



Original Article - Year 2017 - Volume 32 -
Assessment of teaching and learning burn treatment basics among medical students
Avaliação do ensino e aprendizagem de noções básicas de tratamento de queimados entre alunos do curso de medicina
ABSTRACT
INTRODUCTION: Burns, an injury of high biopsychosocial importance, are a crucial issue in medical training, and newly graduated students face burn patients in a variety of professional settings.
METHODS: This study assessed the teaching and learning of burns among medical students at a public facility in the State of São Paulo; a specific questionnaire was applied to evaluate first year (Group 1: 54 students) and sixth year (Group 2: 60 students) medical students' knowledge about the initial care of burn patients.
RESULTS: In Group 1, there was a substantial lack of knowledge about the subject, with a general average incorrect answer rate ("errors") of 70.98% and a correct answer rate of 29.02%; in Group 2, these rates were 36.66% and 63.34%, respectively. Only 63.34% of the sixth-year students would be able to adequately conduct the treatment of a burn patient, gauged by their ability to offer a patient a better prognosis.
CONCLUSIONS: The data are disturbing, since adequate knowledge and preparation of the trainees for the care of burn patients has not been verified, and burns are emergency situations that require prompt, adequate, and efficient medical intervention to reduce patients' morbidity and mortality.
Keywords: Learning curve; Medical education; Burns; Emergency medical services; Aptitude tests.
RESUMO
INTRODUÇÃO: Agravo de grande importância biopsicossocial, queimadura é um tema crucial na formação médica, uma vez que recém-formados se deparam com pacientes que sofreram queimaduras nos mais variados cenários profissionais.
MÉTODOS: Este estudo avaliou o ensino e a aprendizagem do tema queimaduras em alunos do curso de Medicina de uma faculdade pública do Estado de São Paulo; foi aplicado um questionário específico para avaliar o conhecimento sobre o atendimento inicial ao paciente queimado na primeira série (grupo 1 - 54 estudantes), e na sexta série (grupo 2 - 60 estudantes).
RESULTADOS: Observou-se, no grupo 1, grande desconhecimento sobre o tema, com média geral de desconhecimento ("erros") de 70,98% e de acertos de 29,02%; no grupo 2, essas taxas foram de 36,66 % e 63,34 %, respectivamente. Somente 63,34% dos alunos do sexto ano conseguiriam conduzir adequadamente o tratamento de um paciente queimado e, consequentemente, oferecer a este paciente um melhor prognóstico.
CONCLUSÕES: Os dados são preocupantes, uma vez que não se verificou conhecimento nem preparo adequados dos formandos para atendimento de pacientes queimados, e que queimaduras são situações de emergência que exigem intervenção médica rápida, adequada e eficiente, a fim de reduzir a morbimortalidade das vítimas.
Palavras-chave: Curva de aprendizado; Educação médica; Queimaduras; Serviços Médicos de emergência; Testes de aptidão.
Given its social importance and impact on public health, burn treatment is a topic of paramount importance for medical training. According to Shahrokhi et al.1, medical education in burns can be divided into three main components: surgical education, inter-professional education, and mentorship.
Historically, the traditional method of education in the practice of surgery was the hospital-centric model, initially described by William Halsted more than 100 years ago1. The acquisition of competences is dependent on observation, assistance, and subsequently performance of the task, classically known as "see one, do one, and teach one". However, with the advance of technology and concern for patient safety and "medical errors", there has been a demand for innovation in surgical education1.
Newly trained physicians are faced with patients who have been burned in a variety of professional settings: emergency medicine, trauma, pre-hospital care, plastic surgery, dermatology, and general practice, so it is essential for medical students to have significant knowledge about burn management2.
A study by Egro and Estela2 in 2014 reports that poor knowledge on the diagnosis and initial care in burns could potentially lead to mismanagement by doctors.
OBJECTIVE
The purpose of this study is to indirectly evaluate how medical training is preparing medical students for the primary care of burns.
We aim to (1) verify whether there is a significant difference between the performance of first year (1st grade) and last year (6th grade) students of the Medical School of Marília (FAMEMA), (2) describe the distribution of age and gender among these students, (3) find out if there is a significant difference in the number of errors and correct answers to the problem cases, (4) find out if there is a greater number of correct answers among students who previously did some extracurricular course on the subject or who attended another college in the health area, and (5) verify if in less complex burn cases there is a greater convergence between the answers given by the students or a greater number of correct answers.
METHODS
This study aims to provide quantitative and qualitative information regarding first and last year medical students' knowledge regarding the conduct and prognosis of burn cases. A questionnaire was applied consisting of questions about the students' identification, knowledge about the initial attendance in burns, and whether they used other sources of knowledge about the subject besides those available from the FAMEMA faculty.
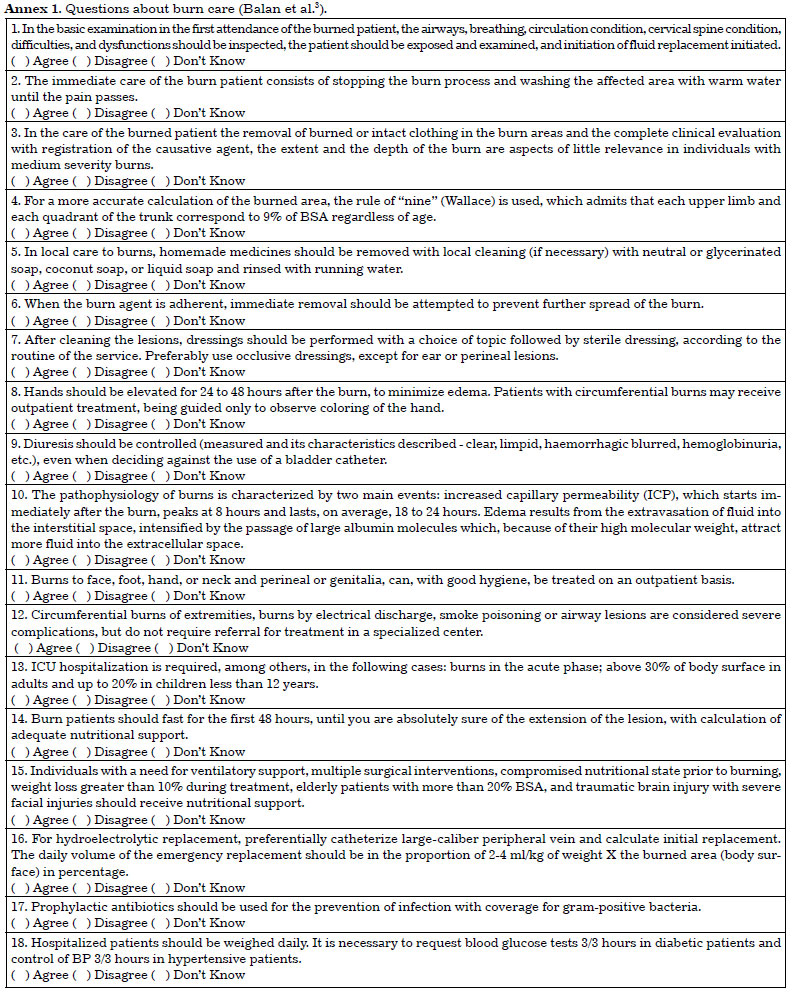
The questionnaire (Annex 1) was constructed and validated through the study "Construction of a questionnaire to analyze the knowledge about the initial attendance of burns", performed in 20083.
Study population
Students of the first and last years of the 2015 FAMEMA medical course were interviewed. First year students were interviewed during the first two months of the medical course. The students of the last (sixth) year were interviewed in the last two months of the course. The ideal size of the study population was 160 subjects, divided into 80 first year students and 80 sixth year FAMEMA medical students.
Inclusion criteria
The only inclusion criterion was being a first or last year medical student at FAMEMA in 2015.
Exclusion criteria
The only exclusion criterion was refusing to participate in the study.
Ethical aspects
This research was approved by the Research Ethics Committee of the Faculdade de Medicina de Marília (FAMEMA - Faculdade de Medicina de Marília) - CAAE: 37178914.0.0000.5413. All participants were informed about the purpose of the research and signed an Informed Consent Form after agreeing to participate.
Data Analysis
Data were transcribed into a spreadsheet and only comparative analysis (percentages) was used for the quantitative analysis. Data obtained were compared with published literature.
RESULTS
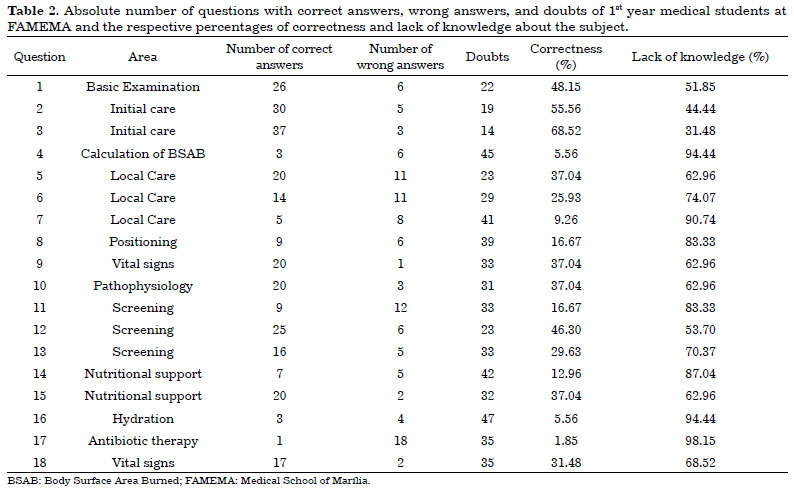
For the assessment of students' general knowledge about burn treatment, the following areas were selected: concept of burns, classification of severity, calculation of body surface area burned (BSAB) in adult patients and children, pathophysiology, basic examination, immediate and initial care, lesions by inhalation, local care, positioning the victim, fluid replacement, screening of burns, analgesia, antibiotic therapy, vital signs, and nutritional support (Table 1).

The questionnaire was applied to 160 first and sixth year medical students at FAMEMA. Of these, 46 refused to participate in the study (26 first year students and 20 sixth year students). Thus, the Group 1 sample was composed of 54 students (47.37% of the total), and the Group 2 sample by 60 students (52.63% of the total). There were 68 female students (59.65%) and 46 male students (40.35%). Among the students, only five (4.39%) had received prior higher education. The overall mean age was 23.93 years.
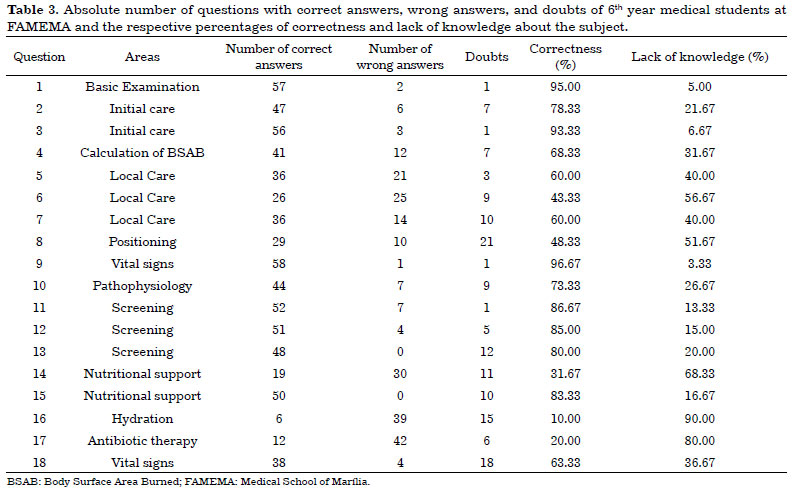
In the questions that addressed basic examination and the immediate and initial care in the first burn care (questions 1, 2 and 3 of the questionnaire), the success rate in Group 1 was 48%, 55%, and 68% respectively, and 95%, 78.33%, and 93.33% in Group 2. For lack of knowledge, it was 51.85%, 44.44%, and 31.48% in Group 1 and 5%, 21.67%, and 6.67% in Group 2.
The failure rate in question 4, which addresses knowledge of the calculation of burned body surface in adults and children, was 94.44% and the success rate was 5% in the first year (Group 1); in the sixth year (Group 2), these indices were 31.67% and 68.33%, respectively.
Questions 5, 6 and 7 assess knowledge about local care in first attendance to burn, and yielded success rates of 37%, 26%, and 9%, and failure rates of 62.96%, 74.07%, and 90.74% in Group 1. In Group 2 the rates were 60%, 43.33%, and 60%, and 40.0%, 56.67%, and 40.0%, respectively.
In questions 8 and 9 the positioning and control of the patient in medical care were addressed, and success rates obtained were, respectively, 16% and 37% in Group 1 and 48.33% and 96.67% in Group 2. The failure rate was 83.33% and 62.96% in Group 1 and 51.67% and 3.33% in Group 2.
The tenth question of the questionnaire was about the pathophysiology of burns. The percentage of correct responses was 37% and the failure rates were 62.96% in Group 1. In Group 2, the success rate was 73.33% and the failure rate was 26.67%.
Questions 11, 12 and 13 were on screening of burns and the rates of correct answers were 16%, 46% and 29%, while incorrect answers were 83.33%, 53.70%, and 70.37% in Group 1. In Group 2, the rates of correct answers were 86.67%, 85%, and 80%, while incorrect answers were 13.33%, 15%, and 20%.
In questions 14 and 15, the subject was nutritional support of the patient. The rates of correct answers were 13% and 37%, and failure rates were 87.04% and 62.96% for Group 1. The rates for Group 2 were 31.67%, 83.33% correct answers, and 68.33% and 16.67% incorrect answers.
Question 16 was about the initial volume administered in the burned patient, and yielded 5% correct answers and 94.44% incorrect answers in Group 1, and 10% correct answers and 90% incorrect answers in Group 2.
Incorrect answers to Question 17 dealt with antibiotic therapy in burn patients. In Group 1 there were 98.15% incorrect answers and, and 1% correct answers. In Group 2 there were 20% correct answers and 80% incorrect answers.
For question 18, which dealt with vital signs in burn patients, Group 1 had 31% correct answers and 68.52% incorrect answers. Group 2 had 63.33% correct answers and 36.67% incorrect answers (for details of results, see Tables 2 and 3).
DISCUSSION
Burns are traumatic injuries generated by contact with heat, cold, chemical substances, electricity, or radioactivity, which cause partial or total destruction of the skin and its attachments, leaving physical and/or psychological sequelae in victims4,5.
Burns are considered a public health problem by the World Health Organization (WHO)6. In 2004 alone, there were approximately 11 million serious burns that underwent a medical procedure worldwide, surpassing the incidence of highly prevalent diseases such as tuberculosis and HIV4.
More than 300,000 deaths per year are caused by fire burns, and this number is much higher when considering burns of other etiologies. Mortality due to burns is greater in developing or underdeveloped countries, corresponding to 95% of the total number of deaths caused by burns worldwide6.
In developed countries, the mortality due to burns in males is higher than in females (ratio of 2:1) in the age range of 15-59 years, while in underdeveloped countries the death rate in women is 2- to 3-fold higher in the same age group4. In Egypt, 9% of the deaths of women of childbearing age are caused by burns. In India, approximately 65% of deaths due to burns occur with women, usually related to domestic accidents, self-mutilation, and domestic violence4.
A prospective study, conducted from April 2000 to March 2005 in Hong Kong7, revealed 264 children admitted to the Burns Unit of the Prince of Wales Hospital, with a predominance of males in all age groups, and with scalding the most common etiology7. Another study8, published in 2008 and carried out at the CHU IbnRochd National Burn Center in Casablanca, Morocco, found that 543 burned children were admitted in the service (45.7% of the total), 96.5% of whom were suffering from thermal burns, with a predominance of 1-5 year olds and the majority (63.5%) being male.
In 2009, 80,607 hospitalizations were performed in the Unified Health System (SUS) in Brazil due to injuries resulting from burns. There was a predominance of men compared to women (58.6%), and the most affected age groups were young adults (23.1%) and children (22%), with predominance of children under 4 years of age (16%)5.
In Brazil, external agents, such as burns, are the main cause of deaths in the age group from 1 to 14 years, contributing to high rates of infant mortality. In the case of burns, the sequelae also have great social impact: for each death, there are four children with physical sequelae and 100% of the survivors have some form of psychological sequelae9. In the SUS data for 2015, available through DATASUS (http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sih/cnv/fiuf.def), 7,147 urgent hospitalizations were performed and R$ 9,795,595.31 (approximately US $ 3,000,000.00) were spent with hospital services due to accidents due to contact with heat sources and hot substances.
Peets et al.10 have noted that curricular content is currently based on the opinions of some doctors and directors of educational institutions rather than on protocols. Accordingly, the curricula, when it comes to the care of serious patients, such as burn victims, may not meet the students' educational needs. The pathologies selected in the study were: respiratory arrest, cardiac arrhythmias, hemorrhagic shock, electrolyte disturbances and acid-base balance, convulsion, cardiac arrest, overdose, and drug withdrawal, in addition to polytrauma and sepsis. Based on this, it is noted that the topic "burns" is not often addressed in the medical curriculum. However, the adequate preparation of the professionals for the emergency care of burn patients is of critical importance.
A study conducted in the Kilimanjaro Christian Medical Center found that most of the burn patients did not receive adequate emergency conduct, which culminated in prolonged hospital stays and increased mortality11. In a prospective observation12 performed at Royal Perth Hospital, Australia, 227 burn patients were attended to, but only 88 (39%) received appropriate first aid and 50% of the patients received inappropriate first aid.
In the assessment performed in the present study, in Group 1 (first year medical students), there was a large rate of general ignorance on the subject "burns", with a general average lack of knowledge ("errors") of 70.98 % and correct answers of 29.02%; in Group 2 (sixth year medical students) these rates were 36.66% and 63.34%, respectively. This verifies that the learning in the primary care of burns yielded a higher percentage of correct answers among the last year medical students in the sample studied.
However, only 63.34% of the sixth-year students would theoretically manage to treat a burned patient as expected. The data are troublesome, as the lack of knowledge of the last year medical students occurred particularly in relation to local care, nutritional support, hydration, and administration of antibiotics, subjects of fundamental importance in these cases; the good use of time in these cases is fundamental and a determining factor of the prognosis13.
The highest rates of correct answers in Group 1 were in basic examination and immediate and early care in the first burn attendance, where they demonstrated greater knowledge on basic themes. However, due to the importance of the initial approach of the burn patients for their survival, and the fact that the general knowledge about such topics is expected for first year medical students, an average percentage of correct answers of 57% is considered inadequate, and we can therefore say that students' medical education has been inadequate from the beginning. The contemplation of themes about local care, medical management, and pathophysiology in the syllabus of the first year of medical school was not expected, and the average lack of knowledge found in the sample was high, at 64%.
As Group 1 comprised newly graduated high school students, we can also infer how poor health education is in primary and secondary schools. As in our study, one conducted by Rea et al.12 pointed out that first aid education is not adequately provided in Australia. They observed that first year university students performed poorly on a questionnaire about initial approaches to burns. Nevertheless, schools play an important and growing role in promoting health, and preventing illness and accidents among children and adolescents14.
In our study, the final year medical students (Group 2) performed well in the basic examination and immediate burn care domains, in agreement with Lemon et al.15, who obtained satisfactory results in first aid in burns. However, in the local care domains in primary care for burns, we obtained low percentages of correct answers, as was the case in the study conducted by Rea et al.12, whose objective was to verify the knowledge of the initial approach in burns among health professionals - this initiative found that only 18.8% of respondents achieved correct answers.
It is important to emphasize that emergency situations require immediate intervention, conducted quickly and efficiently, aiming at reducing the morbidity and mortality of the victims, an important focus area in medical training13. Skinner and Peat16, in 2002, emphasized that burn injuries, when conducted with appropriate first care, are associated with more favorable outcomes, restricting tissue damage, the need for surgeries, and morbidity.
In the analysis of the knowledge of pathophysiology of burns, the present study had 73.33% correct answers in Group 2. Lemon et al.15 analyzed the same domain (knowledge of the pathophysiology of burns) with four questions, obtaining correct answers of 88%, 83%, 36%, and 92%, which may be considered acceptable in the two studies (the present study and that of Lemon et al15). Generally, in the two groups analyzed in this study, the theoretical knowledge in burns was higher than the practical. A previous study performed by Chakravarthy et al.17 pointed out that teaching in emergency medicine demands practical training with simulations to achieve the desired efficacy.
Unfortunately, in this study, Group 2 revealed a significant lack of knowledge about the calculation of body surface area burned in adults and in children (68.33%) and the initial fluid replacement volume to be administered (90%). Such calculations are fundamental in the first care given to patients who are burned in the emergency room, since adequate hydration in the first hours after trauma is directly related to survival rates18.
In the UK alone, around 175,000 burn patients are attended to in emergency rooms per year and 13,000 in the Netherlands19. In Brazil, there is no specific survey on such attendance, but, being a third world country, very high numbers are expected. Once again, we are concerned about the extent to which our students are prepared for emergencies, particularly in the case of burns.
In a study conducted by Lemon et al.15 in the United Kingdom, only 45% of the students had formal education in burns, 20% had teaching unrelated to the college curriculum, and 35% had no related teaching. In previous studies, it was shown that only 13% of English schools teach burns in a structured manner, and of the 29 colleges interviewed, the maximum time allowed for the subject throughout the entire undergraduate course is 4 hours, not very different from that which we observe in the day-to-day of our institution.
FAMEMA has only one activity of formal education for burns, and it is only 2 hours long. Comparing it with the study conducted by Lemon et al.15, our students have only half the time to receive "formal education" in burns.
The reduced weightage of the specialty of Plastic Surgery in the medical curriculum, and consequently of the theme "burns", is very much related to the fact that this specialty is often only thought of in its aesthetic components. A 2006 survey20 showed that 93% of medical students rated "cosmetic surgery" as the core of the Plastic Surgery specialty during an assessment of the medical curriculum.
CONCLUSION
Although sixth year students had higher rates of correct answers than first year students did, there was still insufficient knowledge and preparation for burn patient care. This is disturbing, as burns are emergency situations that require prompt, adequate, and efficient medical intervention to reduce the morbidity and mortality of the victims.
COLLABORATIONS
GM Analysis and/or interpretation of data; final approval of the manuscript; conception and design of the study; completion of surgeries and/or experiments; writing the manuscript or critical review of its contents.
AFM Final approval of the manuscript; completion of surgeries and/or experiments; writing the manuscript or critical review of its contents.
LRMS Analysis and/or interpretation of data; final approval of the manuscript; conception and design of the study; completion of surgeries and/or experiments; writing the manuscript or critical review of its contents.
REFERENCES
1. Shahrokhi S, Jindal K, Jeschke MG. Three components of education in burn care: surgical education, inter-professional education, and mentorship. Burns. 2012;38(6):783-9. DOI: http://dx.doi.org/10.1016/j.burns.2012.01.012
2. Egro FM, Estela CM. The need for burns teaching: a cross-sectional study to assess burns teaching in the United Kingdom. Burns. 2014;40(1):173-4. PMID: 24238672 DOI: http://dx.doi.org/10.1016/j.burns.2013.10.001
3. Balan MAJ, Meschial WC, Santana RG, Suzuki SM, Oliveira MLF. Validation of an instrument for investigating knowledge on the initial assistance to burns victims. Text Context Nursing. 2014:23(2):373-81. DOI: http://dx.doi.org/10.1590/0104-07072014000380013
4. Peck MD. Epidemiology of burns throughout the world. Part I: Distribution and risk factors. Burns. 2011;37(7):1087-100. PMID: 21802856 DOI: http://dx.doi.org/10.1016/j.burns.2011.06.005
5. Gawryszewski VP, Bernal RTI, Silva NN, Morais Neto OL, Silva MM, Mascarenhas MDM, et al. Sá NN. Public hospital emergency department visits due to burns in Brazil, 2009. Cad Saúde Pública. 2012;28(4):629-40. DOI: http://dx.doi.org/10.1590/S0102-311X2012000400003
6. Burn prevention: success stories and Lessons Learned [internet]. Geneva: World Heath Organization; 2011. [cited 2017 Oct 30]. Available from: http://www.who.int/violence_injury_prevention/publications/other_injury/burn_success_stories/en/
7. Tse T, Poon CH, Tse KH, Tsui TK, Ayyappan T, Burd A. Paediatric burn prevention: an epidemiological approach. Burns. 2006;32(2):229-34. DOI: http://dx.doi.org/10.1016/j.burns.2005.08.025
8. Zahid A, Atannaz J, Alaoui M, Rafik A, Ezzoubi M, Diouri M, et al. Epidemiological profile of children burns admitted at the National Center for Brules, Morocco. Ann Burns Fire Disasters. 2011;24(4):171-4.
9. Millan LS, Gemperli R, Tovo FM, Mendaçolli TJ, Gomez DS, Ferreira MC. Epidemiological study of burns in children treated at a tertiary hospital in São Paulo. Rev Bras Cir Plást. 2012;27(4):611-5. DOI: http://dx.doi.org/10.1590/S1983-51752012000400024
10. Peets AD, McLaughlin K, Lockyer J, Donnon T. So much to teach, so little time: a prospective cohort study evaluating a tool to select content for a critical care curriculum. Crit Care. 2008;12(5):R127. DOI: http://dx.doi.org/10.1186/cc7087
11. Ringo Y, Chilonga K. Burns at KCMC: epidemiology, presentation, management and treatment outcome. Burns. 2014;40(5):1024-9. DOI: http://dx.doi.org/10.1016/j.burns.2013.10.019
12. Rea S, Kuthubutheen J, Fowler B, Wood F. Burn first aid in Western Australia--do healthcare workers have the knowledge? Burns. 2005;31(8):1029-34.
13. Maia ER, Gonçalves Júnior J, Lima EP, Campos W, Jovino EM, Fernandes FF, et al. Conhecimentos em atenção pré-hospitalar e suporte básico de vida por estudantes recém-ingressos de medicina. Rev Bras Educ Méd. 2014;38(1):59-64. DOI: http://dx.doi.org/10.1590/S0100-55022014000100008
14. Liberal EF, Aires RT, Aires MT, Osório AC. Safe school. J Pediatr (Rio J). 2005;81(5 Suppl):S155-63. DOI: http://dx.doi.org/10.1590/S0021-75572005000700005
15. Lemon TI, Stapley S, Idisis A, Green B. Is the current UK undergraduate system providing junior doctors knowledge and confidence to manage burns? A questionnaire-based cohort study. Burns Trauma. 2015;3:6. DOI: http://dx.doi.org/10.1186/s41038-015-0005-9
16. Skinner A, Peat B. Burns treatment for children and adults: a study of initial burns first aid and hospital care. N Z Med J. 2002;115(1163):U199.
17. Chakravarthy B, Ter Haar E, Bhat SS, McCoy CE, Denmark TK, Lotfipour S. Simulation in medical school education: review for emergency medicine. West J Emerg Med. 2011;12(4):461-6. DOI: http://dx.doi.org/10.5811/westjem.2010.10.1909
18. Dougherty W, Waxman K. The complexities of managing severe burns with associated trauma. Surg Clin North Am. 1996;76(4):923-58. PMID: 8782481 DOI: http://dx.doi.org/10.1016/S0039-6109(05)70488-6
19. British Burn Association Standards. National Burn Care Review. [acesso 2017 Out 31]. Disponível em: http://www.britishburnassociation.org/downloads/NBCR2001.pdf
20. Parikh AR, Clarke A, Butler PE. Plastic surgery and the undergraduate medical school curriculum. Med Educ. 2006;40(5):476-7. PMID: 16635148 DOI: http://dx.doi.org/10.1111/j.1365-2929.2006.02425.x
1. Faculdade de Medicina, Universidade de Marília, Marília, SP, Brazil
2. Faculdade de Ciências Médicas, Universidade Estadual de Campinas, Campinas, SP, Brazil
3. Faculdade de Medicina de Marília, Marília, SP, Brazil
4. Sociedade Brasileira de Cirurgia Plástica, São Paulo, SP, Brazil
Institution: Faculdade de Medicina de Marília, Marília, SP, Brazil.
Corresponding author:
Luís Ricardo Martinhão Souto
Avenida Santo Antonio, 60, Apto. 130
Marília, SP, Brazil - Zip Code 17501-470
E-mail: lrmsouto@yahoo.com.br
Article received: June 5, 2017.
Article accepted: September 23, 2017.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket