



Articles - Year 1999 - Volume 14 -
Resurfacing with Tru-Pulse Laser - The Ideal Procedure for Dark Skin Individuals
Resurfacing com Tru-Pulse Laser - Uma Conduta Ideal para Pessoas de Pele Morena
ABSTRACT
The advent of Ultrapulse CO2 laser provided plastic surgeons with the opportunity to present their patients with the most simple and efficient treatment for skin lesions, including those from periocular region, periorbital and peribuccal wrinkles and frontal scars. The authors of this work present their experiences in 11 cases of resurfacing using CO2 laser. Material and methods used for skin preparation, type of anesthesia as well as a demonstration of how to do resurfacing and which intensity should be used in some cases are described; also, their experience with the exposed dressing) the postoperative and results are reported. Some photos of patients before and after laser application showing a satisfactory result for the physicians and a more pleasant life for the patients are shown on the conclusion.
Keywords: Resurfacing with C02 laser; laser in dark skins; facelift/full face; CO2 Tru-Pulse laser.
RESUMO
O advento do Laser Ultrapulsátil de CO2 deu aos cirurgiões plásticos a oportunidade de presentear seus pacientes com o mais simples e eficaz tratamento para lesões da pele, incluindo as da região periocular, as rugas periorbitais, peribucais e cicatrizes frontais. Os autores deste trabalho apresentam suas experiências em 111 casos de resurfacing com laser de CO2. São descritos os materiais e os métodos por eles utilizados para a preparação da pele, o tipo de anestesia, demonstrando-se como fazer o resurfacing e qual a intensidade que deverá ser utilizada em alguns casos; são relatados também suas experiências com o curativo expositivo, o pós-operatório e os resultados. Na conclusão, são exibidas algumas fotografias de pacientes antes e depois da aplicação do laser, demonstrando um resultado satisfatório para os doutores e uma vida mais agradável para os pacientes.
Palavras-chave: Resurfacing com laser de CO2; laser em peles morenas; facelift/full face; Tru-Pulse Laser de CO2.
Our rationale reports treatment of 111 patients, 6 males and 105 females, with ages ranging from 47 to 66 years old. Predominant color was the dark one, Fitzpatrick III to V (Fig. 1); treatment of periaral region prevailed (Fig. 2), since patient's greater complaint rate referred to this area.
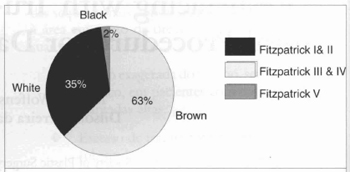
Fig. 1 - 65% of the patients is Fitzpatrick In to V.

Fig. 2 - Major demand is patients with wrinkles at oral region.
SKIN TREATMENT
All patients were submitted to previous skin preparation for 15 to 45 days (Table I) and also to supplemental treatment starting at the 30th postoperative day for 30 days (Table II). Laser was associated to other techniques when patients presented flaccidity, deep wrinkles and/or depressions (Fig. 3).
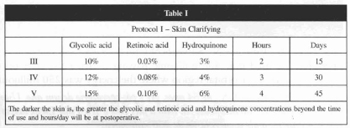
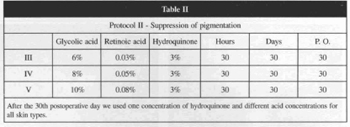

Fig. 3 - The use of laser has been associated to techniques such as implants, cantoplasties, cervical lifting, face lifting and others.
Patients that presented great potential for allergy, spots caused by insect sting, use of isotetrinoine, emotional instability or those who have not followed postoperative care were withdrawn. Special attention was given to those patients with herpes history, all of them being prophilatically medicated
ANESTHESIA
Local anesthesia was the method of choice for all patients and the drug for infiltration was 0.5% lidocaine with epinephrine at 1:200,000 associated to regional blockade.
Sedation was carried out by anesthesiologists from our team with the use of phentanyl, demerol and midazolem endovenous solutions in patients submitted to full-resurfacing and in those for whom the process was associated to face-lifting. The experience in maintaining a stable narcosis threshold turned the use of oxygen therapy unnecessary, so interruption of laser application was not required.
RESURFACING
Face regions, as well as deep wrinkles were marked and those regions with variable intensity and frequency according to cutaneous thickness were scanned in order to facilitate the procedure. The changes in the amount of scanner passing varied according to cutaneous thickness. The application of 300 millijoules in two passing at lower eyelid region was generally sufficient. 300 millijoules were applied in two passing at malar region; 400 to 500 millijoules twice or three times at labial region and 500 millijoules with a total of two or three passing and four to six passing at the top of the deeper wrinkles. Two to four passing were made at frontal region with 500-millijoule intensity, the same occurring in upper maxillary regions and mentum.
Note: For all patients submitted to full-resurfacing) we carried out a degradê of about 2 centimeters at the cervical region boundaries (scanning with skin spacing).
DRESSING
After washing the face with physiological saline, the operated areas were covered with healing cream with antibiotic - 0.5% Clostebol Acetate + 0.5% Neomycin sulfate - the so-called Semi-Open Dressing (Fig. 4), and the patient was removed to room with the prescription of anti-inflammatory analgesics, oral antibiotic and rest, and the instruction to continue treatment with an antiviral. All the patients were discharged from hospital after a one or two hour rest when submitted to laser therapy only.

Fig. 4 - At immediate postoperative we used exposed dressing with healing cream.
The patients were instructed to keep the face always covered with the cream - 0.5% Clostebol Acetate + 0.5% Neomycin Sulfate -, and the face should be washed upon our supervision at the 3rd P.O. (Fig. 4), when the use of an hydrating lotion with sun filter and 5% Dexpantenol was initiated. Patient return to his or her activities in general occurred at the 10th P.O., and the patient was asked to return weekly to consultation. Second protocol, with which pigmentation is avoided, was determined to start at the 30th P.O.
DISCUSSION AND CONCLUSION
We would like to make a critical evaluation of this work initially speaking about the fear we felt till we managed to precisely handle the intensity and the number of laser passing required for each area. The option for Exposed Semi-Open dressing with a thick layer of cream has been satisfactory. The formation of small crusts that were eliminated in about four days with facial bathes, petrolatum and the use of acetic acid were not a problem for us. The special attention given to lower eyelid treatment avoided sclera-show or ectropion and we concluded that the test performed to verify tarsal tension and prophylactic contoplasty would be the best procedure when required. We also observed that skin retraction after laser passing at labial region made it more graceful and, in some cases, the association to implants was the ideal upgrade to get a more harmonized mouth contour.
An outstanding joviality was obtained at frontal region where a supplemental treatment of muscle hypertrophy with botuline toxin and synthetic implant for the deeper wrinkles were carried out.
Small exeresis and deeper lesion sutures were previously performed when required, in order to treat acne sequelae with laser, which greatly facilitated the skin leveling for laser use.
Finally, we would like to state that the least tissue traumatism, the more precise removal of skin layers, the absence of ecchymosis, less postoperative pain and patient recovery speed were the factors that have stimulated us to proceed with the Ultrapulse CO2 laser treatment.
RESULTS
The evaluation of treatment efficacy taking into consideration the great patient satisfaction, the safety to treat hyperpigmentation, the persistence of erythema for minimal time (always less than 45 days) and the absence of hypopigmentation in all cases led us to excellent results in 57% of the areas treated in a 12-to-18 month follow-up (Fig. 5).
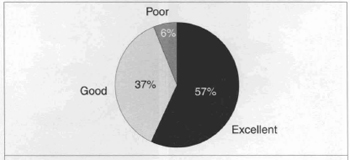
Fig. 5 - Erythema disappears after 45 postoperative days. 94% of satisfactory results were obtained in a 18 month follow-up.

Figs. 6a & 6b - Patient S.N., 54 years old, preoperative and one-year postoperative. We used four 500 millijoule passing of Tru-Pulse laser on the whole face except for orbital region where the energy was 250 millijoules.

Figs. 7a & 7b - Patient M.I.A, 49 years old, preoperative and six-month postoperarive, the laser being associated to cervical lifting.

Figs. 7c & 7d - Patient M.I.A, 49 years old, preoperative and six-month postoperative, laser has been associated to cervical lifting.

Figs. 8a & 8b - Patient I.C., 50 years old, face, Fitzpatrick IV with sun keratosis. Preoperative and 60-day postoperative.
REFERENCES
1. ALSTER T, PRESTON L, MACEDO OR. Beneficios da Cirurgia Cosmética a Laser. Senac : São Paulo, 1997.
2. CALDEIRA A, GRIGALEK G. Chemical Face Dermabrasion Six Years Experience. Rev. Soc. Bras. Cir. Plast. Estet. Reconstr. 1995; 10(3): 3-74.
3. FANOUS N, PRINJA N, SAWAF M. Laser resurfacing of the neck: a review of 48 cases. Aesth. Plast. Surg. 1998; 22:173-179.
4. ROBERT III TL, BADIN AZD, MORAES LM. Rejuvenescimento Facial a Laser. Rio de Janeiro : Revinter, 1998.
5. ROBERTS III TL. The emerging role of laser resurfacing in combination with traditional aesthetic facial plastic surgery: 1998; 22:75-80.
6. RONCATTI C, TUNDISI M. Resurfacing com o Ultrapulse-Laser; Nova arma no rejuvenescimento facial. Rev. Soc. Bras. Cir. Plast. Estet. Reconstr. 1996; 11(2):3-74.
7. MAHE E. Lower lid blepharoplasty - the transconjuctival approach: extended indications.
Aesth. Plast. Surg. 1998; 22:1-8.
8. MELE JA, KULICK MI, LEE D. Aesthetic laser blepharoplasty: Is it safe? Aesth. Plast. Surg. 1998; 22:9-11.
9. WOOD-SMITH, REES TD. Cosmetic Facial Surgery. Philadelphia : W.B. Saunders, 1973.
I - Senior Member of the Brazilan Society of Plastic Surgery
Address for correspondence:
Moises Wolfenson, MD
Av.João de Barros, 791
54470-090 - Recife - PE Brazil
Phone: (55-81) 231-1621 Fax: (55-81) 421-1190
From the Plastic Surgery and Laser Department of Hospital Mont Sinai.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket