



Special Article - Year 2016 - Volume 31 -
Nasal morphology - harmony and proportion applied to rhinoplasty
Morfologia nasal - harmonia e proporção aplicadas à rinoplastia
ABSTRACT
The study of nasal morphology is of fundamental importance for a better understanding and planning of rhinoplasty. The objective of this study is to analyze the basic shape of the nose seen as an isolated structure, and especially in equilibrium with the patient's face. The existing patterns to do so are quite subjective, since the concept of beauty depends on several factors. The classic proportion measurements assist the surgeon with the conception and aesthetic view. When combined with an understanding of the anatomy and surgical technique they determine the final outcome of rhinoplasty. Thus, the concept of "optimal" nose must be applied on an individual basis, respecting classical anthropometry patterns, gender, ethnic-racial, cultural and psychosocial factors. Morphology is not limited only to the static aspect of the nose, but is directly related to personal dynamics, mimicry and personality of the patient.
Keywords: Nose; Rhinoplasty; Nasal cartilages.
RESUMO
O estudo da morfologia nasal é de fundamental importância para um melhor entendimento e planificação das rinoplastias. O objetivo deste trabalho é analisar a forma básica do nariz visto como estrutura isolada, e principalmente em equilíbrio com a face do paciente. Os padrões determinados são bastante subjetivos, pois o conceito de beleza depende de vários fatores. As medidas clássicas de proporção auxiliam na concepção e visão estética do cirurgião. E quando associadas ao conhecimento da anatomia e técnica cirúrgica irão determinar o resultado final da rinoplastia. Logo, o conceito do nariz "ideal" deve ser aplicado para cada um, respeitando os padrões clássicos da antropometria, o sexo, grupo étnico-racial, fatores culturais e psicossociais. A morfologia não se restringe apenas ao aspecto estático do nariz, mas relaciona-se diretamente com a dinâmica pessoal, a mímica e a personalidade.
Palavras-chave: Nariz; Rinoplastia; Cartilagens nasais.
The study of human proportion was quite developed in Greek civilization. Aristotle in the fourth century BC already highlighted the importance of proportion applied to aesthetics. In the era of Hellenistic architecture, the human body was considered the perfect example of symmetry and harmony, being used as a measure to build temples1.
Long before that, the Egyptians used the middle finger as a basic measurement unit. Total body length amounted to nineteen fingers and the nose was the same size as the finger2. This justifies the representation of figures in profile with a typically enlarged nose and straight dorsum.
Later, according to the indication of some anatomists, the nose was used as a unit, where body length was equivalent to thirty noses1. It is also observed that there exists a proportion relationship between thumb length and nose, as well as hand and face2.
For the initial study of human figure, some classic works were examples of perfection, such as Demosthenes mask, Antinuous head, the marathoner kid and some Roman emperors, all of them emphasizing masculinity with a similar nasal pattern (slight hump on the dorsum, elevated Nasion and little nasal projection). Aphrodite images are examples of feminine beauty, with a small nose, straight dorsum and obtuse nasolabial angle1,3.
The Greco-Roman beauty pattern prevailed until the Renaissance, when Leonardo da Vinci determined important body and facial proportion measures. In front view, the face was divided into four segments, where the nose was equivalent to ¼ of the total. In profile, the craniofacial complex was represented by a square, defined anteriorly by the vertical plane of the face3-5 (Figure 1).
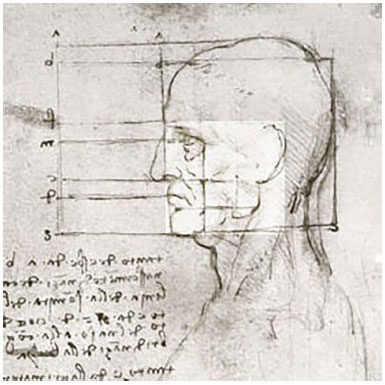
Figure 1. Proportions of the human head. Study by Leonardo da Vinci showing a square limited anteriorly by the vertical plane of the face, posteriorly by the insertion of the ear, inferiorly by the mandible and superiorly by the eyebrow. (Leonardo da Vinci. The proportions of the head, 1490).
In the early twentieth century, Ghyka used face proportion programs, emphasizing the classical patterns in well determined lines1 (Figure 2). These measures were initially used in nasal reconstruction surgeries after trauma with amputation.

Figure 2. A: Harmonic analysis of ideal proportions; B: Diagram of the proportions of the face, shown in A (Matila Ghyka. The Geometry of Art and Life, 1946).
In 1931, Jacques Joseph used proportional measures in cosmetic surgery, starting with rhinoplasty using the endonasal access. He divided the nose into three zones (Joseph zones). The upper third consists of the bony part of the nasal dorsum; the mid third formed by triangular cartilages or upper lateral side; and the lower third, which represents the moving part of the nose, called lobe by some authors. For others, the lobe is only the nasal tip5 (Figure 3).

Figure 3. Joseph Zones. 1) Bony part; 2) Mid 1/3 formed by triangular cartilages; 3) Lower 1/3 or lobe.
More recently, several authors have carried out anthropometric and profileplasty studies emphasizing the nose, among them Broadbent, Gonzalez-Ulloa, Farkas and Brahman Guyuron6.
OBJECTIVE
The objective of this study is to conceptualize the shape of the nose as an isolated structure and in equilibrium with the face to determine the harmony and proportion of the nose alone and its relationship with the craniofacial complex. This requires an artistic and aesthetic perception. This relationship should be compared to the classical patterns of proportion in cases of doubt.
We know that there is a strict relationship between the artist and the plastic surgeon. The surgeon, unlike the artist, works with predetermined and imperfect shapes, transformed by trauma or by time. The work of a surgeon results from his ability and practice and postoperative care, as opposed to the artist, who is free to create and whose results are immediate. The raw material of a surgeon is noble and irreplaceable. The similarity between both, artist and surgeon, is the pursuit of perfection associated with the conception of an ideal of beauty.
POINTS APPLIED IN ANTHROPOMETRY
Anthropometry applied to the nasal region requires the visualization of the patient in three projections: frontal; profile, including the whole craniofacial complex; and projection of the lower nose to study the nose pattern.
These points are as follows: The Trichion (TR) is the point where the hairline meets the midline of the forehead and varies a lot in men. The Glabella (G) is the area between the eyebrows, which separates the first part of the face from the second one, when the face is divided into three parts, (Figure 4).
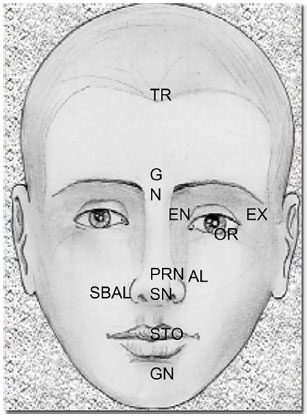
Figure 4. Points applied in anthropometry (frontal view): Trichion (TR), Glabella (G), Nasion (N), Inner canthus (IC), Outer Canthus (OC), Inferior orbital rim (OR), Pronasal (PRN), Alare (AL), Sublare (SBAL), Subnasal (SN), Stomion (STO), Gnathion (GN).
Nasion (N) is the most important point in the facial profile, is located in the deepest area of the frontonasal suture 4 to 6 mm below the glabella, and close to the projection of the upper eyelid7,8 (Figure 5). Pronasal (PRN) is the most important area of the nasal tip, in the midline of apex nasi. In cases of forked tip, there are two para-axial points. The subnasal (SN) point is also an important one and is located in columellalabial junction (Figure 6).

Figure 5. Nasion region (profile view).

Figure 6. Columella (profile view).
The Maxillo-frontal point (MF) is a lateral point that determines the thickness of the nasal root and is located at the junction of maxillo-frontal sutures. Stomion (STO) is the midpoint of the oral fissure. Gnathion (GN), menton or pogonion is the most prominent area of the mandible. The inner canthus (IC) and outer canthus (OC) are the innermost and outermost points of the eye, respectively. Alare (AL) is the most lateral part of the wings, which determines the width of the nasal lobule.
The Sublare (SBAL) is where the alar base disappears in the upper lip skin. The Alar curvature point (CA) varies a lot according to racial group8 (Figure 7). The relationship between these points determines distances and angles that represent the face proportion indices.

Figure 7. Landmarks used in nasal anthropometry (lower view): Pronasal (PRN), Alare (AL), Thickness of the wing (AL'-AL'), Length of the Columella (C'-SN), Subnasal (SN), Sublare (SBAL), Alar curvature point (AC).
NASAL PROPORTION INDICES
There is a total of sixteen nasal proportion indices. They determine the length, width, slope and angle of the nose. On the vertical axis we have the nose length (N-SN) and Dorsal Length (N-PRN). On the horizontal axis, we have the nasal width (AL-AL), alar length (AC-PRN), alar thickness (AL-AL), nasal root width (MF-MF), length of the nasal root slope (EN-M), columella thickness (SN-SN), width of the nose floor (SBAL-SN). In the bottom view we have the nasal root depth (EN-M), tip protrusion (SN-PRN) columella length (C-SN).
The main nasal inclinations are the dorsum (DS) and columella (CS). Three angles are used: nasofrontal (a) nasolabial (b) and nasal tip angle (g). The latter is known as Joseph angle8. In practice, these angles are the most used reference angles by surgeons (Figure 8).

Figure 8. Profile angles: Nasofrontal Angle (a), Nasolabial Angle (b) and Nasal tip angle (g). Inclinations: Dorsum (BI) and Columella (CI).
The Frankfurt Plane (F) is a key reference for the study of profileplasty, and is used to determine the nasal projection. It is created by the midline of two well-defined points. From the most prominent part of the tragus, Tragion (T), we draw a line toward the inferior orbital rim (OR) which may be marked externally, in the midline of the lower eyelid with the face (Figure 9).

Figure 9. Frankfurt plane: line traced between the Tragion (T) and the inferior orbital rim (OR).
This line forms the Frankfurt plane and the line perpendicular to this plane, which crosses the Nasion is the vertical axis of the face, the Facial Line8. Other authors determine the vertical axis by marking a line connecting the glabella to the pogonion, the Vertical Plane4. The nasofacial angle is formed by the vertical axis of the face and the line that follows the nasal dorsum. In men it is in average 36º, and slightly lower in women, about 34º. This angle determines the nasal projection.
There are 6 Neoclassical Canons for nasal measurements: Face Profile divided into 3 parts (forehead, nose length and lower face); Nasoaural (ear insertion at the same height as the nose); Orbitonasal, Nasofacial and Naso-oral (which determines the width of the nose) pattern; Naso-aural slope (parallel relationship between the nasal dorsum and the major axis of the ear) (Figure 10).

Figure 10. Neoclassic patterns: 1. Face profile in 1/3 (A, B e C); 2. Nasoaural pattern; 3. Orbitonasal pattern; 4. Nasofacial pattern; 5. Naso-oral pattern; 6. Nasoaural inclination.
The Nasal Index is a calculation of the thickness divided by the length, times one hundred (N.I. = thickness/length x100). This index classified the nose into 3 types: Leptorrhine, less than 60%; Mesorrhine between 60 and 80% and Platyrrhine, greater than 80% (Figure 11).
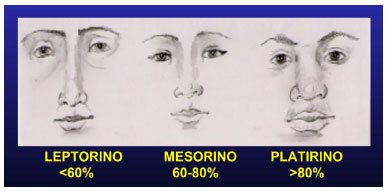
Figure 11. Nasal index: 1. Leptorrhine; 2. Mesorrhine; 3. Platyrrhine.
EXTERNAL NOSE ANATOMY
The nose is divided into two regions: the cephalic and caudal part. The cephalic part is fixed and is formed by the bone pyramid and the top of the triangular cartilage. The caudal part is mobile and is also called lobe (Figure 12). There is a controversy on whether the term lobe only represents the nasal tip or the whole mobile part.

Figure 12. External anatomy of the nose; cephalic and caudal part.
The root, in the most cranial portion, is limited by the extension of the midline of the eyebrow line and inferiorly by the lower eyelid rhyme. It may also be the region between the upper and the lower orbital rim. In the deepest part we have the Nasion, which is located at the level of the upper eyelid crease. The Nasion may be high, as in Greek type noses, or low as in the negroid nose (Figure 13).

Figure 13. External anatomy of the nasal root and its measurements. Nasal root width (MF-MF).
The nasal dorsum, from a surgical point of view is better conceptualized as the osteo-cartilaginous valve, located between the root and the nasal lobule. The most important measurements are the thickness and inclination of the dorsum (Figure 14). Parallel dorsal lines should be the continuation of the philtral ridges.

Figure 14. External anatomy of the dorsum and its dimension. The dorsum is 8 to 10 mm thick in men and 6 to 8 mm thick in women. The inclination of the dorsum is measured by the Nasofacial angle (about 36º in men and 34º in women).
The dorsum is 8 to 10 mm thick in men, with a slightly convex or straight profile and is 6 to 8 mm thick in women, with a slightly concave profile. Inclination of the dorsum is measured by the nasofacial angle (about 36o. in men and 34o. in women), which is the most important nasal angle. We should also observe deviation from the midline, with changes in the whole axis, irregularities and size of the hump (bone and cartilage)
The nasal lobule consists in the tip (apex nasi), alas, columella and the septum is the internal support structure. The tip is formed by the contact of alar cartilages. Sheen determined four characteristic points at the tip: two bright spots (light reflex points), the supra-tip region and the columella-lobular junction, forming two isosceles triangles9 (Figure 15).

Figure 15. Nasal tip Isosceles triangles (Sheen); Two light points in the supra-tip region and at the columella-lobular junction.
The projection of the nasal tip may be measured by the distance between the pronasal (PRN) and subnasal (SN) regions, or between the NRP and the alar insertion region10 (Figure 16). There is also an angle that represents the separation between the medial crura, divergence angle; and columella-tip angle, which is the rotation angle. This angle is greater than 50 degrees and determines the upturned tip and when it is less than 30 degrees we have the falling nasal tip11.

Figure 16. Methods for tip protrusion measurement: Tip Protrusion (SN-PRN) and Alar length (AC-PRN).
The nasal tip should be investigated as to its thickness, position, rotation, symmetry and projection. The thickness is determined by skin type and form of alar cartilages at the domus. In cases of hyperprojection, there are intrinsic and extrinsic factors that increase the tip. A heavy, blobby, or bulbous nose results from an increase of the columellar-alar angle of the alar cartilages, and has no relationship with the cephalometric nasal index. Moreover, a bulbous nose usually has excess fatty tissue present at the tip of the nose10. Extrinsic factors are advanced jaw, increased septum and nasal spine. Intrinsic factors include increased alar cartilage at the medial crus and elongated columella.
When the tip is flat there is a hypodevelopment or decrease of these elements. There are several forms of atypical tip: forked tip, boxer tip, in parentheses, ball-point, boxy and globous tip10. In case of a globous tip (fatty or sebaceous), there is an increase in skin thickness and sebaceous glands, which impairs the final aesthetic result of the surgery11.
The columella is extended from the tip to the lip, separating the nostrils medially. In profile view, it corresponds to approximately 60% of the lobe. Aesthetically speaking, the columella should be a little more projected than the alas. Its inclination is related to the nasolabial angle, also called columellar-labial or septo-labial angle.
This angle may be modified by the action of a dermocartilaginous ligament located along the dorsum, going down between the domus toward columella. With the action of mimic muscles there is a depression of the nasal tip. This tip depression can be treated sectioning this ligament12.
The nasal ala is a lateral extension of the lobe, and consists basically in the alar cartilages. The measurement between the two alas of the nose is nasal thickness, which according to the classical anthropometric patterns, corresponds to one fifth of the face in the front view (Figure 17).

Figure 17. Anterior vision of the face, divided into 5 equal parts. The nose in the central fifth.
ETHNIC-RACIAL VARIATIONS
Harmony and symmetry are universal elements of beauty6. In the study of nasal morphology nasofacial balance and proportions are important elements. Therefore, in ethnic groups with broad faces, and increased intercantal and bimaxillary protrusion distance, we cannot change the nose and make it thin and not proportional with the face. The objective of rhinoplasty in these cases is to provide a better definition of the elements, respecting ethnic and racial patterns.
Anatomical variations are determined by five elements: skin type, fibrofatty layer, alar cartilage, base of the nasal ala and pyramid. These variations are particular to each racial group. In black patients with thicker skin at the tip, with lower elasticity and an increase in subcutaneous tissue above the alas, determining a lower definition of this area, giving the appearance of bulbous nose12,13.
The alar cartilage is thin and undeveloped in blacks, however, in a study in fifteen cadavers, Daniel observed the opposite7. The angle of divergence between the medial and medial and lateral crus is obtuse, often greater than 90 degrees, and the space is filled by fatty and fibrous tissue. The nasal spine is more prominent in Caucasians. Deformities of the alar base may be divided by the interalar distance and alar curvature.
Typically, interalar distance corresponds to the medial canthal line and in blacks it is greatly increased. The curvature of the lateral alar rim is characterized by lateral extension greater than 2 mm from its implantation in the face. In Negroid nose this distance is reduced or absent. The nasal pyramid and dorsum are more projected in Caucasians.
Negroid and oriental noses have extended bone pyramid, and depressed dorsum14. The frontonasal angle also varies according to racial group, and is deeper in blacks, increasing the appearance of a flat nose (platyrrhine). In Caucasians, the frontonasal angle is higher, increasing the projection of the nose, usually associated with a tip hyperprojection (leptorrhine). In Orientals it is a mid-term between the Negroid and Caucasian nose (mesorrhine) 6.
Cephalometric indices are also important when an extensive reconstruction of the face or nose is necessary, whether they are due to congenital or post-traumatic defects. A database with the main measurements was collected from different ethnic groups. The normal range was established for each resulting database, providing valuable information on the main facial characteristics15,16.
In Brazil there is a large ethnic-racial complex, which includes mainly Caucasians, Native Indians and African blacks. Early in the century, miscegenation increased as a result of the immigration of several groups (Italians, Germans and Japanese). The dominant character of blacks determined the development of some features of the so-called bulbo-negroid nose.
However we cannot conceptualize a single nose type in Brazil. What we find are several elements of different racial groups determining a large number of shapes and patterns, which requires a more specific work in each region17.
A study by Farkas et al.7, evaluating 200 white patients from four different sub-groups: Anglo-Saxon (n = 91), German (n = 26), Latin (n = 25), Slavic (n = 27) and others (n = 31) demonstrated that the most significant differences occurred in the mobile part of the nose (lobe). As it occurs with the projection of the tip, larger in German groups and smaller in Latin groups, the pattern of the angle of the nasal tip or inclination of the columella, which vary among these groups. The largest tip angle (76.5 degrees) was found in the German group and the lowest in Latin (70 degrees).
TYPES OF NOSTRIL
The nose pattern is directly related to the length of the columella, tip projection and inter-alar distance, varying significantly according to the racial group. The type of nostril is classified as an angle formed between a line that crosses the nose base and the major axis of the nostril (Figure 18).

Figure 18. Determining the nose angle (line that crosses the nasal base and the major axis in the nostril).
They are classified into seven types (Figure 19). During growth there is a change in this angle until the nose reaches its final size. In the newborn the nostril is round, i.e. 0 degrees; and according to the racial group it rises to 60º in children, and may reach 90º in adults.

Figure 19. Farkas classification for nose types: I (70 a 90º); II (55 to 69º); III (40 to 54º); IV (nostril without the major axis); V, VI e VII (negroid types).
Type I ranges between 70 and 90º and is characteristic of the Anglo-Saxon nose. In type II (55 to 69º) characteristic of European groups, where the base is slightly more curved than in nostril type I. In type III (40 to 54º) the base is wider and full, and is typical in southern Europe, Asia and Latin America.
Type IV is a round nostril that does not have a major axis, found in a few non-Caucasian groups and in some Asian groups. Type V (25-39º) and VI (10-24º) is more frequent in Negroid noses, where the base is quite wide. The last type, Type VII has a negative axis (-50 to -20 º), is unusual even in blacks and is associated with a wide columella, with tip projection equal to type VI.
The change in nasal shape should only be determined after determining the standard of measurements and ethnic-racial types. When even within the normal range, the nose has an unpleasant aspect, we can classify it into Correction of Disharmony. On the other hand, when there is actually a rupture of facial harmony with the measurements that are outside the normal range, we classify it Correction of Disproportion7.
Harmony means an optimal proportion relationship. And proportion is the relationship of measurements that as constant and in parallel with other structures. These concepts are fully applied for the nose and parallelism is applied with the craniofacial complex. There are different measurements and proportions among nose structures.
However we cannot standardize a basic type, since the face to be taken as a reference. And in turn, the face is presented in various forms, influenced mainly by ethnic-racial character. Therefore, based on studies conducted since the Renaissance by artists and anatomists until the present time by orthodontists and plastic surgeons, we can determine a sum of measurements, which when within the normal range, may represent an ideal of beauty.
In the 50's, an Italian orthodontist declared that beauty is not an abstraction created from the artist's imagination, but a concrete fact, as long as based on measurable characteristics demonstrated in a biometric correlation and somatic characters4.
Some authors recommend the use of cephalometric analysis of soft tissues, together with the application of mold on the photograph of the patient, so that an accurate rhinoplasty is performed7. However, in the planning of conventional rhinoplasty, most surgeons use only their own concept of aesthetics and their knowledge of classical measurement standards, without making a detailed study for each case.
"Predictive" rhinoplasty based on a quantitative analysis may provide accurate data for the removal of the nasal dorsum or alar cartilages9. It is comparable to the use of computer graphics in the idealization of the final result. This may be an ambitious proposal and is often disappointing for the patient after surgery, since the actual results, regardless of the surgeon's experience, can never be compared to a computerized simulation.
Likewise, previous quantification of what will be resected or modified may be affected by many factors, both during surgery and in the postoperative period. For example, fibrosis resulting from scarring may change the definition of structures, with an impact on the final shape of the nose. However, these changes do not invalidate the proposed method.
Studies evidencing racial characteristics8-12 report the characteristic types for each group. However, the patient's opinion is of fundamental importance. Complaints, in some cases, do not reflect the true existing change. It is for the surgeon to clarify and inform about possible changes, respecting patients' will.
Therefore, the planning of rhinoplasty should be made only after a complete understanding of what the patient wishes to change his or her nose. The psychological profile must also be respected, and in some cases, it is better to avoided radical changes in the shape of the nose.
CONCLUSION
In conclusion, nasal morphology is an essential part of balance, harmony and proportion of the face. Several parameters are used as cephalometric references that will determine corrections in nose disharmony and disproportion. It is essential to be aware of all of this to perform a rhinoplasty. However, their use is only required in cases of extreme changes.
Finally, we highlight there is no single aesthetic pattern for the nose, there must be a balance and adjustment according to different faces and individuals. Rhinoplasty may be the only cosmetic surgery offering an actual benefit of "beauty" to the patient.
COLLABORATIONS
IRF Study conception and design.
REFERENCES
1. Seghers MJ, Longacre JJ, Destefano GA. The Golden Proportion and Beauty. Plast Reconstr Surg. 1964;34(4):382-6.
2. Bellanger C. Desenho Artístico: Contendo a nomenclatura anatômica do corpo humano adaptado para as condições brasileiras por João Medeiros. RJ, BNG/Brasil Art; 1978.
3. Broabent TR, Mathews VL. Artistic relationships in surface anatomy of the face: application to reconstructive surgery. Plast Reconstr Surg (1946). 1957;20(1):1-17.
4. Farkas LG, Sohm P, Kolar JC, Katic MJ, Munro IR. Inclinations of the facial profile: art versus reality. Plast Reconstr Surg. 1985;75(4):509-19.
5. McCarthy JG, ed. Plastic Surgery. Vol. 3. Philadelphia: Saunders; 1990. p. 1785-804.
6. Daniel RK, ed. Aesthetic Plastic Surgery: Rhinoplasty. Boston: Little, Brown and Co; 1993.
7. Farkas LG, Kolar JC, Munro IR. Geography of the nose: a morphometric study. Aesthetic Plast Surg. 1986;10(4):191-223.
8. Guyuron B. Precision rhinoplasty. Part I: The role of life-size photographs and soft-tissue cephalometric analysis. Plast Reconstr Surg. 1988;81:489-99.
9. Sheen JH. Aesthetic Rhinoplasty. Vol. 1. St. Louis: CV Mosby; 1987. p. 83-93.
10. Farina R, Cury E, Ackel IA. The prominent nasal tip. Aesthetic Plast Surg. 1984;8(3):141-4.
11. González-Ulloa M. The fat nose. Aesthetic Plast Surg. 1984;8(3):135-40.
12. Pitanguy I. Surgical importance of a dermocartilaginous ligament in bulbous noses. Plast Reconstr Surg. 1965;36:247-53.
13. Pitanguy I. Narizes Bulbo-Negróides: experiência e contribuições pessoais ao seu tratamento. Rev Bras Cir. 1971;61(11-12):201-11.
14. de Avelar JM. Personal contribution for the surgical treatment of negroid noses. Aesthetic Plast Surg. 1976;1(1):81-8.
15. Beheri GE. Rhinoplasty in Egyptians. Aesthetic Plast Surg. 1984;8(3):145-50.
16. Farkas LG, Katic MJ, Forrest CR, Alt KW, Bagic I, Baltadjiev G, et al. International anthropometric study of facial morphology in various ethnic groups/races. J Craniofac Surg. 2005;16(4):615-46.
17. Junqueira Júnior AA, Magri LV, Melchior MO, Da Silva AMR, Rodrigues da Silva AMB, Rodrigues da Silva MAM. Facial anthropometric analysis of a healthy group of young Brazilian adults by means of stereophotogrammetry technique. Rev Odontol UNESP. 2016;45(3):139-45.
1. Sociedade Brasileira de Cirurgia Plástica, São Paulo, SP, Brazil
2. Harmony Medical Center, Fortaleza, CE, Brazil
Institution: Harmony Medical Center, Fortaleza, CE, Brazil.
Corresponding author:
Isaac Rocha Furtado
Avenida Dom Luis, 1233, sala 606 - Meireles
Fortaleza, CE, Brazil Zip Code 60160-230
E-mail: dr.isaacfurtado@gmail.com
Article received: April 27, 2016.
Article accepted: August 6, 2016.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket