



Original Article - Year 2018 - Volume 33 -
New classification of hypertrophy of the labia minora and correlation with indicated surgical techniques
Nova classificação para hipertrofia dos pequenos lábios vaginais e correlação com as técnicas cirúrgicas indicadas
ABSTRACT
INTRODUCTION: Nymphoplasty or labioplasty is the most common genital plastic surgery. The objective of labioplasty is to correct hypertrophy of the labia minora and clitoral prepuce, removing excess tissue without affecting their function of protecting the vagina and aiding in genital lubrication. Several types of classifications have been proposed to facilitate the understanding of the degree of hypertrophy of the labia minora and assist in selecting the most suitable procedure in labioplasty. After analyzing several classifications, the author proposes a new classification to facilitate the understanding of hypertrophy of the labia minora, clitoral hood, and vaginal prepuce and help select the best labioplasty procedure.
METHODS: A literature search was conducted in PubMed/Medline using the following terms: hipertrofia lábios vaginais, labioplastia, labiaplasty, labioplasty, labia minora hypertrophy, and labial protrusion. All the classifications described in the identified studies were analyzed.
RESULTS: A new classification has been proposed. Hypertrophy of the labia minora was classified in four grades: grade 0 (< 1 cm), grade 1 (> 1 cm and < 3 cm), grade 2 (> 3 cm and < 5 cm), and grade 3 (> 5 cm).
CONCLUSIONS: The new classification improves the understanding of the size and extent of hypertrophy of the labia minora and helps select the best procedure in labioplasty.
Keywords: Hypertrophy; Vulva; Reconstructive surgical procedures; Female genitalia; Minor surgical procedures.
RESUMO
INTRODUÇÃO: Primeira colocada entre as mais procuradas cirurgias plásticas genitais, a ninfoplastia ou labioplastia visa a correção da hipertrofia dos pequenos lábios vaginais e prepúcio, retirando seu excesso, sem interferir na sua função de proteção da vagina e auxílio na lubrificação genital. Diversos tipos de classificações foram propostos para facilitar a compreensão do grau de hipertrofia dos pequenos lábios vaginais e ajudar na escolha da técnica da labioplastia. Após analisar várias classificações, o autor propõe uma nova classificação, no intuito de facilitar a compreensão da hipertrofia das ninfas, capuz do clitóris e prepúcio e ajudar na escolha da técnica apropriada para labioplastia.
MÉTODOS: Foi feita uma busca na literatura médica PubMed/Medline com os termos hipertrofia lábios vaginais, labioplastia, labiaplasty, labioplasty, lábia minora hipertrophy, labial protrusion. Foram analisadas todas as classificações descritas nos trabalhos encontrados.
RESULTADOS: Uma nova classificação foi proposta. A hipertrofia dos pequenos lábios vaginais foi classificada em 4 graus: Grau 0 (< 1 cm), Grau 1 (> 1 cm e < 3 cm), Grau 2 (> 3 cm e < 5 cm) e Grau 3 (> 5 cm).
CONCLUSÕES: A nova classificação, além de facilitar a compreensão do tamanho e extensão da hipertrofia das ninfas, também auxilia na escolha da técnica a ser escolhida para a labioplastia.
Palavras-chave: Hipertrofia; Vulva; Procedimentos cirúrgicos reconstrutivos; Genitália feminina; Procedimentos cirúrgicos menores.
The increased access of the population to nudity on television, internet, printed media, and other media improves the understanding of the anatomy of the female genitalia by women, allowing the comparison of genital structures by this population1-4 and the formation of an aesthetic pattern, with a consequent increase in the interest in genital aesthetic surgery.
The labia minora of the vagina are formed by two skin folds that extend from the frenulum of the clitoris to the posterior commissure of the vaginal vestibule. The labia minora are filled with connective tissues with erectile properties and have a rich vascular and nervous network. The lateral area is composed of keratinized epithelium and fuses to the labia majora in the interlabial sulcus. The medial area joins the lateral portion of the vaginal vestibule5,6.
The labia minora that protrude through the labia majora and become exposed provide a loose and wrinkled appearance to the vulva and may cause embarrassment to some women.
Nymphoplasty or labioplasty is the most common genital surgery. The objective of labioplasty is to correct hypertrophy of the labia minora and clitoral prepuce, removing excess tissue, without interfering with their function of protecting the vagina and aiding in genital lubrication.
Several types of classifications have been proposed to facilitate the understanding of the degree of hypertrophy of the labia minora and assist in selecting the best procedure in labioplasty. After analyzing several classifications, the author proposes a new classification to facilitate the understanding of hypertrophy of the labia minora, clitoral hood, and clitoral prepuce and help select the most appropriate labioplasty procedure.
OBJECTIVE
To present a new classification for hypertrophy of the labia minora to facilitate the understanding of the degree and extent of hypertrophy and help select the best labioplasty procedure.
METHODS
A literature search was conducted in PubMed/Medline using the following terms: hipertrofia lábios vaginais, labioplastia, labiaplasty, labioplasty, labia minora hypertrophy, and labial protrusion. Four classifications were found for hypertrophy of the labia minora: Felicio8, Cunha9, Motakef3, and Gonzalez10.
After analyzing several classifications and considering the experience of the author in performing 400 labioplasty surgeries, a new classification of hypertrophy of the labia minora was proposed. The study was developed in the author's private clinic in São Paulo, Brazil from March to June 2017 and was approved by the Research Ethics Committee of the clinic. The study also complied with the principles of the Declaration of Helsinki.
RESULTS
The literature review allowed the identification of four classifications of hypertrophy of the labia minora:
Classification of Felicio, 19928
Yhelda Felicio (1992) published the first classification of hypertrophy of the labia minora in the French magazine La Revue de Chirurgie Esthétique de Langue Française8. In some publications, this classification is erroneously attributed to that of Franco3,11-15. This scoring takes into account the distance from the base of the labia minora near the vaginal introitus to the most distal margin.
Grade 1: < 2 cm;
Grade 2: 2-4 cm; Grade 3: 4-6 cm; Grade 4: > 6 cm.
Although simple, this first classification takes into account the entire extension of the labia minora from their base near the vaginal introitus. However, it does not evaluate the protruding and exposed tissue, which is usually the cause of most complaints by patients. Therefore, comparing and estimating the actual hypertrophy in different cases are difficult because the size of the labia majora interferes with the concealment or exposure of the labia minora.
Labia minora with a width of 2 cm remain concealed by the labia majora in cases in which the latter have a projection of 2 cm. The same 2 cm labia minora may be exposed in cases in which the labia majora are atrophic, without volume. This classification does not take into account the presence of hypertrophy of the clitoral hood or prepuce, which often accompanies hypertrophy of the labia minora.
Classification of Cunha, 20119
Grade 1: Excess skin in the posterior/inferior region adjacent to the vaginal introitus;
Grade 2: Excess skin that extends laterosuperiorly to the clitoris;
Grade 3: Excess skin in the entire region, including the clitoral prepuce (Figures 1 to 3).
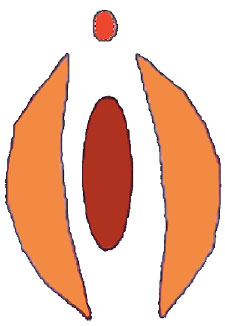
Figure 1. Classification of Cunha type 1.

Figure 2. Classification of Cunha type 2.
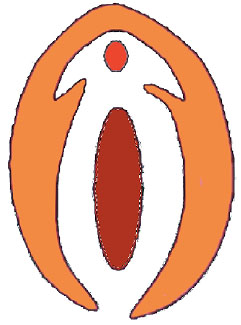
Figure 3. Classification of Cunha type 3.
This classification is the first to contemplate the extension of hypertrophy from the vaginal prepuce to the labia minora but does not infer the size of the labia minora nor the protruding tissue. However, this inference is necessary for selecting the surgical procedure and is the cause of most complaints by patients.
Classification of Motakef, 20153
This classification takes into account the protruding tissue of the labia minora, i.e., the distance from the labia majora to the most distant margin of the labia minora.
Grade 1: < 2 cm;
Grade 2: 2-4 cm;
Grade 3: > 4 cm (Figure 4).
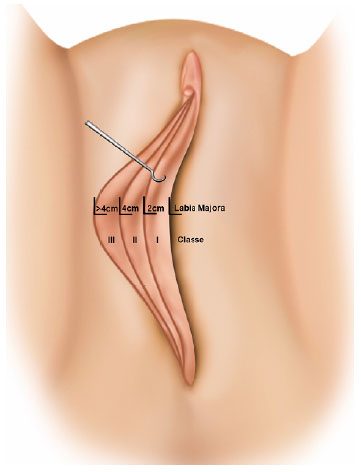
Figure 4. Classification of Motakef3.
Letter "A" is added to the numerical classification in cases of asymmetry, and letter "C" is added in cases of increase in the size of the clitoral hood and prepuce.
This classification is logical for measuring hypertrophy because the measurement is made not from the base of the labia minora near the introitus, but from the protruding tissue, which is considered hypertrophic. However, the entire labia minora protrude in cases of atrophy and lack of volume of the labia majora, thus providing an overestimated assessment of hypertrophy.
Classification of Gonzalez, 201510
Gonzalez proposed a more comprehensive classification to clarify the structure of the labia minora, vaginal prepuce, and clitoral hood, as well as the presence or absence of asymmetry in the labia minora.
Similar to Motakef's classification, the size of the labia minora is measured from the protruding exposed tissue that is not covered by the labia majora.
| Grade of hypertrophy | Location | Symmetry |
| Grade 1: <2 cm | A: Anterior | Symmetrical |
| Grade 2: 2 to 4 cm | B: Central | Asymmetrical |
| Grade 3: 4 to 6 cm | C: Generalized | |
| Grade 4: > 6 cm |
(Figures 5 to 7).
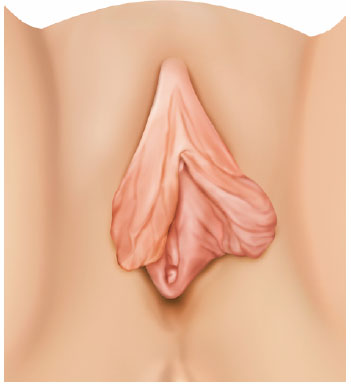
Figure 5. Classification of Gonzalez10, class A.
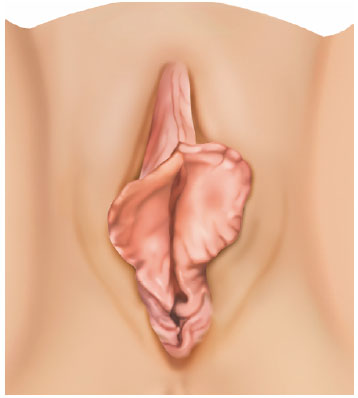
Figure 6. Classification of Gonzalez10, class B.
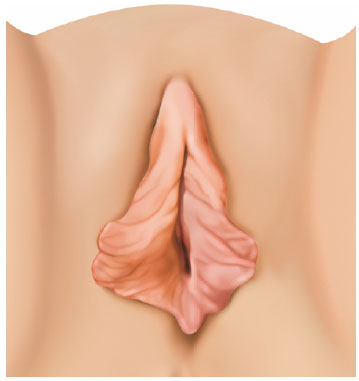
Figure 7. Classification of Gonzalez10, class C.
With regard to hypertrophic extension, letter "A" classifies the hypertrophy that predominantly affects the anterior area of the labia minora closer to the clitoris. Letter "B" classifies central hypertrophy, which is predominantly distal to the clitoris. Letter "C" classifies hypertrophy along the entire extension from the vaginal prepuce to the area next to the introitus.
Letter "S" indicates symmetry, whereas letter "A" indicates asymmetry.
Although more complete and complex, this classification presents the same difficulty in standardizing the cases in which the labia majora are atrophic, without volume. The absence of actual hypertrophy in cases of flat labia majora with 1-cm labia minora may have the same classification as a 3-cm labia minora, in which the volume of the labia majora covers 2 cm of the labia minora. In both cases, the exposed tissue size is 1 cm; however, surgery is not indicated in the former.
New classification
We propose a new classification to provide a comprehensive information on hypertrophy, including the size and extension of the hypertrophic tissue resectable by labioplasty, facilitating the choice of the surgical technique.
Considering that the minimum size of the labia minora should be at least 1 cm1,3,7,16,17 and that resection should not leave tissues smaller than 1 cm even in cases in which the height of the labia majora is shorter or absent, the following classification is used:
| Grade of hypertrophy | Extension of hype |
| Grade 0: < 1cm | A: affects the labia minora below the clitoris |
| Grade 1: >1 cm and < 3 cm | B: affects the labia minora above the clitoris, extending to the prepuce |
| Grade 2: >3 cm and < 5 cm | |
| Grade 3: > 5 cm |
(Figure 8).
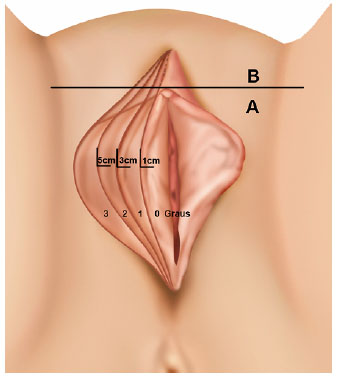
Figure 8. Classification of Colaneri.
The following classification of the labia minora is used:
Grade 0: < 1 cm
When there is an absence of hypertrophy and when the labia minora are small (up to 1 cm from their base near the vaginal introitus to their most distant margin), they should not be operated1,3,7,16. In cases in which there are protrusion and exposure of the labia minora, atrophy and lack of volume of the labia majora should be considered, and the procedure should include the use of a fat graft or another type of filling and not labioplasty.
Grade 1: > 1 cm and < 3cm
This slight degree of hypertrophy allows the resection of 2 cm of the labia minora; however, the first centimeter should be maintained intact. In these cases, wedge resection techniques are not recommended by most authors3,18. Direct resection and de-epithelialization are indicated7.
Grade 2: > 3 cm and < 5 cm
In this degree of hypertrophy, wedge resection techniques are indicated because the resectable part is 2 to 4 cm and protects the pedicle, with a good vascular and nervous network. Direct resection is also recommended; however, de-epithelialization should not be performed to avoid a thickened appearance of the labia minora19.
Grade 3: > 5 cm
There is a significant hypertrophy probably with thickened labia minora and broad base.
In these cases, wedge resection and flap rotation are indicated. Direct resection and de-epithelialization provide a thickened appearance to the labia minora. Resection should be performed by laser because it allows the removal of the internal tissues of the labia minora, making the structure thinner and avoiding thickening of their base.
Extent of hypertrophy.
A: Hypertrophy affects only the labia minora.
B: Hypertrophy affects the labia minora and the region above the clitoral hood and can extend to the prepuce.
In cases classified as B, resection should be extended to the vaginal hood and/or prepuce for a better aesthetic result.
With regard to the asymmetry of the labia minora: Some degree of asymmetry is common20. Although asymmetry is common in double organs, including ears, hands, and eyebrows, the labia minora appear to be more prone to asymmetry, and the asymmetries are significant in many cases. Therefore, tissue asymmetry was not classified, and in cases of large asymmetries, classifying different areas of the labia minora (e.g., right and left) is recommended, such as grade 3B right and grade 1A left.
The different degrees of hypertrophy were determined by selecting cases of direct resection because the marking and the surgical specimen facilitate the visualization of the excess tissue (Figures 9 to 19).
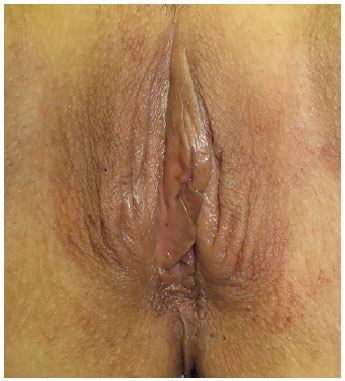
Figure 9. Grade 0.
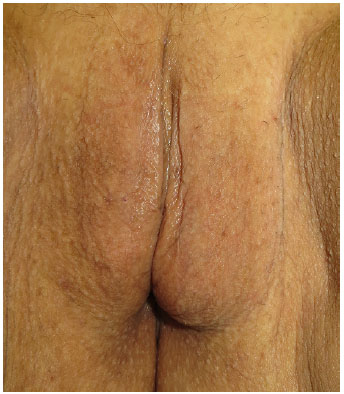
Figure 10. Grade 0; surgical results 1 year and 4 months after fat grafting of the labia majora.
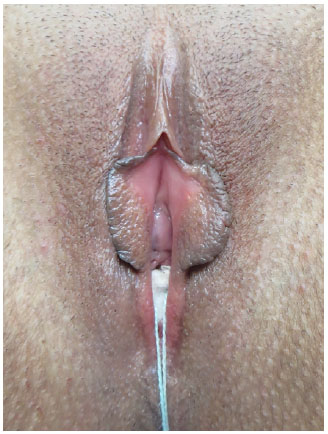
Figure 11. Grade 1A.
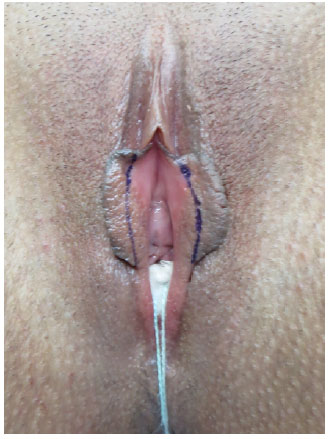
Figure 12. Grade 1A, demarcation of the excess tissue.

Figure 13. Grade 2A.
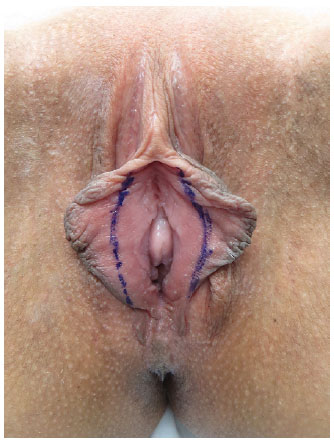
Figure 14. Grade 2A, demarcation of the excess tissue.
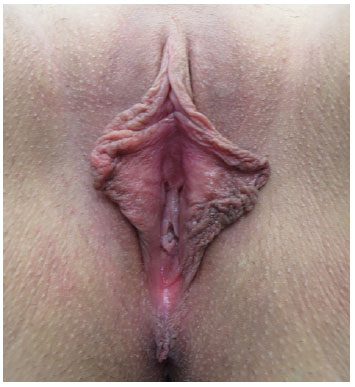
Figure 15. Grade 2B.
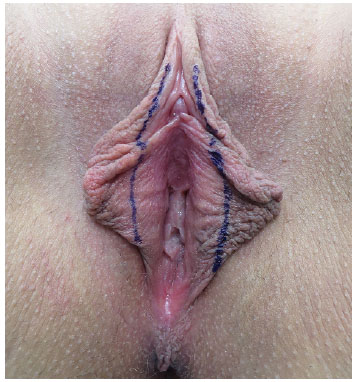
Figure 16. Grade 2B, demarcation of the excess tissue.
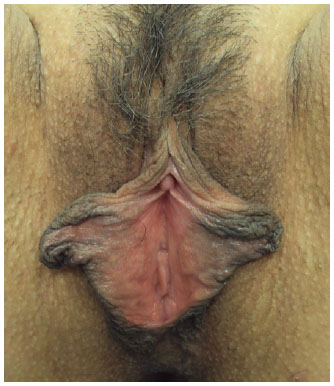
Figure 17. Grade 3A.

Figure 18. Grade 3A, demarcation of the excess tissue.

Figure 19. Grade 3B right and 1A left.
DISCUSSION
Although several classifications of hypertrophy of the labia minora have been proposed, there is no consensus on the use of these classifications. We sought a classification that could help understand the size and extent of hypertrophy and select the most appropriate surgical procedure in each case. In our case series of up to 400 cases of labioplasty, we lack a simple and complete classification, which facilitates the understanding of the size and extent of hypertrophy, as well as simplify the comparison between different cases.
This new classification indicates the resectable size of the labia minora and the extension of hypertrophy, providing a broader analysis of each case and therefore allowing the selection of the most appropriate surgical procedure.
According to the current literature, some grades based on this classification can be inferred:
Grade 0: Labioplasty should not be performed; the minimum size of the labia minora to be maintained is 1 cm1,3,7,16,17; thus, surgery is contraindicated. In cases of exposure of the labia minora due to atrophy and lack of volume of the labia majora, fat grafting or other filling techniques are indicated to increase the volume of the labia majora.
Grade 1: Small hypertrophy and well resolved by direct resection or de-epithelization3,19. Wedge resection and flap rotation are not recommended for labia minora smaller than 3 cm5,7 because the pedicle becomes very thin, increasing the risk of necrosis and dehiscence.
Grade 2: Hypertrophy with a possibility of resection of 2 to 4 cm. Wedge resection techniques are indicated because the pedicle is safe. Direct resection is adaptable to any case and is recommended. De-epidermization is not suggested because it thickens the base of the labia minora3.
Grade 3: Significant hypertrophy. De-epidermization is not indicated because the labia minora are long and thick. Direct resection should be performed by laser because it allows the resection of an internal wedge, removing the internal tissue and thinning the labia minora, thus preventing the thickening of the base of the labia minora. Wedge resection and flap rotation are indicated and safe for the pedicle.
Category A or B indicates the extent of hypertrophy and the need to extend the resection beyond the labia minora by covering the tissue around the clitoris and prepuce.
Asymmetry was not classified because some degree of asymmetry occurs in most cases. In cases of significant asymmetry, each side of the labia minora should be classified separately, indicating the side after classification, e.g., grade 3B right and grade 1A left.
CONCLUSION
The proposed new classification improves the understanding of the size and extent of hypertrophy of the labia minora and prepuce and allows the selection of the most suitable procedure in labioplasty.
COLLABORATIONS
AGFC Analysis and/or interpretation of data; conception and design of the study; completion of surgeries and/or experiments; writing the manuscript or critical review of its contents.
REFERENCES
1. Hodgkinson DJ, Hait G. Aesthetic vaginal labioplasty. Plast Reconstr Surg. 1984;74(3):414-6. PMID: 6473559 DOI: http://dx.doi.org/10.1097/00006534-198409000-00015
2. Munhoz AM, Filassi JR, Ricci MD, Aldrighi C, Correia LD, Aldrighi JM, et al. Aesthetic labia minora reduction with inferior wedge resection and superior pedicle flap reconstruction. Plast Reconstr Surg. 2006;118(5):1237-47. DOI: http://dx.doi.org/10.1097/01.prs.0000237003.24294.04
3. Motakef S, Rodriguez-Feliz J, Chung MT, Ingargiola MJ, Wong VW, Patel A. Vaginal Labiaplasty: Vaginal labiaplasty: current practices and a simplified classification system for labial protrusion. Plast Reconstr Surg. 2015;135(3):774-88. DOI: http://dx.doi.org/10.1097/PRS.0000000000001000
4. Alter GJ. A new technique for aesthetic labia minora reduction. Ann Plast Surg. 1998;40(3):287-90. DOI: http://dx.doi.org/10.1097/00000637-199803000-00016
5. Goodman MP. Female genital cosmetic and plastic surgery: a review. J Sex Med. 2011;8(6):1813-25. DOI: http://dx.doi.org/10.1111/j.1743-6109.2011.02254.x
6. Trichot C, Thubert T, Faivre E, Fernandez H, Deffieux X. Surgical reduction of hypertrophy of the labia minora. Int J Gynaecol Obstet. 2011;115(1):40-3. PMID: 21803353 DOI: http://dx.doi.org/10.1016/j.ijgo.2011.04.007
7. Choi HY, Kim KT. A new method for aesthetic reduction of labia minora (the deepithelialized reduction of labioplasty). Plast Reconstr Surg. 2000;105(1):419-22. DOI: http://dx.doi.org/10.1097/00006534-200001000-00069
8. Felicio Y. Chirurgie Intime. Rev Chir Esth Lang Franc. 1992;27(67):37-43.
9. Cunha FI, Silva LM, Costa LA, Vasconcelos FRP, Amaral GT. Ninfoplasatia: Classificação e refinamentos técnicos. Rev Bras Cir Plást. 2011;26(3):507-11.
10. González PI. Classification of Hypertrophy of Labia Minora: Consideration of a Multiple Component Approach. Surg Technol Int. 2015;27:191-4.
11. Triana L, Robledo AM. Refreshing labioplasty techniques for plastic surgeons. Aesthetic Plast Surg. 2012;36(5):1078-86. DOI: http://dx.doi.org/10.1007/s00266-012-9916-z
12. Felicio Yde A. Labial surgery. Aesthet Surg J. 2007;27(3):322-8. DOI: http://dx.doi.org/10.1016/j.asj.2007.03.003
13. Hamori CA. Discussion: Vaginal labiaplasty: current practices and a simplified classification system for labial protrusion. Plast Reconstr Surg. 2015;135(3):789-90. DOI: http://dx.doi.org/10.1097/PRS.0000000000001215
14. Franco T, Franco D. Hipertrofia de Ninfas. J Bras Ginecol. 1993;103(5):163-8.
15. Cao Y, Li Q, Li F, Li S, Zhou C, Zhou Y, et al. Aesthetic Labia Minora Reduction with Combined Wedge-edge Resection: A Modified Approach of Labiaplasty. Aesthetic Plast Surg. 2015;39(1):36-42. DOI: http://dx.doi.org/10.1007/s00266-014-0428-x
16. Chang P, Salisbury MA, Narsete T, Buckspan R, Derrick D, Ersek RA. Vaginal labiaplasty: defense of the simple "clip and snip" and a new classification system. Aesthetic Plast Surg. 2013;37(5):887-91. DOI: http://dx.doi.org/10.1007/s00266-013-0150-0
17. Hexsel D, Pop S, Rusciani A. Rejuvenation of the External Female Genitalia. In: Robinson JK, Hanke CW, Siegel DM, Fratila A, Bhatia AC, Rohrer TE, eds. Aesthetic Surgical Procedures. London: Saunders; 2015. p. 666-72.
18. Rouzier R, Louis-Sylvestre C, Paniel BJ, Haddad B. Hypertrophy of labia minora: experience with 163 reductions. Am J Obstet Gynecol. 2000;182(1 Pt 1):35-40. PMID: 10649154 DOI: http://dx.doi.org/10.1016/S0002-9378(00)70488-1
19. Ellsworth WA, Rizvi M, Lypka M, Gaon M, Smith B, Cohen B, et al. Techniques for labia minora reduction: an algorithmic approach. Aesthetic Plast Surg. 2010;34(1):105-10. DOI: http://dx.doi.org/10.1007/s00266-009-9454-5
20. Daher M, Muñiz AR, Daher AC, Vanzan K, Monteiro G, Maciel J, et al. Ninfoplastia em estrela: técnica para redução dos pequenos lábios vulvares. Rev Bras Cir Plást. 2015;30(1):44-50.
Sociedade Brasileira de Cirurgia Plástica, São Paulo, SP, Brazil
Institution: Clínica privada, São Paulo, SP, Brazil.
Corresponding author:
Andre Gonçalves de Freitas Colaneri
Rua Borges Lagoa, 1065, conj. 100 - Vila Clementino
São Paulo, SP, Brazil - Zip Code 04038-032
E-mail: andrecolaneri@me.com
Article received: June 28, 2017.
Article accepted: January 26, 2018.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket