



Articles - Year 1999 - Volume 14 - Issue 1
Non-surgical Treatment of Neonate Ear Deformities
Deformidades Congênitas da Orelha - Tratamento Conservador do Recém-Nascido
ABSTRACT
Genetic or mechanical ear deformities - except microtias - can be treated by a conservative approach in the first 72 hours of life by means of the ear's anatomical modeling with hydrophilic cotton (a low cost material) and fixation with micropore adhesive tape for 10 to 21 days. In this stage the level of maternal estrogen in the neonate circulation reduces quickly, allowing a natural hardening of the cartilage to its permanent shape.
Keywords: Deformity; molding; estrogen; neonate.
RESUMO
As deformidades congênitas da orelha, exceto as microtias, de causa genética ou mecânica, podem ser tratadas conservadoramente nas primeiras 72 horas de vida, por meio de modelagem anatômica, com material moldável de baixo custo (algodão hidrófilo) e fixação por fita adesiva tipo micro pore, que deve permanecer por um período de 10 a 21 dias. Nesta fase, os níveis de estrogênio materno circulante no recém-nascido diminuem rapidamente, permitindo que as cartilagens adquiram seu enrijecimento natural. Assim, a nova arma auricular obtida por modelagem tende a permanecer em caráter definitivo.
Palavras-chave: Deformidades; moldagem; estrogênio; recém-nascido (R.N.)
In the fetus' prenatal period its cartilages, ligaments, and connective tissue are relaxed by the estrogen, in order to facilitate the passage through the parturition channel. By this time, the ear's congenital deformities may arise from abnormalities in the morphogenesis or could be a result of the external pressure or malposed fetus. These malformations will be definitive as the level of circulating estrogen decreases, leading to the hardening of the cartilages as reported by Matsuo(l) in 1982 (Table I) and Forst(2) in 1986.

Whenever it's possible to conservatively intercede in the first 3 days of life by means of a molding plaster, the deformities may be permanently corrected.
MATERIAL & METHODS
The study started with 31 children being treated in 1984 in the baby ward of Hospital Felicio Rocho's maternity, in Belo Horizonte, Brazil. In 1986 another 31 children were treated in Santa Casa de Misericórdia Hospital in Juiz de Fora, Brazil.
All 62 cases were examined by a pediatrician and no other congenital deformities were reported. It was possible to identify six different kinds of isolate/associate and unilateral/bilateral deformities after the examination of the children's ears. A total of 133 deformities were treated.
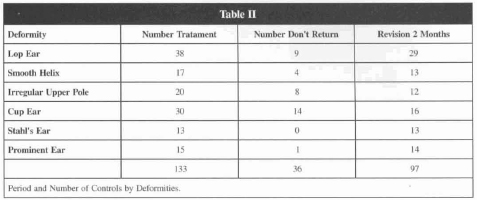
Two months later, 39 children with a total of 97 deformities returned for revision. It was possible to observe a favorable evolution regarding the anatomical shape of the ears in this short follow-up (Table II).
Twenty children totalling 46 deformities were examined in a late follow-up, from 1990 to 1993, with ages ranging from 4 to 9 years old. The correction was considered favorable.
CHOSEN METHOD
Once identified the deformity, the child's family was advised to use the conservative treatment. After authorized, the neonate was photographed and the ears were molded utilizing Hoffmann solution (equal parts of alcohol and ether) in order to degrease the skin and Benjoin tint to help the fixation of the adhesive tape (Fig. 1).

Fig. 1 - Materials utilized.
a) Small hydrophilic cotton rolls embedded in water or saline solution.
b) The anterior (external) and posterior (internal) sulcus are molded by apposing the compressed cotton, allowing an anatomical conformation to the ear (Fig 2).

Fig. 2 -Molding of the ear.
c) The mold is fixed with small micropore strips (Fig. 3).

Fig. 3 - Fixation of the mold with micropore strips.
d) The plaster is reinforced with wider strips in the surrounding skin, in order to fix the ear in its new position (Fig. 4).

Fig. 4 - The molding is reinforced with wide strips of micropore tape.
The plasters were made within the first 72 hours of life and were kept for a preriod that ranged from 10 days in minor defects to 21 days in more severe cases.
STATISTICAL EVALUATION
In a 2 months follow-up it was possible to review 39 cases (with 97 defects) out of 62 (with 133 defects). The high incidence of deformities is explained by the bilaterallity in most cases and for the existence of more than one kind of deformity in the same ear, in other cases.
For better evaluation of the results, all cases were divided into 4 groups: Excelent, Good, Regular and Fair, according to the kind of deformity (Table III).
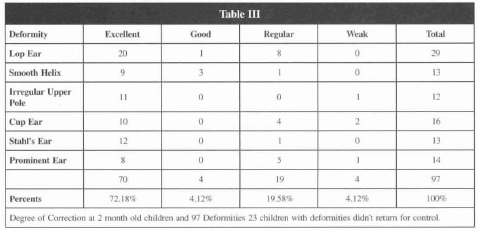
It is important to notice that an expressive group (72.18%) was ranked Excelent.
In a late follow-up (more than 4 years later) it was possible to verify that out of 39 cases examined 2 months postoperative, 20 were reexamined. The Excellent group remained at 73.91 % of the cases, as shown in Table IV.
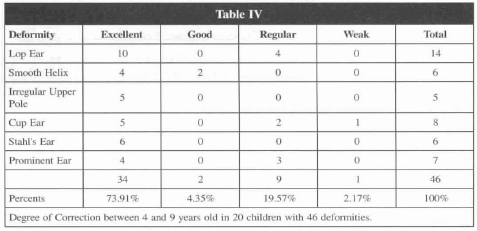

Fig. 5 - Neonate of V G., born in 8/31/84 with familiar antecedents. Presented left lop ear treated at 63 hours of life. Plasters were kept for 21 days, with an Excelent degree of correction.

Fig. 6 - Neonate of M. C. S. P. S. born in 9/9/1984 without familiar antecedents. Presented lop ear. Plaster made with 28 hours of life and kept for 21 days. Excellent degree of correction.

Fig. 7 - Neonate of J. N. M. born in 7/21/1986 without familiar antecedents. Presented unilateral Stahl's ear. Plaster made at 63 hours of life and kept for 10 days. Excelent degree of correction.

Fig. 8 - Neonate of C. I. A., born in 7/15/1986. Presented left lop and cup ear; right lop ear. Treated at 72 hours of life. Plasters were kept for 21 days. Four years postoperative.
CONCLUSION
The proposed method proved to be very simple to be performed, with efficient results as long as employed in the first 72 hours of life.
62 cases were treated, in a total of l33 congenital auricular deformities. In a 2 month follow-up, 39 cases (97 defects) were reviewed.
72.18% of these were considered Excellent. 20 children (46 defects) were evaluated from 4 to 9 years postoperative. The ratio of Excellent results remained unchanged (73.91%), meaning a definitive correction.
Due to the efficiency and facility of this method, it should be divulged to professionals in the hospitals' nurseries, in order to make this preventive approach a reality and thus to avoid a more traumatic surgical correction in the future.
REFERENCES
1. MATSUO K, HIROSE T, TOMONO T, TWASAWA M, KATOHDA S, TAKAHASHI N, KOH B. Nonsurgical Correction of Congenital Auricular Deformities in the Early Neonate: A preliminary report. Plast. Reconstr. Surg. 1984; 73: 385l.
2. BROWN FE, COLEN LB, ADDANTE RR, GRAHAM JM, Jr SCD. Correction of Congenital Auricul. Deformities by Splinting in the Neonatal Period. Pediatrics. 1986; 78:406-411.
3. THOMAS L. Reversible collapse rabbit ears after intravenous papain and prevention of recovery by cortisone. J. Exp. Med. 1956; 104:245.
4. HIROSE T, TOMONO T, YAMANOTOK. Nonsurgical correction for cryptotia using simple apparatus. In J. Fonseca (Ed), Transaction of the 7th International Congress of Plastic Reconstr. Surg. 1979; 353-354.
5. SHELDON H , ROBINSON A. Sructies on cartilage: II Electron microscopic observations on rabbit ear cartilage following the administration of papain. J. Biophys. Biochem. Cytrol. 1960; 8:151.
6. WEISSKOPF A, BURN HF, SCHOENHOLZ WK. Protective action of estrongen against streptococcal infection in mice and its relation to connective tissue. Laryngoscope. 1961; 71:788.
7. KENNY FM, ANGSUSINGHA K, STINSON D, HOTCHIKISS J. Unconjugated estrongens in the perinatal period. Pediatr. Res. 1973; 7:826.
8. WINTER JSD, HUGHES LA, REYES FI, FAIMAN C. Piruitary gonadal relations in infancy: 2. Patterns os serum gonadal steroid concentration in man from birth to two years of age. J. Clin. Endocrinol. Metab. 1976, 42:679.
9. HASCALL VC, HEINEGARD D. Aggregation of Cartilage Proteoglycans I. The role of hyaluronic acid. The G. of Biolog. Chemistry. 1974; 249:4232-4241.
I - Titular Member of the SBCP.
Address for correspondence:
Édina Márcia Zinato Respeita, MD
R. Dom Viçoso, 20
36026-390 - Juiz de Fora - MG Brazil
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket