



Case Report - Year 2018 - Volume 33 -
Simultaneous treatment of sacral and ischial pressure ulcers with a single flap: case presentation
Tratamento simultâneo de úlceras de pressão sacral e isquiática com retalho único: apresentação de um caso
ABSTRACT
Pressure ulcers are alterations of the integrity of the skin and underlying tissues, caused by pressure, more commonly on bony prominences, especially in areas devoid of sensitivity, which lead to necrosis and ulceration. Data from the international literature estimate that 3-14% of hospitalized patients develop pressure ulcers. We herein describe the simultaneous correction of extensive sacral and ischial ulcers in a young paraplegic patient, using a gluteus maximus fasciomyocutaneous flap from the posterior aspect of the thigh.
Keywords: Myocutaneous; Pressure ulcer; Paraplegia; Muscle spasticity; Risk factors
RESUMO
Úlceras de pressão são alterações da integridade da pele e tecidos subjacentes, causadas por pressão, mais usualmente sobre proeminências ósseas, especialmente em áreas desprovidas de sensibilidade, levando à necrose e ulceração. Dados da literatura internacional estimam que 3 a 14% dos pacientes hospitalizados desenvolvem úlceras de pressão. Descrevemos a correção simultânea de úlceras sacral e isquiática extensas em paciente paraplégico jovem utilizando retalho fasciomiocutâneo de glúteo máximo e de face posterior da coxa.
Palavras-chave: Retalho miocutâneo; Lesão por pressão; Paraplegia; Espasticidade muscular; Fatores de risco
INTRODUCTION
Pressure ulcers are alterations of the integrity of the skin and underlying tissues, caused by pressure, most commonly on the protuberances, especially in areas deprived of local sensitivity, which lead to necrosis and ulceration.
Data from the international literature estimate that between 3% and 14% of all hospitalized patients develop pressure ulcers1, which emphasizes the importance of preventive measures in patients with increased risk. The surgical treatment of pressure ulcers dates back to 1947, with Croce and Beakes2 using skin flaps.
The use of muscle and musculocutaneous flaps (proposed by Ger3, Minami et al.4, and Nahai et al.5) and fasciocutaneous flaps (proposed by Hurwitz et al.6, Alonso et al.7, Ramirez8, Calil et al.9, and Paletta et al.10) was a significant improvement to the surgical arsenal for the treatment of these conditions. Within the widely varied situations that arise in daily clinical practice, surgical solutions with characteristics appropriate to the patient’s local needs are vital.
OBJECTIVE
This study aimed to describe the simultaneous correction of extensive sacral and ischial pressure ulcers with a single flap in a 21-year-old paraplegic patient. He was admitted with anemia, urinary infection, necrotic ulcers, and spastic contracture in the lower limbs. After clinical treatment, he was submitted to correction of the ulcers by rotation of a fasciomyocutaneous flap from the gluteus maximus and posterior surface of the thigh, pediculated by the superior and inferior gluteal artery and the posterior fasciocutaneous branch of the thigh.
In spite of the dimensions, the flap used displayed good blood perfusion, evolving without necrosis or dehiscence. The flap proved to be a valid option for young patients without diseases that lead to circulatory impairment.
CASE REPORT
A 21-year-old male patient with a 1-year history of paraplegia received inadequate care, which led to the development of multiple pressure ulcers, including extensive right sacral and ischial ulcers. The patient was admitted febrile, malnourished, anemic, and with urinary tract infection, necrotic ulcers, and spastic contracture in the lower limbs.
After clinical preparation, simultaneous correction of the right sacral and ischial ulcers through the rotation of a single fasciomyocutaneous flap was performed.
Surgical technique
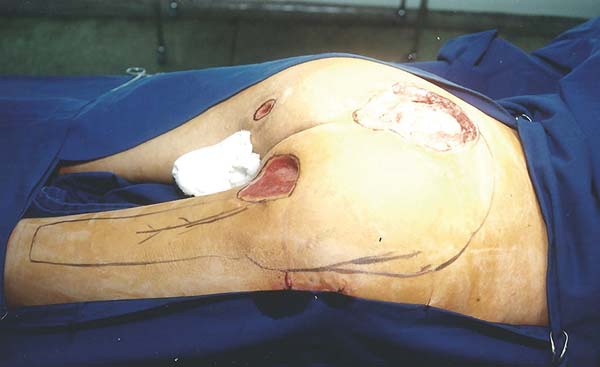
The patient was positioned in ventral decubitus, with the flap and edges of the ulcers demarcated (Figure 1), followed by dissection of the flap from the distal extremity while securing the fascia to the subcutaneous cell tissue (TCSC), elevation of the gluteus maximus and cutaneous portions (Figure 2), rotation and suturing of the flap closing the two ulcers (Figure 3), and closing the donor area of the thigh edge to edge. The flap and donor area evolved with good healing (Figures 4 and 5).









RESULTS
The flap used for the simultaneous correction of the right sacral and ischial ulcers showed good blood perfusion and evolved without necrosis or hematoma. The patient presented mild superficial pressure sores at the proximal extremity of the posterior thigh donor area by tension in the suture line, which healed spontaneously, and presented serous-sanguineous secretion drainage in its distal end, which did not prevent proper healing. We emphasize that the tension did not impair the venous return of the right lower limb.
DISCUSSION
According to Alonso et al.7 and Paleta et al.10, the circulation of the posterior fasciocutaneous portion of the thigh flap was programed to be nourished from the fasciocutaneous branch of the inferior gluteal artery. The anatomical studies of Calil et al.9 showed an intersection between the first and second perforating branches of the deep femoral artery, which leads to an extensive area of cutaneous perfusion in the posterior aspect of the thigh, which allows the preparation of large flaps.
The study of Hurwitz et al.6 showed inferior gluteal artery anastomoses with branches of the medial femoral circumflex artery. When these and other anastomotic vessels were sectioned, the inferior gluteal artery could supply the circulation of the posterior region of the thigh.
Ramirez8 mentioned the importance of the first perforating artery for the perfusion of the posterior fasciocutaneous thigh flap. In two-thirds of flaps in the study, the artery was ligated without impairment of the flap. The author also mentioned the importance of the branches of the medial femoral circumflex artery with its more superior and medial location than the first perforator.
Owing to the arc of rotation of the flap used in the present study and the inclusion of the gluteus maximus muscle, ligation of the first and second perforating arteries was needed to maintain the perfusion of the posterior fasciocutaneous portion of the thigh through the inferior fasciocutaneous gluteal artery branch. The inclusion of the gluteus maximus muscle in the flap enabled a better filling of the extensive sacral ulcers.
In the event of necrosis of the fasciocutaneous portion, one option would be to use the myocutaneous flap of the local gracilis or fasciocutaneous. In sacral ulcer relapse, a fasciocutaneous flap may be made for closure alone or associated with a musculocutaneous or fasciocutaneous flap of the contralateral gluteal region.
CONCLUSIONS
The use of fasciomyocutaneous flaps from the gluteus maximus and posterior surface of the thigh proved to be a good surgical option for simultaneous correction of right sacral and ischial ulcers as demonstrated in the case of a young patient described herein, who had no illnesses that would lead to circulatory impairment and clinical imbalance.
REFERENCES
1. Bergstrom N, Allman RM, Alvarez OM, Carlsson CE, Eaglesetein W, Frantz RA, et al. Pressure ulcer in adults: prediction and prevention. Rockville: Agency for Health Care Policy and Research; 1992.
2. Croce EJ, Beakes HC. The operative treatment of decubitus ulcer. N Engl J Med. 1947;237(5):141-9.
3. Ger R. The surgical management of decubitus ulcers by muscle transposition. Surgery. 1977;69(1);106-10.
4. Minami RT, Mills R, Pardoe R. Gluteus maximus myocutaneous flaps for repair of pressure sores. Plast Reconstr Surg. 1977;60(2):242-9.
5. Nahai F, Silverton JS, Hill HL, Vasconez LO. The tensor fascia lata musculocutaneous flap. Ann Plast Surg. 1978;1(4):372-9.
6. Hurwitz DJ, Swartz WM, Mathes SJ. The gluteal thigh flap: a reliable, sensate flap for the closure of buttock and perineal wounds. Plast Reconstr Surg. 1981;68(4):521-32.
7. Alonso N, Carramaschi F, Calonge HCF, Gemperli R, Monteiro Júnior AA, Ferreira MC. Retalho fasciocutâneo posterior da coxa no tratamento de úlceras de pressão. Rev Bras Ortop. 1986;21(1):13-5.
8. Ramirez OM. The distal gluteus maximus advancement musculocutaneous flap for coverage of trochanteric pressure sores. Ann Plast Surg. 1987;18(4):295-302.
9. Calil JA, Ferreira LM, Neto MS, Castilho HT, Garcia EB. Aplicação clínica do retalho fasciocutâneo da região posterior da coxa em V-Y. Rev Assoc Med Bras. 2001;47(4):311-9.
10. Paletta C, Bartell T, Shahadi S. Applications of the posterior thigh flap. Ann Plast Surg. 1993;30(1):41-7.
1. Universidade Estadual de Londrina, Londrina,
PR, Brazil.
2. Universidade Federal do Paraná, Curitiba, PR,
Brazil.
Corresponding author: Antonio Chiquetti Junior, Rua Paes Leme, nº 1264, sala 601 - Jardim das Américas - Londrina, PR, Brazil, Zip Code: 86010-610. E-mail: chiqueti@sercomtel.com
Article received: April 12, 2018.
Article accepted: October 1, 2018.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket