



Articles - Year 1998 - Volume 13 -
Otoperichondrioplasty - Update of Technique
Oto-Pericondrioplastia - Atualização de Técnica
ABSTRACT
There are many techniques that aim to correct lop ear, a very common deformity. All of them seek to correct the scapho-conchal angle and to reduce the conchal portion size, positioning the free border of the auricle uniformaly regarding its incision into the skull. Our technique was first published in 1969, and its originality consisted in the detachment of the posterior perichondrium from the ear cartilage. Based on Ely, McEvitt and Luckett's principles four meridian incisions were performed in order to obtan 3 strips that, once superposed, created a rounded shape anthelix. By shortening the perichondrium, it was possible to maintain the new angle because the cartilaginous memory had been broken by such incisions. Nowadays, advances in surgical equipment (detacher and special abrasive scratches for the auricle) the technique was simplified by the abolishment of the cartilaginous strips. Using an auricle detacher we create a tunnel in the posterior face of the cartilage along the entire stretch of the anthelix. Through a small incision in the cartilage the scratcher is introduced performing debridement maneuvers in the anterior face of the cartilage to break its memory. As in the previous technique, the posterior perichondrium of the ear was properly detached; by suturing with absorbable stitches it is possible to shorten the perichondrium maintaining the ortho-positioning of the anthelix in the entire extent of the auricle: upper pole, medium portion and lobule.
Keywords:
RESUMO
Existem várias técnicas para correção da orelha em abano, deformidade bastante comum em nosso meio. Todas elas visam corriqir o ângulo escafo-conchal, além de diminuir o tamanho da concha, posicionando a borda livre do pavilhão auricular de maneira uniforme em relação à sua implantação no crânio. Em 1969 publicamos nossa conduta, cuja originalidade era aquela de se descolar o pericôndrio posterior da cartilagem auricular. Baseados nos princípios de Ely, McEvitt e Luckett, fazíamos 4 incisões longitudinais na cartilagem, a fim de obter 3 tiras que, uma vez superpostas, permitiam uma anti-hélix com aspecto arredondado. Fazendo-se o encurtamento do pericôndrio, conseguia-se manter o novo ângulo, já que a mola da cartilagem havia sido quebrada pelas incisões. Atualmente, com o desenvolvimento de instrumental apropriado (descoladores e raspas abrasivas especiais para pavilhão auricular) simplificamos nossa conduta, passando a abolir as tiras cartilaginosas. Utilizando-se o descolador de pavilhão, fazemos um túnel na face anterior da cartilagem, em todo o trajeto da anti-hélix que se pretende moldar. Por uma pequena incisão na cartilagem, introduz-se a raspa, fazendo manobras de desbastamento da face anterior da cartilagem, de maneira a quebrar a referida mola. Como na técnica anterior; o pericôndrio posterior da orelha foi devidamente descolado; fazendo sutura com fio absorvível, encurtamos o pericôndrio, mantendo, dessa maneira, o ortoposicionamento da anti-hélix em toda a extensão do pavilhão auricular: pólo superior, parte média e lóbulo da orelha. Os resultados são bastante naturais e a técnica ficou muito simplificada.
Palavras-chave:
Lop ear is a deformity that arises from an abnormal development of the auricle, being characterized by many anatomostructural changes, among which:
1. Increase of the scapho-conchal angle.
2. Erasing of the anthelix.
3. Repellence of the auricle free border of the skull.
4. Increase of the conchal portion.
Aesthetical surgery for this deformity was first reported in the XIX Century. In 1845 Dieffenbach(lO) preconized the correction of this deformity simply by the excision of the retroauricular skin. Ely(14) in 1881, Monks(23) in 1891 and Cocherill(6) in 1894 recognized that the cartilaginous conchal portion should be excised, as published by Morestin(24) in 1903 and Lucktt(22) in 1910, who firstly paid attention to the scapho-conchal angle, considering it the main element in the correction of the deformed auricle.
Later, Baxter(2) in 1942 , McEvitt(25) in 1947 and Barsky(1) in 1938 improved the principles established by Luckett. More recently Converse(7, 8) in 1938, Tanzer(39), Mustardé(27, 28) and Sperli(33, 34) in 1969 introduced modifications in their own techniques with great contribution to the treatment of the lop ear.
TECHNICAL COMMENTS
Modern techniques, as far as properly employed, have satisfactory results. However, not all of them cover all the essential needs for the correction.
Note that:
-Few techniques intend to dissect and front the anatomical elements.
-The anthelix shape is not always satisfactory.
-Little attention has been paid to the orthopedic maintenance of the scapho-conchal angle.
-Relapse is not uncommon.
-Unsatisfactory results, in most extreme cases, lead to secondary deformities such as "earphone", where the upper pole and the lobule remain distant from the skull, as long as the auricle's medium portion approaches.
-The retroauricular sulcus may be wiped out due to excessive skin removal.
-In a few techniques, in which strings are left transfixed in the cartilage, there may be relapse by the section of the cartilage due to its excessive traction.
-In some cases we can find chondritis caused by the presence of stitches in the cartilage. However, this is a transitory complication.
PREVIOUS CONDUCT
After an extensive bibliographic review we looked forward to applying certain basic principles of surgical technique and mechanics to employ a technique that has been employed in our service for 26 years with a long term follow-up.
The original technique (Fig. 1) consisted of classical ear surgery principles and the following additions:

Fig. 1 - Marking details and surgical steps of our previous technique.
1. The anthelix is marked in the anterior face of the auricle using methylene blue or green stain pen.
2. Marking of the skin meridian at the retroauricular sulcus. It can be as long as necessary.
3. Incision of the previously marked auricle's posterior skin (meridian).
4. Removal of the meridian by means of a thin skin layer.
5. Placement of needles through the auricle according to the previous marking of the anthelix.
6. The points of the transfixed needles are drenched with methylene blue or green stain pen. The needles are removed through the anterior face of the auricle. This maneuver transfers the ink into the structure of the perichondrium and cartilage.
7. Incision of the perichondrium until it reaches the cartilage, along the meridian area marked with the stain.
8. Detachment of the posterior perichondrium from the auricle, exposing the neat cartilage.
9. Four meridian incisions are made in the cartilage, parallel to the marking. With this we obtain three cartilaginous strips, measuring 2 mm wide each.
10. Removal of the cartilaginous conchal portion, starting at the limit of the last interna incision. This meridian must be as wide a necessary.
11. Double breasted suture of the perichondrium, shortening it as necessary. The auricle must be in its definitive position.
12. Skin suture, with special attention to embed the suture in the auriculotemporal angle to avoid erasing of the retroauricular sulcus.
13. Placement of a thin layer of plaster, contouring the anterior face of the auricle and just passing by its border to the posterior face.
PRESENT CONDUCT
Considering the recent evolution of surgical instruments and the refinements of micro-abrasives, we decided to abolish the confection of cartilaginous strips in benefit of the slender of the cartilage in the entire extent of the anthelix.
These factors allowed an important simplification in the technique as follows:
1. Anthelix is marked in the anterior face of the auricle using methylene blue or stain pen (Fig. 3).
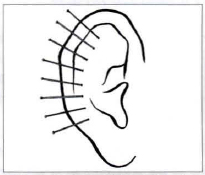
Fig. 3 - Scheme illustrating the marking of the anthelix in the anterior face of the auricle, with transfixing of the needles to the posterior face.
2. Skin meridians are marked at the height of the retroauricular sulcus, being wider or thinner as necessary (Fig. 4).

Fig. 4 - Marking of the posterior skin meridian of the auricle (scheme).
3. Incision of the previously marked posterior skin meridian.
4. Removal of the skin meridian.
5. Placement of needles transfixing the auricle, according to the anterior marking of the anthelix (Fig. 5).

Fig. 5 - Needles transfix the ear through its posterior face allowing the projection of the anterior face marking into the cartilaginous and perichondrial planes.
6. The points of the transfixed needles are drenched with methylene blue or green stain pen. The needles are removed through the anterior face of the auricle.
This maneuver transfers the ink into the structure of the perichondrium and cartilage.
7. Incision of the perichondrium until it reaches the cartilage, along the meridian area marked with the coloring (Fig. 6).
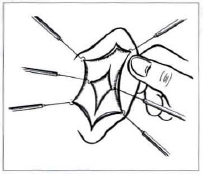
Fig. 6 - Schematic representation of the perichondrial incision until it reaches the cartilaginous plane.
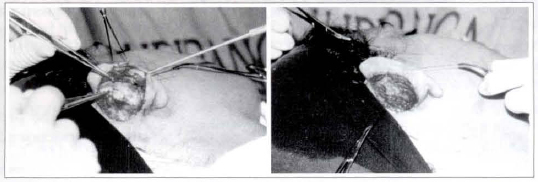
8. Detachment of the posterior perichondrium from the auricle, exposing the neat cartilage (Fig. 7).
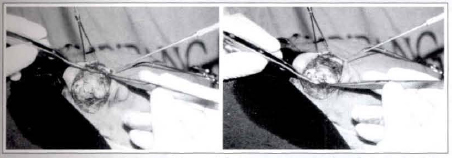
Figs. 7a & 7b - Detachment of the auricle's posterior perichondrium, showing the neat cartilage.
9. Detachment of the cartilage from the anterior skin of the auricle, measuring approximately 8 mm wide. Use an appropriate cartilage detacher (Fig. 8).
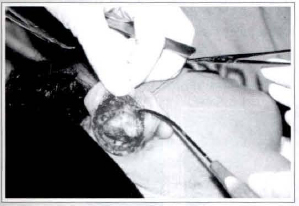
Fig. 8 - Detachment of the anterior cartilaginous plane of the ear. Approximately 8 mm wide, using an appropriate cartilage detacher.
10. Scratching of the anterior face of the cartilage, along the entire marked region. Use a special ear cartilage rasp (Fig. 9).
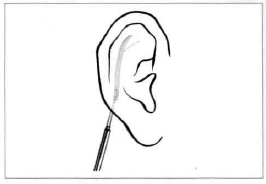
Fig. 9a - Scheme of the scratching of the anterior face of the auricular cartilage aiming to weaken and "break" the cartilaginous memory.

Fig. 9b . Scratching of the cartilaginous anterior face in the entire marked region.
11. Removal of the cartilaginous conchal portion meridian when necessary.
12. Double breasted suture of the perichondrium to shorten it whenever necessary. The auricle is now placed in its definitive position (Figs. lOa & lOb).
Figs. lOa & 10b . Double breasted suture of the ear posterior perichondrium in order to shorten the perichondrium, positioning the auricle in its definitive position and keeping the scapha-conchal angle corrected. Final suture of the shortened retroauricular perichondrium.
13. Skin suture.
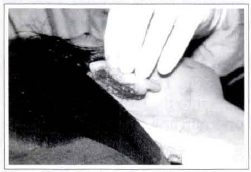
Fig. lla - Repositioning of the corrected auricle.

Fig. 11b - Normal stabilization of the auricle.
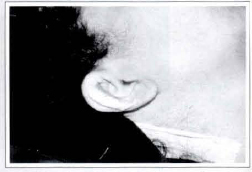
Fig. llc· Semi-compressive curative with gauze support.
DISCUSSION
The adequate skin removal preserving the perichondrial plane propitiates the detachment of a thick perichondrium that once shortened will keep the auricle in its new position.
The detachment of the perichondrium is very easy and must be performed with a delicate scalpel or scissors to an extent necessary to free the posterior face of the cartilage.
Then a 5 mm incision is made in the marking of the future anthelix. Through this incision the anterior face of the cartilage is detached using an auricular detacher.
Once detached, the entire extent of the anterior cartilage is scratched to be separated from the perichondrium and thinned enough in order to weaken the cartilaginous memory.
The removal of the cartilaginous conchal portionwhich may be as wide as necessary - aims to avoid the projection of the conchal portion beyond the desired limit, as it may happen in acute cases. Besides that, its shape may vary in order to correct a prominent position of the lobule that is fixed exclusively by the excess of conchal cartilage. We must never try to approach the lobule to the skull through the removal of its skin and soft tissues.
We reinforce that the determining factor for the projection of the lobule is the excess of the lower conchal portion.
When the perichondrium is double breasted sutured, the desired scapho-conchal angle is immediately achieved. In this step it is possible to balance the distantness of the auricle from the mastoidal region in three portions: upper pole, medium portion and lobule.
Poliglycolic acid absorbable string or catgut may be used. Only the perichondrium is sutured, in a double breasted shape. The cartilage is never sutured.
Late results are persistent and lop ear has not relapsed.

Figs. 12a & 12b - Patient 1: Anterior view, pre and postoperative.
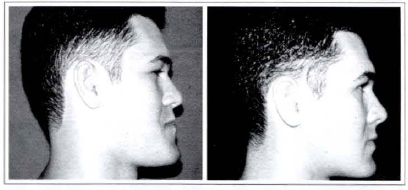
Figs. 12c & 12d - Patient 1: Profile view, pre and postoperative.
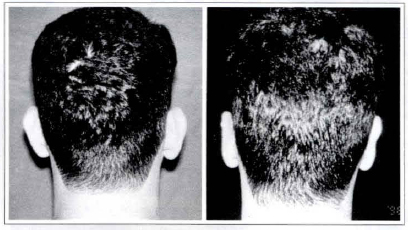
Figs. 12c & 12f - Patient 1: Posterior close-up view, pre and postoperative.
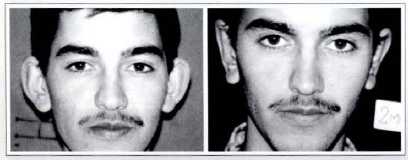
Figs. 13a & 13b - Patient 2: Anterior view, pre and postoperative.
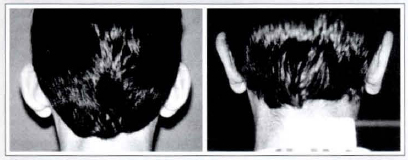
Figs. 13c & 13d - Patient 2: Posterior view, pre and postoperative.
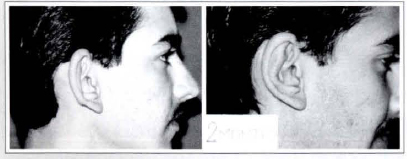
Figs. 13e & 13f - Patient 2: Profile close-up view, pre and postoperative.
CONCLUSION
In order to correct the scapho-conchal angle (anthelix) by means of the weakening of the cartilaginous memory and willing to reconstmct a normal anthelix - with rounded borders and no relapse - six new principles were added to the technique to enable good results without much difficulties, as follows:
1. The future anthelix is marked using needles to transfix the auricle from its anterior to the posterior face.
2. Marking of the future anthelix in the posterior face. Incision of the perichondrium onto this marking.
3. Detachment of the posterior face perichondrium from the cartilage.
4. Slenderness of the cartilage in its anterior face through scratching.
5. Removal of the cartilaginous conchal portion whenever necessary.
6. Double breasted suture of the perichondrium in order to shorten and achieve the desired scapho-conchal angle.
This Technique aims to execute the basic principles of surgery in which anatomical elements must be properly dissected and fronted.
REFERENCES
1. BARSKY AJ. Plastic Surgery. Philadelphia: W. B. Saunders Company, 1938. p.178.
2. BAXTER H. Plastic correction of protruding ear in children. Canad. Med. Ass. J. 1941; 45:217.
3. BECKER JO. Correction of the protruding deformed ear. Br. J. Plast. Surg. 1952; 5:187.
4. BECKER JO. Surgical correction of the abnormally protruding ear. Arch. Otolaryntol. 1949; 50:541.
5. CLOUTIER A. Correction of outstanding ears. Plast. Reconstr. Surg. 1961; 28:412.
6. COCHERIL RC. Essai sur la restauration du pavillon de l'oreille. Thèse pour le Doctorat en Médicine. Lille, L. Danel, 1894.
7. CONVERSE JM, NIGRO A, WILSON AA, JOHNSON M. A technique for surgical correction of lop ears. Plast. Reconstr. Surg. 1955; 15:411-418.
8. CONVERSE JM, WOOD-SMITH D. Technical details in the surgical correction of the lop ears deformity. Plast. Reconstr. Surg. 1963; 31:118.
9. CRICKELAIR GF, COSMAN B. Another solution for the problem of the prominent car. Alan. Surg. 1964; 100:314-324.
10. DIEFFENBACH JF. Die operative chirurgie. Leipzig: F.A. Brockhaus, 1845.
11. DAVIS JS, KITLOWSKI EA. Abnormal prominence of the ears: A method of readjustment. Surgery. 1937; 2:835.
12. DURNAS DW. Correction of prominent ears by concha-mastoid sutures. Plast. Reconstr. Surg. 1968; 42:189-193.
13. ERICH JB. Surgical correction of protruding ears. Proc. Staft Meet. Mayo Clin. 1958; 33:99-104.
14. ELY ET. An operation for prominence of the auricles. Arch. Otology. 1881; 10:97.
15. FARINA R, RICARDO B, GOLCMN B, DE CASTRO O. Otoplasty. Br. J. Plast. Surg. 1962; 15:385.
16. GONZALES-ULLOA M. An easy method to correct prominent ears. Br. J. Plast. Surg. 1952; 4:207.
17. JU DMC, Ll C, CRICKELAIR GE The surgical correction of protruding ears. Plast. Reconstr. Surg. 1963; 32:283.
18. JOSEPH J. Eselsohren. Verhandl der Bul Med. Gesellsch 1896. p.206.
19. KAYE BL. A simplified method for correcting the prominent ear. Plast. Reconstr. Surg. 1967; 40:40-48.
20. KEEN WW. New method of operating for relief of deformity due to protruding ears. Ann. Surg. 1890; 12:49.
21. KITLOWSKI EA. Correction of prominent ars. Plast. Reconstr. Surg. 1959; 23:374.
22. LUCKETT WH. A new operation for prominent ears based on the anatomy of the deformity. Surg. Gynec. Obst. 1910; 10:635-637.
23. MONKS GH. Operation forcorrectingdeformiry due ro prominent ears. Bostolt Merl. Sltrg.J. 1891; 124:84.
24. MORESTIN H. De la reposition et do plissement. cosmetiques du palillon de ltoreille. Rev. Orthop. 1891; 4.
25. MC-EVITT WG. The problem of the protruding ear. Plast. Reconstr. Surg. 1947; 2:481.
26. Mc DOWELL AJ. Goals in otoplasty for protruding ears. Plast. Reconstr. Surg. 1908; 41:17-27.
27. MUSTARDE JC. The treatment of prominent ears by buried mattress sutures: a ten year survey. Plast. Reconstr. Surg. 1967; 39:382.
28. MUSTARDE JC. Correction of prominent ears using simple mattress sutures. Br. J. Plast. Surg. 1963; 10:170-176.
29. PIERCE GW, KLABUNDE EH, GERGERON VL. Useful procedures in plastic surgery. Plast. Liz. Reconstr. Surg. 1947; 2:358.
30. ROGERS BO. Ely's 1881 operation for correction of protruding ears. A medical "first". Plast. Reconstr. Surg. 1968; 42:584-586.
31. ROGERS BO. The historical evolution of plastic and reconstructive surgery, in nursing care of the plastic surgery patient. Edited by Wood-Smith and P. C. Porowsky. St. Louis: Mosby Co, 1967. p. 4.
32. ROGERS BO. The first one hundred years of Manhattan Eye, Ear and Throat Hospital in Centennial Symposium: Manhattan Eye, Ear & Throat Hospital, New York: Wondhaven Press, 1968. p. 11-26.
33. SPERLI AE. Surgical treatment of the prominent ear. Rev. Latino-Americana. de Cirugia Plastic 1969; III:3-16.
34. SPERLI AE. Otoplastia estética. Revista do Colég Brasileiro de Cirurgiões. 1971; 2:86-90
35. STARK RB, SAUNDERS DE. Natural appea ance restored to the unduly prominent ear. Br. Plast. Surg. 1962; 15:385-397.
36. STENSTRON SJ. Natural technique for corretion of congenitally prominent ears. Plast. Reconstr. Surg. 1963; 32:509-518.
37. STRAITH RE. Anthelix reconstruction in the protruding ear problem. Plast. Reconstr. Surg. 195: 12:454.
38. STRAITH RE. Correction of the protmding ear Plast. Reconstr. Surg. 1959; 24:277.
39. TANZER RC. The correction of prominent ear Plast. Reconstr. Surg. 1962; 30:236.
I - Assistant Professor, Department of Surgery of Santa Casa de São Paulo. Head Professor of the residency program of Serviços Integrados de Cirurgia Plástica - Hospital Ipiranga São Paulo, Brazil.
Address for correspondence:
Aymar E. Sperli, MD
Av. Cidade Jardim, 993 01453-000 - São Paulo - SP Brazil
Phone: (55 ll) 820-1279 - Fax: (55 11) 820-3792
e-mail: sperli@imedical.com
Work performed at Serviços Integrados de Cirurgia Plastica. Official Residency Program in Plastic Surgery - MEC-SBCP. Hospital Ipiranga, São Paulo, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket