



Original Article - Year 2017 - Volume 32 -
Evaluation of pressure parameters intra-abdominal and thoracic in patients submitted to abdominoplasty
Avaliação dos parâmetros pressóricos intra-abdominal e pulmonar em pacientes submetidos à abdominoplastia
ABSTRACT
INTRODUCTION: The abdomen is an important aesthetic and functional segment in the characterization of body contouring. The plication of the rectus abdominis may cause various problems to the patient such as increased intra-abdominal and thoracic pressure. Thus, this study aims to evaluate abdominal pressure and pulmonary parameters in patients undergoing abdominoplasty with liposuction.
METHODS: This is a descriptive longitudinal prospective study. All patients underwent the lipoabdominoplasty with liposuction of flanks by the same senior plastic surgeon. The intra-abdominal pressure was measured by a device attached to indwelling urinary catheter of the patient and intra-thoracic pressure was measured by the ventilation device monitor. Measurements were made before and after plication and in Fowler's position.
RESULTS: Mean surgery time was 4 hours and 08 minutes. Intra-abdominal pressure before and after plication of the rectus abdominis ranged from 2 to 11 cm H2O and 5-16 cm H2O, respectively. Intra-thoracic pressure before and after plication of the rectus abdominis ranged from 13 to 17 cm H2O and 14-18 cm H2O respectively. The intra-abdominal pressure in Fowler's position ranged from 6 to 23 cm H2O. The intra-thoracic pressure in Fowler's position ranged from 15 to 19 cm H2O. One case of small dehiscence, one case of seroma and one case of respiratory distress were observed.
CONCLUSION: The results demonstrate that plication of the rectus abdominis increases intra-abdominal and pulmonary pressure without generating significant systemic changes.
Keywords: Abdominoplasty; Pressure; Rectus abdominis.
RESUMO
INTRODUÇÃO: O abdome é um segmento estético-funcional importante na caracterização do contorno corporal. A confecção da plicatura do reto abdominal pode ocasionar diversos transtornos como o aumento da pressão intra-abdominal e torácica. Assim, este estudo tem como objetivo avaliar os parâmetros de pressão abdominal e pulmonar em pacientes submetidos à abdominoplastia com lipoaspiração.
MÉTODOS: Estudo longitudinal prospectivo descritivo. As pacientes foram submetidas à lipoabdominoplastia com lipoaspiração de flancos pelo mesmo cirurgião plástico sênior. A mensuração da pressão intra-abdominal foi feita por meio do uso de um dispositivo acoplado à sonda vesical de demora do paciente e a pressão intratorácica foi aferida por meio do monitor do aparelho de ventilação. As medições foram feitas antes e após a plicatura e durante a posição de Fowler.
RESULTADOS: O tempo médio do ato operatório foi de 4 horas e 8 minutos. A pressão intra-abdominal antes e após a plicatura do músculo reto abdominal variou de 2 a 11 cm H2O e 5 a 16 cm H2O, respectivamente. A pressão intratorácica antes e após a plicatura do músculo reto abdominal variou de 13 a 17 cm H2O e 14 a 18 cm H2O, respectivamente. A pressão intra-abdominal em posição de Fowler variou de 6 a 23 cm H2O. A pressão intratorácica em posição de Fowler variou de 15 a 19 cm H2O. Foi observado um caso de deiscência, um caso de seroma e um caso de desconforto respiratório.
CONCLUSÃO: Os resultados elucidam que a plicatura do reto abdominal ocasiona o aumento da pressão intra-abdominal e pulmonar sem gerar alterações sistêmicas significativas.
Palavras-chave: Abdominoplastia; Pressão; Reto do abdome.
The abdominal and chest walls are anatomical structures that provide protection of organs to maintain physiological functions such as the position of the organs inside them during changes of gravitational forces1. The abdomen is an important aesthetic and functional segment in the characterization of body contouring. Abdominoplasty is one of the most frequent aesthetic procedures and in combination to the plication of the aponeurosis of the rectus abdominis muscle it restores a graceful and youthful appearance of this unit2.
The plication of the rectus abdominis should take into consideration some measurement values. The width of the linea alba is considered normal when its measurements are smaller than 22 mm about three centimeters above the navel and up to 16 mm about two centimeters below the navel3.
If not properly performed, the completion of this step in abdominoplasty may cause several problems to patients. Increased intra-abdominal pressure caused by plication of the rectus abdominis may lead to abdominal compartment syndrome in addition to increased pulmonary morbidity with impaired respiratory function by increasing intra-thoracic pressure4,5.
In recent years, especially in the last decade, modifications and improvements have been added to the procedure, aiming at obtaining more satisfactory results and decreasing complications. The correct use of the technique in addition to patient monitoring provides safety and satisfactory postoperative cosmetic results5,6.
OBJECTIVE
Therefore, this study aims to evaluate abdominal and pulmonary pressure parameters in patients undergoing abdominoplasty with liposuction.
METHODS
This is a descriptive longitudinal prospective study carried out from December 2015 to July 2016 at the plastic surgery service of senior author in Brasilia. Pressure measurements were assessed before and after plication of the rectus abdominis and in Fowler's position.
This research project has followed the legal procedures established by the National Health Council Resolution 196/96 with regard to research involving human subjects and was subjected to examination and approval of the Research Ethics Committee, UNIEURO University Center, Brasília under registration no. 1.578.501.
Because this was a prospective study, all patients signed the Free Informed Consent Form (IC).
The sample was intentional and based on profiles of patients undergoing abdominoplasty with liposuction from December 2015 to July 2016. The database for the development of this research was collected intraoperatively by the study authors.
The study variables were age, gender, postoperative surgical complications, body mass index (BMI), duration of surgery, weight of the abdominal specimen, total amount of liposuction fat, hospital stay and complete diuresis after surgery.
The distances between the inner borders (supra umbilical, infra umbilical and umbilical) of the rectus abdominis, as well as intra-abdominal and thoracic pressure values before and after plication of the rectus abdominis and in Fowler's position were assessed.
All patients undergoing abdominoplasty during the study period were included in the analysis. Patients who refused to participate were excluded.
Surgical technique
To equalize the sample, all patients underwent a classic lipoabdominoplasty with liposuction of flanks by the same senior plastic surgeon, in the same operating room to maintain the same surgical and anesthesia team. It began with an arcuate incision in the lower abdomen (after previous demarcation) with detachment of the skin-fat flat at the level of the xiphoid process and followed by tunneling of the flap after releasing the umbilical scar.
Before plication, the distance of the inner borders (supra umbilical, infra umbilical and umbilical) of the rectus abdominis was measured with the aid of a surgical ruler and intra-abdominal and pulmonary pressure values were obtained.
The plication of the rectus abdominis muscle was performed in all patients using simple stiches with nylon 2-0 in a single layer.
After plication, a new intra-abdominal and pulmonary pressure measurement was performed.
Intra-abdominal and pulmonary pressure evaluation
Abdominal pressure was measured indirectly using a device connected to the patient's urinary catheter. The device consisted of a ruler (which was coupled to a zero-frame holder at the level of the patient's pubic symphysis) with a HartmannTM device used to measure central venous pressure, which was connected to a 500 ml bag of saline solution stained with methylene blue (1 ml) for easy reading (Figure 1). For pressure measurement, the system was properly calibrated and connected to the patient's urinary catheter (with a previously emptied bladder and infused with 100 ml of 0.9% saline solution), and was clamped during the measurement procedure.
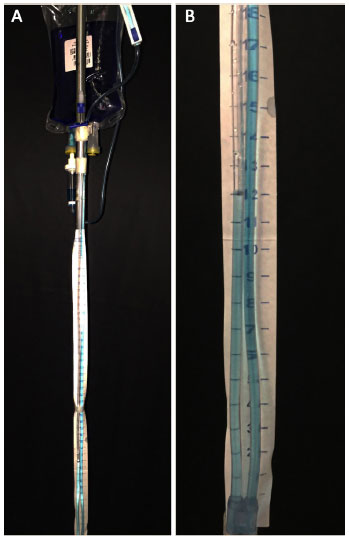
Figure 1. A: The intra-abdominal pressure measurement system is attached to a 500 ml bag of saline solution stained with 1 ml of methylene blue to facilitate reading; B: Abdominal pressure value after plication of the rectus abdominis muscle.
Pulmonary pressure was measured indirectly with the aid of a DrägerTM device (Fabius plus model) used for mechanical ventilation monitoring (Figure 2). To equalize the sampling, all patients underwent general and epidural anesthesia using the same monitoring device, which was properly calibrated.

Figure 2. Device used for pulmonary pressure measurement.
Statistical analysis
Statistical analysis was based on the results obtained, which were organized in a Microsoft Excel 2008 spreadsheet and analyzed by Epi Info software, version 3.5.1, and BioEstat software, version 5.0.
RESULTS
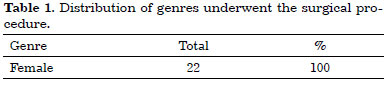
We analyzed 22 female patients undergoing surgical procedure (Table 1).
Patient's age ranged from 22 to 51 years, mean of 34 years.
Mean BMI was 25.6 kg/m2.
Mean surgery time was 4 hours and 08 minutes.
Hospital stay ranged from 24 to 48 hours.
The weight of the surgical specimens ranged from 1.54 to 3.45 kg, with mean of 3.06 kg.
The mean amount of liposuction fat removed was 3.02 L.
The total diuresis ranged from 1.32 L to 2.15 L, with a mean of 1.68 L.
The distance from the inner border of the supra umbilical rectus abdominis muscles ranged from 44 a 82 mm, with mean of 67.3 mm. The distance from the inner border of the umbilical rectus abdominis muscles ranged from 42 a 81 mm, with a mean of 65.6 mm. The distance from the inner border of the infra-umbilical rectus abdominis muscles ranged from 39 to 77 mm, with a mean of 61.9 mm.
Intra-abdominal pressure before and after plication of the rectus abdominis ranged from 2 to 11 cm H2O (mean 8.5 cm H2O) and 5 to 16 cm H2O (mean 12.3 cm H2O), respectively. The intrathoracic pressure before and after plication of the rectus abdominis ranged 13 to 17 cm H2O (mean 14.7 cm H2O) and 14-18 cm H2O (mean 16.2 cm H2O), respectively. The intra-abdominal pressure in Fowler's position ranged from 6 to 23 cm H2O (mean 18.2 cm H2O). The intrathoracic pressure in Fowler's position ranged from 15 to 19 cm H2O (mean 17.5 cm H2O).
In our study, we observed one case of small dehiscence, which was treated conservatively. There was also one case of seroma treated by serial punctures and lymphatic drainage and 1 case of respiratory distress, which was treated with physical therapy and non-invasive ventilation.
There were no surgical complications such as hematoma, pulmonary embolism, deep vein thrombosis (DVT), flap necrosis and/or infection (Table 2).
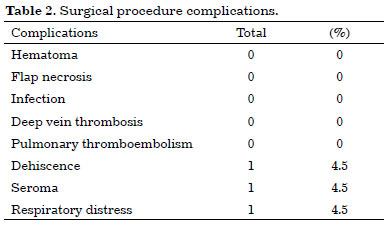
Figure 3 illustrates the result obtained with the procedure.
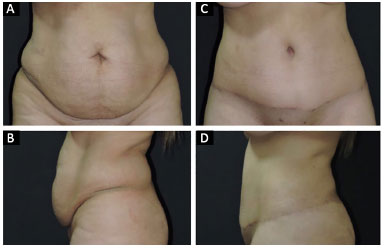
Figure 3. Patient undergoing classic abdominoplasty. A and B: Preoperative; C and D: Postoperative.
DISCUSSION
The plication of the aponeurosis of the rectus abdominis muscle aims to restore the integrity of the abdominal wall, reinforcing the musculoaponeurotic layer of the abdomen. Different techniques are reported in the literature, however, the plication of the anterior sheath remains the most used7, and is the one used in this study.
Increased intra-abdominal pressure caused by excessive musculoaponeurotic plication may cause several complications for the patient, among them the abdominal compartment syndrome, first reported by Étienne-Jules Marey in 18938,9.
For intra-abdominal pressure measurement, various techniques are described in the literature. However, the intravesical method is the most reproducible and feasible for evaluation being considered the gold standard by the World Society of the Abdominal Compartment Syndrome9, which was used in our study.
The normal values of intra-abdominal pressure range from 0 to 16.3 cm H2O, reaching 20-25 cm H2O postoperatively and 34 cm H2O in critical patients10.
Intra-abdominal hypertension is characterized by sustained intra-abdominal pressure increases above 16. cm H2O. It may be classified as moderate (16.3 to 20.4 cm H2O), severe (22-27 cm H2O), moderate compartment syndrome (28.5 to 34 cm H2O) and severe compartment syndrome (> 34 cm H2O)10.
In our study we found that all patients undergoing the surgical procedure were female. Intra-abdominal pressure before plication (2-11 cm H2O) was within normal range. A high pressure after plication of the rectus abdominis (5-16 cm H2O) with a slight reduction in Fowler's position (6 to 23 cm H2O) was observed. Despite the increased pressure observed, there was no systemic involvement since postoperative diuresis was within the normal range (1.32 L to 2.15 L)
Oneal et al.11 conducted a prospective study of eight patients undergoing abdominoplasty with extensive plication of the rectus abdominis muscles. Patients had intravesical pressure monitored. Intravesical pressure did not reach more than fifteen centimeters of water above pre-operative levels in any of the patients. During the procedure, none of the patients had ventilation difficulties.
The results obtained in our study were similar to those obtained by Oneal et al.11. We did not obtain any increase greater than fifteen centimeters of water above preoperative levels in the intravesical pressure.
Abramo et al.12 conducted a study with 20 patients undergoing abdominoplasty with treatment of the musculoaponeurotic plane. Measurements of pulmonary pressure were performed intraoperatively before plication (20-21 cm H2O), immediately after plication (25-30 cm H2O) and at the end of the procedure (20-24 cm H2O). There were no thromboembolic complications.
The results obtained in our study showed intrathoracic pressure before (13-17 cm H2O) and after (14-18 cm H2O) plication of the rectus abdominis similar to those obtained in the study by Abramo et al.12 and there were no thromboembolic complications.
Finally, it is known that intra-abdominal pressure increase caused by plication of the aponeurosis may contribute to increased pulmonary morbidity postoperatively. However, other factors must be taken into account for respiratory involvement, including Fowler's position (semi-seated) required in the postoperative and the use of a tight surgical girdle13,14.
In our study, we observed an increase in both abdominal (6-23 cm H2O) and intra-thoracic (15-19 cm H2O) pressure during Fowler's position, which corroborates the studies described in the literature.
Among the complications obtained in this study, the authors highlight a case of respiratory distress in a patient on the first postoperative day. During hospitalization, the patient received support with non-invasive ventilation and respiratory therapy and was discharged on the second postoperative day. The patient progressed without complications.
CONCLUSION
The results of this study imply that the surgical repair of the rectus abdominis muscle diastasis by plication of the anterior layer of the rectus abdominis sheath restores a graceful appearance and increases intra-abdominal and lung pressure after the plication of the rectus abdominis muscle and in Fowler's position. However, it does not cause significant systemic alterations when performed safely and following all technical principles in patients undergoing abdominoplasty.
COLLABORATIONS
JDLGA Final approval of the manuscript; completion of surgeries and/or experiments.
DASS Statistical analyses; conception and design of the study; writing the manuscript or critical review of its contents.
JGOJ Completion of surgeries and/or experiments.
LMCD Analysis and/or interpretation of data; conception and design of the study.
LGM Conception and design of the study.
FCA Completion of surgeries and/or experiments.
EFR Completion of surgeries and/or experiments.
JCD Final approval of the manuscript.
REFERENCES
1. Nahas FX, Augusto SM, Ghelfond C. Should diastasis recti be corrected? Aesthetic Plast Surg. 1997;21(4):285-9. PMID: 9263554
2. Dini GM, Ferreira LM. Putting the umbilicus in the midline. Plast Reconstr Surg. 2007;119(6):1971-3. PMID: 17440407 DOI: http://dx.doi.org/10.1097/01.prs.0000259800.70743.3c
3. Beer GM, Schuster A, Seifert B, Manestar M, Mihic-Probst D, Weber SA. The normal width of the linea alba in nulliparous women. Clin Anat. 2009;22(6):706-11. DOI: http://dx.doi.org/10.1002/ca.20836
4. Saggi BH, Sugerman HJ, Ivatury RR, Bloomfield GL. Abdominal compartment syndrome. J Trauma. 1998;45(3):597-609. PMID: 9751558 DOI: http://dx.doi.org/10.1097/00005373-199809000-00033
5. Talisman R, Kaplan B, Haik J, Aronov S, Shraga A, Orenstein A. Measuring alterations in intra-abdominal pressure during abdominoplasty as a predictive value for possible postoperative complications. Aesthetic Plast Surg. 2002;26(3):189-92. PMID: 12140697 DOI: http://dx.doi.org/10.1007/s00266-001-1469-5
6. da Silva DB, Nahas FX, Bussolaro RA, de Brito MJ, Ferreira LM. The increasing growth of plastic surgery lawsuits in Brazil. Aesthetic Plast Surg. 2010;34(4):541-2. DOI: http://dx.doi.org/10.1007/s00266-009-9460-7
7. Tadiparthi S, Shokrollahi K, Doyle GS, Fahmy FS. Rectus sheath plication in abdominoplasty: assessment of its longevity and a review of the literature. J Plast Reconstr Aesthet Surg. 2012;65(3):328-32. DOI: http://dx.doi.org/10.1016/j.bjps.2011.09.024
8. Marey EJ. Physiologie Médicale de la Circulation du Sang. Paris: Adrien Delahaye; 1863.
9. Malbrain ML, Cheatham ML, Kirkpatrick A, Sugrue M, Parr M, De Waele J, et al. Results from the International Conference of Experts on Intra-abdominal Hypertension and Abdominal Compartment Syndrome. I. Definitions. Intensive Care Med. 2006,32(11):1722-32. PMID: 16967294 DOI: http://dx.doi.org/10.1007/s00134-006-0349-5
10. Malbrain M. Abdominal perfusion pressure as a prognostic marker in intra-abdominal hypertension. In: Vicent JL, eds. Year book of Intensive Care and Emergency Medicine. Berlin: Springer; 2002. p. 792-814.
11. Oneal RM, Mulka JP, Shapiro P, Hing D, Cavaliere C. Wide abdominal rectus plication abdominoplasty for the treatment of chronic intractable low back pain. Plast Reconstr Surg. 2011;127(1):225-31. PMID: 21200216 DOI: http://dx.doi.org/10.1097/PRS.0b013e3181fad2f7
12. Abramo AC, Casas SG, Oliveira VR, Marques A. H-Shaped, double contour plication in abdominoplasty. Aesthetic Plast Surg. 1999;23(4):260-6. DOI: http://dx.doi.org/10.1007/s002669900279
13. Martins FMT, Jardim JRB, Nery LE, de Morais VPP, dos Santos ML. Alteração da função pulmonar no pós-operatório de cirurgia abdominal alta. J Pneumol. 1980;6(4):169-72.
14. Daher JC, Reis CT. Alterações da dinâmica respiratória nas abdominoplastias. Rev Brasília Méd. 1976;12(1-2):121-4.
1. Sociedade Brasileira de Cirurgia Plástica, São Paulo, SP, Brazil
2. Hospital Daher Lago Sul, Brasília, DF, Brazil
3. Sociedade Brasileira de Anestesiologia, Rio de Janeiro, RJ, Brazil
4. Hospital São Francisco, Ceilândia, DF, Brazil
Institution: Hospital Daher Lago Sul, Brasília, DF, Brazil.
Corresponding author:
Daniel Augusto dos Santos Soares
CCSW 02 Lote 03, Residencial Unique Duplex apt. 105 - Sudoeste
Brasília, DF, Brazil Zip Code 70680-250
E-mail: daniel.soares@globo.com
Article received: November 2, 2016.
Article accepted: February 21, 2017.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket