



Ideas and Innovation - Year 2017 - Volume 32 -
Periareolar zigzag incision as treatment for gynecomastia
Incisão periareolar em zigue-zague para tratamento de ginecomastias
ABSTRACT
INTRODUCTION: Gynecomastia is a benign hypertrophy and hyperplasia of the male mammary gland, and is considered the most frequent benign condition of the male breast. The objective is to evaluate aesthetic results and satisfaction of patients undergoing a new approach using a periareolar zigzag incision for the treatment of gynecomastia.
METHODS: We present 13 cases of male gynecomastia treated with a periareolar zigzag incision technique.
RESULTS: All patients were satisfied with the scar hidden in the transitional, naturally irregular periareolar skin of the nipple-areolar complex. No complications were observed in this patient series.
CONCLUSION: This approach is an excellent, easy-to-perform surgical alternative for the treatment of gynecomastia, providing a satisfactory cosmetic result without the presence of a stigmatizing scar.
Keywords: Gynecomastia; Hypertrophy; Hyperplasia; Cicatrix.
RESUMO
INTRODUÇÃO: Ginecomastia é a hipertrofia e hiperplasia benigna da mama masculina. Representa a condição benigna mais frequente da mama masculina. O objetivo é avaliar os resultados estéticos, e satisfação dos pacientes submetidos a uma nova abordagem para o tratamento da ginecomastia, com incisão periareolar em zigue-zague.
MÉTODOS: Apresentamos uma casuística de 13 casos de ginecomastia tratados com a técnica periareolar em zigue-zague.
RESULTADOS: Todos os pacientes ficaram satisfeitos com a cicatriz camuflada na transição, naturalmente irregular, da pele periareolar com o complexo aréolo mamilar. Não houve complicações na série descrita.
CONCLUSÃO: A abordagem descrita é uma excelente alternativa para o tratamento das ginecomatias. Proporciona um resultado estético satisfatório, é de fácil execução e tem a vantagem de não deixar estigmas na mama masculina operada.
Palavras-chave: Ginecomastia; Hipertrofia; Hiperplasia; Cicatriz.
Gynecomastia is considered to be a benign hyperplasia and hypertrophy of the male breast1. Galeno was the first to use the term gynecomastia, which was translated from Greek meaning "woman-like breast" (gyneco = woman, mastia = breast). It is the most common benign condition of the male breast2.
In most cases, gynecomastia is a bilateral condition; however, it can be unilateral in 20% of cases3. Generally, the breast shape is rounded, with variable volume, typically subareolar, and it can sometimes be painful, often concentric4. Except for neonatal, pubertal, and senile gynecomastia, considered physiologically normal, increased male breast volume is considered pathological5.
Gynecomastia is caused by alterations in the relationship between hormonal estrogen and androgen, whether physiological, idiopathic (most cases), or secondary to endocrine abnormalities or drug intake, including steroids. The incidence among adolescents aged 14 to 15 years is as high as 65%. In adults, the prevalence is as high as 32%, and following andropause, as high as 40 to 60%6,7.
Treatment is indicated when gynecomastia causes pain and/or emotional distress, particularly embarrassment and shame8. Treatment options are medical and surgical, with the latter indicated when gynecomastia is idiopathic and does not regress for 2 years9.
Glandular tissue resection by the direct, periareolar, or transareolar approach, with or without liposuction, is one of the most common surgical alternatives2. The goal of surgical treatment is abnormal breast tissue resection and normal male breast contour restoration, with minimal scarring, without residual deformity, and without vascular compromise (i.e., necrosis) of the papillary-areolar complex (CAP)9.
In 1973, Simon et al. published a classification scale that is used most commonly owing to its clinical surgical specificity and utility (Chart 1)10.
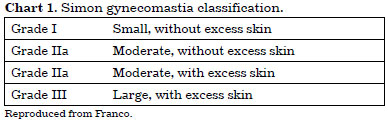
This paper presents an alternative approach for the treatment of Simon grades I and IIA gynecomastia, primarily through an irregular zigzag incision immediately below the periareolar region.
OBJECTIVE
This study aimed to describe the technique, analyze the surgical results, and measure the satisfaction of patients who underwent a new approach with periareolar zigzag incision for the treatment of gynecomastia.
MATERIAL AND METHODS
From January 2008 to February 2013, 13 patients with idiopathic gynecomastia, Simon grades I and IIb, with more than 2 years of evolution underwent surgery in the Plastic Surgery Department of the Hospital de Clínicas of the Federal University of Parana. The patients underwent endocrinological evaluation in the same hospital. All patients underwent surgical correction by using the technique presented in this study. For patients who did not undergo endocrinological evaluation, those with non-idiopathic cause and Simon's grade IIb and III gynecomastia were excluded.
A modified technique of periareolar zigzag incision was used, as described in the surgical technique.
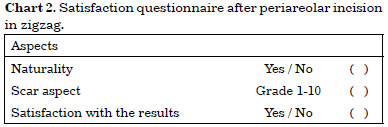
At the 6 month follow-up, the patients were evaluated, and a satisfaction questionnaire was administered with the following items: naturality, appearance of the scar (score, 1-10), and satisfaction with the results (Chart 2).
The study was reviewed and approved by the ethics committee of GRAF PLASTIC SURGERY - EPP INSTITUTION.
Surgical technique
Preoperative markings are made with the patient in a standing position. The semicircular, geometrically zigzagged periareolar incision is marked below the areola, taking care not to extend the markings to the skin surrounding the nipple-areolar complex (Figures 1 and 2).
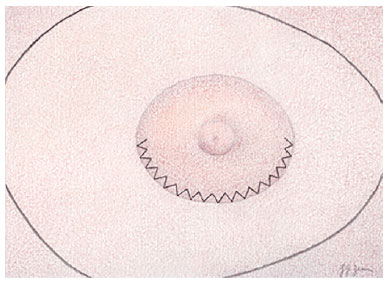
Figure 1. Markings. It is important to mark the ends of the zigzag incision at the 3 and at 9 o'clock positions, with the terminus of the zigzag at each end finishing at the inside, toward the nipple-areolar complex, to avoid inadvertent damage to the skin surrounding the areola during resection.

Figure 2. A: Preoperative markings; B: Preoperative markings (close-up).
A smaller geometric zigzag is associated with better scar camouflage. It is important to mark the ends of the zigzag incision at the 3 and at 9 o'clock positions, with the terminus of the zigzag at each end finishing at the inside, toward the nipple-areolar complex, to avoid inadvertent damage to the skin surrounding the areola during resection. In this way, possible extensions of the incision due to accidental excessive tissue removal will be restricted to the skin of the areola, which can be more easily camouflaged.
Tumescent infiltration with bupivacaine and epinephrine is performed, and the incision is made, going completely through the dermis and subcutaneous tissue. Excess breast tissue is dissected while maintaining approximately 1-cm tissue thickness below the nipple-areolar complex. After adequate hemostasis, the incision is closed in three layers. The deepest layer of sutures brings together the subcutaneous tissue. Subsequently, the dermis and finally the epidermis are closed. The peaks and troughs of the zigzag line on each side are closed with Gillies sutures using mononylon 5-0.
In both breasts of all patients, we performed liposuction with a 3.5-mm cannula through an incision in the inframammary fold at the level of the anterior axillary line.
No post-surgical drains are used in this procedure. Compression dressings are applied for 7 days.
RESULTS
Complications, including infection, vascular compromise, and necrosis of the papillary-areolar complex, delayed healing, hypertrophic scarring, pigmentation changes, or other undesirable complications, were notably absent in this patient series.
All patients were satisfied with the cosmetic result. (Figures 3, 4, 5 and 6).
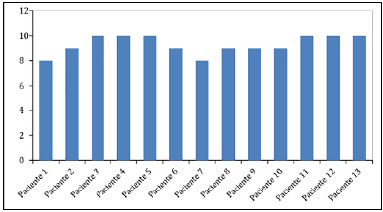
Figure 3. Patient satisfaction questionnaire.

Figure 4. A: Preoperative; B: Three months post-operative; C: Three months post-operative (close-up).
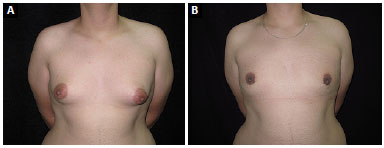
Figure 5. A: Pre-operative; B: Three months post-operative.
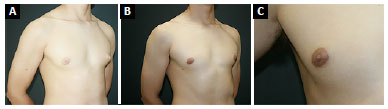
Figure 6. A: Preoperative (gynecomastia grade I); B: Three months post-operative; C: Three months post-operative (close-up).
DISCUSSION
In addition to the choice of surgical approach, discussion of some basic principles related to healing is important. In certain situations, unsightly scars can still develop despite efforts to optimize wound healing11.
Wound healing is a dynamic process, which undergoes many transformations before reaching a steady state at approximately 1 year after tissue injury. The ideal scar should be narrow and level with the surrounding skin, have good color matching, and be within or in parallel to the skin tension lines. These features make a scar less visible. Therefore, techniques that break up make or the scar line more irregular provide greater camouflage and cosmetic acceptability11.
The quality of the incision should be performed with the aim to hide the evidence of surgery. The best possible quality of the incision helps the patient to more easily accept the surgical outcome12.
The results of the present study are similar with literature data on the indices of satisfactory complications. Dornelas et al.13, in a review of 10-year gynecomastia treatment in 284 men, showed that 0.74% of patients with gynecomastia grade I or II had hypertrophic scars. Bruises and seroma developed in 2% and 3.87% of the patients, respectively. Medeiros14, when comparing the type of gynecomastia treatment based on Simon's classification, demonstrated that better results were obtained using periareolar incision when gynecomastia did not require skin resection.
So far, techniques described for the semicircular zigzag incision have been frequently described, but it was mainly used for augmentation mammoplasty15. Application of this modified incision to patients with gynecomastia has allowed greater patient satisfaction, with nearly imperceptible scars.
The aim of this technique was to achieve an irregular, more discreet, natural-looking, non-stigmatizing scar in male breast surgery.
CONCLUSION
The described incision is an excellent alternative for the treatment of gynecomastia because it provides a satisfactory cosmetic result, scar camouflage in the transitional, naturally irregular periareolar skin of the nipple-areola complex.
COLLABORATIONS
ALBP Statistical analyses; analysis and/or interpretation of data; writing the manuscript or critical review of its contents.
JGCK Statistical analyses; writing the manuscript or critical review of its contents.
WMI Analysis and/or interpretation of data; completion of surgeries and/or experiments.
PB Analysis and/or interpretation of data; completion of surgeries and/or experiments.
ASKA Analysis and/or interpretation of data; completion of surgeries and/or experiments.
RSF Final approval of the manuscript.
RG Conception and design of the study; final approval of the manuscript; completion of surgeries and/or experiments.
REFERENCES
1. Aslan G, Tuncali D, Terzioglu A, Bingul F. Periareolar-transareolar-perithelial incision for the surgical treatment of gynecomastia. Ann Plast Surg. 2005;54(2):130-4. DOI: http://dx.doi.org/10.1097/01.sap.0000143513.77819.7a
2. Prado AC, Castillo PF. Minimal surgical access to treat gynecomastia with the use of a power-assisted arthroscopic-endoscopic cartilage shaver. Plast Reconstr Surg. 2005;115(3):939-42. DOI: http://dx.doi.org/10.1097/01.PRS.0000153237.35202.7D
3. Oroz J, Pelay M, Roldán P. Ginecomastia: tratamento quirúrgico. An Sist Sanit Navar. 2005;28(Supl. 2):109-16. DOI: http://dx.doi.org/10.4321/S1137-66272005000400012
4. Piza B. Nova incisão na correção da ginecomastia. Rev Bras Cir. 1983;73(2):93-4.
5. Celebioğlu S, Ertaş NM, Ozdil K, Oktem F. Gynecomastia treatment with subareolar glandular pedicle. Discussion, 287. Aesthetic Plast Surg. 2004;28(5):281-6.
6. Arruda F, Caporossi C, Freire EL. Ginecomastia. In: Carreirão S, Cardim V, Goldenberg D, eds. Cirurgia plástica. Sociedade Brasileira de Cirurgia Plástica. São Paulo: Atheneu; 2005. p. 615-21.
7. Franco T. Cirurgia estética da mama. In: Franco T, ed. Princípios de cirurgia plástica. São Paulo: Atheneu; 2002. p. 705-12.
8. Fruhstorfer BH, Malata CM. A systematic approach to the surgical treatment of gynaecomastia. Br J Plast Surg. 2003;56(3):237-46. DOI: http://dx.doi.org/10.1016/S0007-1226(03)00111-5
9. Prado A, Castillo P. Cirugía de acceso mínimo para ginecomastia. Shaver-lipoaspiración. Rev Chil Cir. 2003;55(6):613-6.
10. McKinney P. Gynecomastia. In: Aston SJ, Beasley RW, Thorne CHM, eds. Grabb and Smith's plastic surgery. 5th ed. Philadelphia: Lippincott-Raven;1997.
11. Tenius FP, da Silva Freitas R, Closs Ono MC. Transareolar incision with geometric broken line for breast augmentation: a novel approach. Aesthetic Plast Surg. 2008;32(3):546-8. PMID: 18365269 DOI: http://dx.doi.org/10.1007/s00266-008-9145-7
12. Stuzin JM, Baker TJ, Baker TM. Refinements in face lifting: enhanced facial contour using vicryl mesh incorporated into SMAS fixation. Plast Reconstr Surg. 2000;105(1):290-301. PMID: 10627000 DOI: http://dx.doi.org/10.1097/00006534-200001000-00046
13. Dornelas MT, Machado DC, Gonçalves ALCP, Dornelas MC, Correa MPD. Tratamento cirúrgico da ginecomastia: uma análise criteriosa. Rev Bras Cir Plást. 2010;25(3):470-3. DOI: http://dx.doi.org/10.1590/S1983-51752010000300012
14. Medeiros MMM. Abordagem cirúrgica para o tratamento da ginecomastia conforme sua classificação. Rev Bras Cir Plást. 2012;27(2):277-82. DOI: http://dx.doi.org/10.1590/S1983-51752012000200018
15. Graf R, Ascenço ASK, Maluf Junior I, Lopes MC, Nasser IJG, Balbinot P, et al. Incisão periareolar em zigue-zague modificada: técnica alternativa para mastoplastia de aumento. Rev. Bras. Cir. Plást. 2013;28(2):297-300
1. Universidade Federal do Paraná, Curitiba, PR, Brazil
2. Hospital Municipal São José, Joinville, SC, Brazil
Institution: Hospital de Clínicas, Universidade Federal do Paraná, Curitiba, PR, Brazil.
Corresponding author:
André Luiz Bilieri Pazio
Rua General Carneiro, 181
Curitiba, PR, Brazil - Zip Code 80060-900
E-mail: drandrepazio@gmail.com
Article received: September 8, 2014.
Article accepted: September 23, 2017.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket