



Ideas and Innovation - Year 2017 - Volume 32 -
Use of absorbable hemostatic gelatin sponge in postoperative care of the vascular pedicle of interpolated flaps
Uso do curativo hemostático de gelatina absorvível no cuidado pós-operatório do pedículo vascular dos retalhos interpolados
ABSTRACT
Interpolated flaps are among the most important and functional flaps in reconstructive plastic surgery, representing a safe option even in the most difficult cases. The pedicle of the interpolated flap requires a dressing to avoid bleeding and local contamination. This dressing often fails to prevent minor bleedings, which occurs within the first 24-48 hours. As a result, it needs to be continuously changed, from three to five times on average. The technique proposed in this study consists in a direct application of a GELFOAM® layer. This is subsequently wrapped with petroleum gauze to prevent bleeding of the open area in the pedicle flap, improving hemostasis and reducing the manipulation of the vascular pedicle.
Keywords: Surgical hemostasis; Surgical flaps; Postoperative bleeding; Dressings.
RESUMO
Os retalhos interpolados têm sido um dos mais importantes e funcionais retalhos no arsenal da cirurgia plástica reconstrutiva, tornando-se uma opção segura mesmo nos casos mais difíceis. O pedículo do retalho interpolado necessita de curativo para evitar sangramento e a contaminação local. Este curativo frequentemente falha na prevenção de pequenos sangramentos que ocorrem durante as primeiras 24-48 horas, forçando a troca recorrente do mesmo, em média de três a cinco trocas. A técnica proposta neste trabalho consiste na aplicação direta de uma camada de GELFOAM®, envolto por gaze petrolizada, para prevenção do sangramento da área cruenta do pedículo do retalho, acarretando melhor hemostasia e menos manipulação do pedículo vascular.
Palavras-chave: Hemostasia cirúrgica; Retalhos cirúrgicos; Hemorragia pós-operatória; Curativos.
Interpolated flaps have become one of the most important and useful flaps in reconstructive plastic surgery, as soon as they were described, providing a safe option, even in the most difficult cases. Frontal and nasolabial interpolated flaps for nasal reconstruction are the most common examples.
However, several indications and precautions should be followed to maintain the viability of interpolated flaps. These involve care in the manipulation of the dressing to avoid injuring the pedicle, besides risks of contamination and bleeding in the postoperative phase, which result from dressing changes. The surgeon is often urged to constantly change the dressing due to residual bleeding, which usually occurs 24 to 48 hours after the surgery.
Residual bleeding is a phenomenon associated with any surgical procedure, especially when there is an exposed area. Adequate or effective bleeding control should be ensured during and after the surgery, aiming to preserve hemostasis either by traditional methods, such as mechanical hemostasis by direct pressure at the bleeding site, hemostatic suture, thermal energy (electrocoagulation), or by topical hemostatic agents. The hemostatic agents are indicated to improve hemostasis, when conventional techniques are not feasible or the circumstances are not suitable.
In 1600, Ambroise Parè devised a procedure of vascular ligature considered a major breakthrough to contain and control bleeding. More recently, new technologies to control hemostasis have been developed. In 1924, electrocautery was performed for the first time, before the implementation of bipolar cautery1. Over the years, hemostatic techniques have been evolving. It is described in the literature that, around 1940, the use of thrombin was first introduced in surgery to control bleeding2.
Topic hemostatic agents have been used as an alternative treatment in cases of residual and postoperative bleeding. Two great groups or categories stand out, representing the entire family of topic agents. While physical agents promote hemostasis through passive (mechanical) substrates, biological or active agents (e.g. thrombin) function by modulating the coagulation process or cascade3.
Several studies have demonstrated the usefulness and effectiveness of hemostatic agents in reconstructive plastic surgery. The hemostatic gelatin sponge, which is proposed in this article, acts as a hemostatic barrier, due to its "buffering" and pro-coagulant effect, producing a matrix for platelet adhesion and aggregation1-3. It is a flexible and easy to handle product. When compared to other hemostatic agents available on the market, its cost is relatively low.
The option for a non-toxic biocompatible hemostatic product, which is well absorbed by the body without leaving residues, it is important to ensure less manipulation of the dressings. The ideal topical agent should present the following characteristics: high hemostatic action, minimal tissue reactivity, biodegradability, and biocompatibility.
OBJECTIVE
The pedicle flap requires dressing to avoid postoperative bleeding and contamination. This dressing needs to be sufficiently compressed, in order to prevent small bleeding, whereas allowing normal flow in the vascular pedicle. Unfortunately, the most common type of dressing used after surgeries fails to prevent usual bleeding from open surfaces, posteriorly to the vascular pedicle, especially during the first 24-48 hours.
This common complication usually leads to continuous dressing changes and increased rate of ischemia. Recommendations for the management of this area range from covering the pedicle with a petroleum gauze4, to partial skin grafting and the use of hemostatic dressings5,6. This work proposes a direct application of an absorbable gelatinous sponge (GELFOAM®), which is subsequently wrapped in petrolatum gauze, aiming to reduce the manipulation of the flap and ensure its viability.
METHODS
In this work, we present an easy approach to minimize the manipulation of pedicle flaps and residual bleeding.
In the Plastic Surgery Service of the São Lucas Hospital, at the Pontifical Catholic University of Rio Grande do Sul, we have incorporated the use of GELFOAM® as hemostatic agent in the postoperative care of the pedicle flap. This procedure implies a direct application and can be carried out soon after the surgery. We prefer the use of petrolatum gauze to reduce laceration and friction of the surrounding tissue if manipulation, change, or removal of the dressing is required.
A total of 20 cases have been evaluated. Most of them involved the use of pedicle flaps for nasal reconstruction. In 11 cases, the frontal flap was used, and in the remaining nine, the interpolated nasolabial flap was employed to treat and cover the nasal defect (Table 1).
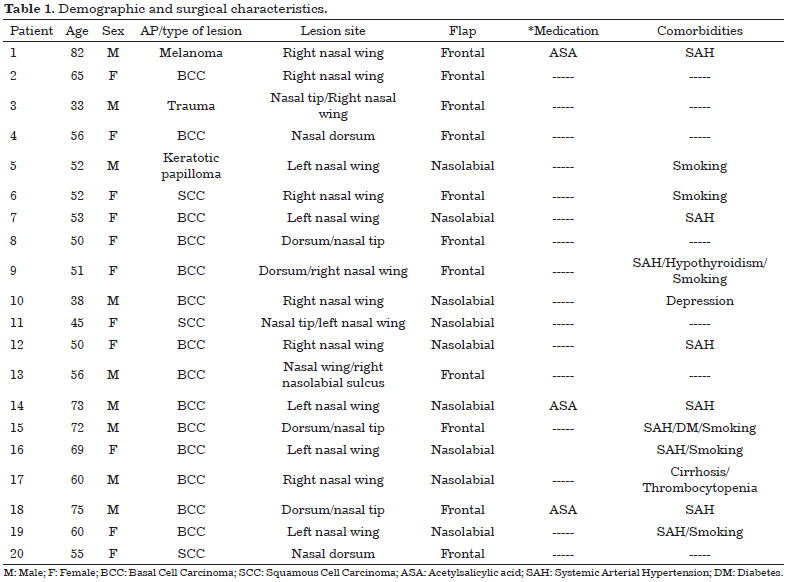
Three of the patients evaluated reported to use acetylsalicylic acid (ASA), which was suspended 7 days before the surgical procedure. Systemic arterial hypertension was the most common comorbidity found in the evaluated cases, reported in nine of the studied patients. There were no complications reported during or after the application of the thin layer of absorbable sponge.
Technique
Once the surgery is completed, the donor site is closed and the flap is sutured in the treated region. Careful hemostasis is performed on the pedicle, using as little electrocautery as possible. A thin absorbable gelatin sponge is applied on the open surface of the pedicle (Figure 1). This is subsequently wrapped in a layer of petroleum (ADAPTIC®) and dry gauze, and maintained for the next 72 hours, if no major bleeding occurs (Figure 2).

Figure 1. Hemostatic absorbable gelatin sponge GELFOAM®.

Figure 2. Thin absorbable sponge layer placed on an open area of the pedicle flap.
In the evaluated cases, the risk of residual bleeding in the postoperative period using this conduct was almost zero.
DISCUSSION
Topic hemostatic agents are key tools for controlling residual bleeding when cautery and hemostatic suture are not an option.
GELFOAM® absorbable sponge is a hemostatic device, insoluble in water, prepared using purified porcine gelatin, and capable to absorb blood up to 45 times its weight7. This absorptive capacity increases or decreases proportionally according to the gelatin size8. The mechanism implies a mechanical support8. Surface action devices applied directly on bleeding surfaces refrain the bleeding by forming an extracellular matrix 9.
Gelatin is hygroscopic, meaning it has the ability to absorb and retain water. This causes the wet (mesh) layer to stimulate coagulation10. According to the theory of Jenkins et al.11, the effect of coagulation may be due to the release of platelet thromboplastin, occurring when platelets are damaged, upon their contact with the GELFOAM ® interstitial wall.
Thromboplastin interacts with prothrombin and calcium and produces thrombin, this being the sequence of events that initiates the formation of clots. Researchers suggest that the physiological formation of thrombin in the sponge is sufficient to produce the clot, due to the action of blood fibrinogen11. Spongy physical properties cause clot's formation and provide the structural support for their generation9,12. Several investigators reported that GELFOAM® liquefies within a week and is completely absorbed within 4 to 6 weeks, without inducing excessive scar formation7,11,13-15. This fact was shown by Barnes in his experiment using absorbable gelatinous sponge in gynecological surgeries, though which there was no excessive scar tissue noticeable at the postoperative gynecological examination14.
CONCLUSION
The main advantage of using foam with absorbable gelatin solution in the immediate postoperative care of interpolated flap vascular pedicle is to prevent residual bleeding. This kind of dressing became a routine protocol in this Service for immediate bleeding control, improving hemostasis and causing less manipulation of the pedicle, which consequently results in a lower risk of flap ischemia. This procedure has led to benefits such as decrease in morbidity and in hospitalization time.
Our experience has shown a significant decrease in dressing changes, from three to five times to one or none in the first 24-48 hours, due to reduced bleeding, without compromising the vascular pedicle.
This study encourages the authors to carry out a systematic analysis of the results using the methodology described, which will be presented in subsequent publication.
COLLABORATIONS
ARM Analysis and/or interpretation of data, statistical analyses, completion of surgeries and/or experiments, writing the manuscript.
BQS Analysis and/or interpretation of data, statistical analyses, completion of surgeries and/or experiments, writing the manuscript.
LER Analysis and/or interpretation of data, statistical analyses, completion of surgeries and/or experiments, writing the manuscript.
LDPS Analysis and/or interpretation of data, statistical analyses, completion of surgeries and/or experiments, writing the manuscript.
MPO Conception and design of the study, completion of surgeries and/or experiments, Final approval of the manuscript.
CU Final approval of the manuscript.
REFERENCES
1. Emilia M, Luca S, Francesca B, Luca B, Paolo S, Giuseppe F, et al. Topical hemostatic agents in surgical practice. Transfus Apher Sci. 2011;45(3):305-11. PMID: 22040778 DOI: http://dx.doi.org/10.1016/j.transci.2011.10.013
2. Lew WK, Weaver FA. Clinical use of topical thrombin as a surgical hemostat. Biologics. 2008;2(4):593-9.
3. de Carvalho MV, Marchi E, Pantoroto M, Rossini M, da Silva DM, Teodoro LF, et al. Topical haemostatic agents and tissue adhesives. Rev Col Bras Cir. 2013;40(1):66-71.
4. Boyd CM, Baker SR, Fader DJ, Wang TS, Johnson TM. The forehead flap for nasal reconstruction. Arch Dermatol. 2000;136(11):1365-70. PMID: 11074699 DOI: http://dx.doi.org/10.1001/archderm.136.11.1365
5. Burget GC, Menick FJ. Aesthetic Reconstruction of the Nose. St. Louis: Mosby; 1994.
6. Christenson LJ, Otley CC, Roenigk RK. Oxidized regenerated cellulose gauze for hemostasis of a two-stage interpolation flap pedicle. Dermatol Surg. 2004;30(12 Pt 2):1593-4. DOI: http://dx.doi.org/10.1097/00042728-200412020-00026
7. Council on Pharmacy and Chemistry: New and Nonofficial Remedies - Absorbable Gelatin Sponge. JAMA. 1947;135(14):921. DOI: http://dx.doi.org/10.1001/jama.1947.02890140041011
8. Goodman LS, Gilman A. Surface-acting drugs, in The Pharmacologic Basis of Therapeutics. 6th ed. New York: MacMillan Publishing; 1980. 955 p.
9. Guralnick WC, Berg L. Gelfoam in oral surgery; a report of 250 cases. Oral Surg Oral Med Oral Pathol. 1948;1(7):632-9. DOI: http://dx.doi.org/10.1016/0030-4220(48)90337-5
10. Palm MD, Altman SJ. Topical Hemostatic Agents: a review. Dermatol Surg. 2008;34(4):431-45.
11. Jenkins HP, Senz EH, Owen H, Jampolis RW. Present status of gelatin sponge for control of hemorrhage. With Experimental Data on Its Use for Wounds of the Great Vessels and the Heart. JAMA. 1946;132(11):614-9.
12. Jenkins HP, Janda R, Clarke J. Clinical and experimental observations on the use of gelatin sponge or foam. Surgery. 1946;20(1):124-32. PMID: 20992243
13. Treves N. Prophylaxis of postmammectomy lymphedema by the use of gelfoam laminated rolls; a preliminary report, with a review of the theories on the etiology of elephantiasis chirurgica and a summary of previous operations for its control. Cancer. 1952;5(1):73-84. DOI: http://dx.doi.org/10.1002/1097-0142(195201)5:1<73::AID-CNCR2820050110>3.0.CO;2-2
14. Barnes AC. The use of gelatin foam sponges in obstetrics and gynecology. Am J Obstet Gynecol. 1947;54(1):105-7. DOI: http://dx.doi.org/10.1016/S0002-9378(16)39476-5
15. Rarig HR. Successful use of gelatin foam sponge in surgical restoration of fertility. Am J Obstet Gynecol. 1963;86:136. DOI: http://dx.doi.org/10.1016/0002-9378(63)90086-3
1. Hospital São Lucas da Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, RS, Brazil
2. Sociedade Brasileira de Cirurgia Plástica, São Paulo, SP, Brazil
Institution: Hospital São Lucas da Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, RS, Brazil.
Corresponding author:
Alan Rodriguez Muñiz
Av. Ipiranga, 6690, sala 220 - Jardim Botânico
Porto Alegre , RS, Brazil Zip Code 90610-000
E-mail: alan-rodriguez@outlook.com
Article received: October 28, 2014.
Article accepted: February 21, 2017.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket