should be noted is the diversity in the type of surgeries performed during training in plastic surgery, which, given this scenario, may lead to training with greater emphasis on aesthetic or reconstructive surgery.
Some associations such as the SBCP have standards for the accreditation of institutions offering post-graduate courses. The criteria for accreditation are varied; there are special rules for each. Some associations have criteria that may be even more stringent than those of the MEC itself, for example, annual evaluations of institutions, while the MEC makes 5-year assessments to obtain reaccreditation.
The lack of training for reconstruction of limbs, breast reconstruction, local flaps, and treatment of pressure ulcers seems unacceptable in a plastic surgery course, since the practice of a plastic surgeon involves these surgeries, which indicates a serious deficiency. Wong et al10 reported that there is a lack of surgical practice among plastic surgeons in the United Kingdom. The authors made suggestions to improve current teaching practices, including curriculum changes and demonstrations, which are considered important, but insufficient, because the practice develops with participation in decision-making and action in the operative field.
The level of confidence in performing procedures can be explained by the large number of patients who seek treatment. The procedures with a lower level of trust involve low demand, and a lack of professionals with the knowledge and skills specific to teaching, in addition to the high cost of materials required.
An interest in increasing knowledge in areas that involve aesthetic procedures (skin care, laser resurfacing, rhinoplasty) corroborates the fact that more trainees have lost interest in reconstructive surgery and are interested in working in private clinics. In a study conducted by the American Society of Plastic Surgery, 1,250 plastic surgeons stated that the number of reparative plastic surgeries has decreased over the past 10 years, as a result of personal choice and the increase in competition with other surgical areas11.
The level of satisfaction with the courses was high, which may be related to the number of procedures performed, and with their expectations, as well as the perception of the ability to perform aesthetic procedures.
A low demand was observed for some procedures, which may reflect the fear of the professionals and restrict their area of activity. Some procedures are left aside not because of a lack of interest but due to a lack of dedication to the area of activity.
In the United States of America, the specialization committee of the Medical Educational Accreditation Board has established a minimum number of cosmetic procedures to be taught in specialization programs, which includes 10 augmentation mammoplasties, 7 face lifts, 8 blepharoplasties, 6 rhinoplasties, 5 abdominoplasties, 10 liposuction procedures, and 9 other cosmetic procedures, without differentiating between reconstructive and aesthetic procedures12.
The average number of surgeries performed by the trainees from Brazil is within these parameters, which is similar to the results in a study by Morrison et al.3, in which the trainees from the United States were asked about their training and the number of procedures they would need to develop confidence. There is a constant deficit in the number of plastic reconstructive surgeons in Brazil, since many are directed only to cosmetic surgery, which reflects the current profile of trainees. These characteristics are easily identified in academics and medical fellows by superficial and fragmented knowledge, lack of interest due to the high complexity, allure of salary and quality of early life, as well as individual thought and others13.
CONCLUSION
As discussed, it is important that the institutions accredited by the SBCP be aware of the type of surgeries performed, so that they can adapt and maintain a good level of training in the areas of reconstructive and aesthetic surgery. Consideration should be given to the difficulties encountered in the financing of such services, especially for the institutions that primarily serve SUS patients, as well as the qualifications and dedication of the teaching staff. An increase in the number of professionals from other medical specialties performing procedures that were once performed only by plastic surgeons is evidence that this specialty is being diluted and is losing space. Superior training courses with specialists will guarantee the future of the practice of aesthetic and restorative plastic surgery.
COLLABORATIONS
|
RLV |
Analysis and/or data interpretation, conception and design study, data curation, formal analysis, investigation, methodology, project administration, writing - original draft preparation, writing - review & editing. |
|
CJB |
Analysis and/or data interpretation, data curation, formal analysis, investigation, realization of operations and/or trials, supervision, validation, writing - review & editing. |
|
FP |
Resources, visualization, writing - original draft preparation, writing - review & editing. |
REFERENCES
1. Brasil. Ministério da Saúde. Atenção Especializada e Hospitalar. [acesso 2019 Fev 12]. Disponível em: http://portalms.saude.gov.br/atencao-especializada-e-hospitalar
2. Rohrich RJ. Training the next generation of plastic surgeons: a lesson from geese. Plast Reconstr Surg. 2000;106(5):1125-6. PMID: 11039384 DOI: https://doi.org/10.1097/00006534-200010000-00023
3. Morrison CM, Rotemberg SC, Moreira-Gonzalez A, Zins JE. A survey of cosmetic surgery training in plastic surgery programs in the United States. Plast Reconstr Surg. 2008;122(5):1570-8. PMID: 18971742 DOI: https://doi.org/10.1097/PRS.0b013e318188247b
4. Xavier AP. Uma visão antropológica da aplicação de questionários na pesquisa em educação. Educ Rev. 2012;44:293-307. DOI: https://doi.org/10.1590/S0104-40602012000200018
5. Scheffer MC, Cassinote AJF. A Feminização da medicina no Brasil. Rev Bioét. 2013;21(2):268-77
6. Brasil. Presidência da República. Lei No11.381, de 1º de dezembro de 2006. Altera a Lei no 6.932, de 7 de julho de 1981, que dispõe sobre as atividades do médico residente, e revoga dispositivos da Lei no 10.405, de 9 de janeiro de 2002. Brasília: Presidência da República; 2006. Disponível em: http://www.planalto.gov.br/ccivil_03/_Ato2004-2006/2006/Lei/L11381.htm
7. Brasil. Comissão Nacional de Médicos Residentes. Disponível em: http://portal.mec.gov.br/residencias-em-saude/residencia-medica PMID: 26510389
8. Brasil. Sociedade Brasileira de Cirurgia Plástica. RRegulamento interno disponível em área privada aos membros da SBCP. Disponível em: http://www2.cirurgiaplastica.org.br/images/Docs/regimentos/regimento_DESC.pdf
9. Sociedade Brasileira de Cirurgia Plástica. Serviços Credenciados. [acesso 2019 Fev 12]. Disponível em: http://www2.cirurgiaplastica.org.br/sbcp/servicos-credenciados
10. Wong M, Jones S, Sheikh H, James N. The effect of the new deal on the operative experience of plastic surgical SHOs. J Plast Reconstr Aesthet Surg. 2006;59(3):311-2. PMID: 16673549 DOI: https://doi.org/10.1016/j.bjps.2005.09.009
11. Pinder RM, Urso-Baiarda F, Knight SL. Decades of change in plastic surgery training. J Plast Reconstr Aesthet Surg. 2010;63(8):e662-3. DOI: https://doi.org/10.1016/j.bjps.2010.01.037
12. Accreditation Council for Graduate Medical Education. Case Log System. Data Collections. Chicago: Accreditation Council for Graduate Medical Education. Disponível em: http://www.acgme.org
13. Cunha MS. Ensino da Cirurgia Plástica e a nova geração; para refletir. Rev Bras Cir Plást. 2013;28(4):529-30.
1. Hospital Municipal Barata Ribeiro, Rio de Janeiro, RJ, Brazil.
2. Universidade Federal Fluminense, Niterói, RJ, Brazil.
Corresponding author: Ricardo Luis Vanz Rua Fagundes Varela, 305, Ingá, Niterói, RJ, Brazil. Zip Code: 24210-520. E-mail: ricardovanz@gmail.com
Article received: August 09, 2018.
Article accepted: April 21, 2019.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket