



Original Article - Year 2016 - Volume 31 -
Clinical classification of brow ptosis
Classificação clínica de ptose da cauda do supercílio
ABSTRACT
INTRODUCTION: The study of the eyebrow is a great challenge for plastic surgery because of its complex relationship with facial structures. The present study aims to describe a clinical classification of brow ptosis.
METHODS: A cross-sectional study with patients of both sexes and ages ranging from 18 to 100 years, subdivided into 3 groups according to age. Group 1: 18 to 30 years of age, Group 2: 31 to 60 years of age, and Group 3: 61 to 100 years of age. Three measurements were taken on each side by different examiners blinded to each other's results.
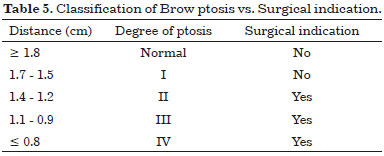
RESULTS: A total of 90 patients, with ages ranging from 18 to 94, including 39 (43.3%) men and 51 (56.7%) women, were studied. Group 1, with a mean age of 26.7 years was considered normal, with mean brow ptosis of 2.14 cm. In Group 2, with a mean age of 44.2 years, the mean brow measurement was 1.9 cm. In Group 3, the mean age was 72.6 years and the mean brow measurement was 1.27 cm. The table outlining the brow ptosis classification assigns a degree of ptosis to each interval, ranging from I to IV. Each degree was correlated with a numerical range in which > 1.8 cm is normal, 1.7-1.5 cm corresponds to degree I ptosis, 1.4-1.2 cm to degree II ptosis, 1.1-0.9 cm to degree III ptosis, and < 0.8 cm to degree IV ptosis. Surgery was indicated for degrees II, III, and IV.
CONCLUSION: The objective measurement of brow tail position enabled classification of the degree of ptosis and guides surgical decision-making.
Keywords: Classification; Eyebrows; Lift; Anthropometry.
RESUMO
INTRODUÇÃO: O estudo do supercílio se emoldura como um grande desafio para a cirurgia plástica por sua complexa relação com as estruturas faciais. O objetivo é descrever uma classificação clínica de ptose da cauda do supercílio.
MÉTODOS: Estudo transversal, com pacientes de ambos os sexos, com idade de 18 a 100 anos, subdivididos em três grupos segundo a faixa etária. Grupo 1: 18 a 30 anos, Grupo 2: 31 a 60 anos e Grupo 3: 61 a 100 anos. Realizaram-se três medidas de cada lado por examinadores distintos, sem que cada um soubesse o valor da aferição dos demais.
RESULTADOS: Total de 90 pacientes, com idades variando entre 18 e 94 anos, sendo 39 (43,3%) do sexo masculino e 51 (56,7%)do sexo feminino. As medidas do Grupo 1, considerado como normal, com média de idade de 26,7 anos, e com média de 2,14 cm em relação a medidas da ptose da cauda do supercílio. Já no Grupo 2, média da faixa etária foi de 44,2 anos e a média foi de 1,9 cm. No Grupo 3, média de idade de 72,6 anos com média de 1,27 cm. A tabela com a Classificação da Ptose da Cauda do Supercílio, em que se atribuiu a cada intervalo um grau de ptose, variando de grau I ao grau IV. Cada grau foi correlacionado com um intervalo numérico em que: > 1,8 cm representa a normalidade; 1,7-1,5 cm o grau I de ptose; 1,4-1,2 cm o grau II de ptose;1,1-0,9 cm o grau III de ptose e < 0,8 cm o grau IV de ptose. Em referência à indicação cirúrgica, essa teve sua indicação nos graus II, III e IV.
CONCLUSÃO: A medida objetiva da posição da cauda do supercílio possibilitou classificação do grau de ptose e orientação quanto à necessidade de intervenção cirúrgica.
Palavras-chave: Classificação; Sobrancelhas; Rejuvenescimento; Antropometria.
Through the centuries, the concept of beauty has been a goal and a challenge for artistic geniuses. Scholars and artists have sought to represent the classical ideal of human beauty since ancient times. For example, the work by Marcus Vitruvius Pollio, a renowned Roman architect, detailed the measurements and proportions of the perfect human body, which he entitled the "golden ratio"1.
Such work, which only expressed the proportions of the human body as numbers, was portrayed by the Renaissance genius artist Leonardo Da Vinci, who immortalized the "Human Being" in his works. In his "Vitruvian Man," Leonardo Da Vinci materializes the numbers on the human body, showing the proportions of beauty. Another key expression of Da Vinci's genius is "La Gioconda," which shows classic beauty in the proportions of the face, and especially in the expression of the eyes.
The archetype of human beauty is mainly expressed in the face, with all its nuances and expressions of feeling, and in the body's aging stages, which show the significance of facial expressions and the proportions of its constituents in social relationships and human health.
Scientifically, aging is depicted by the repositioning of both the soft tissue constituents and bone structure of the face, as defined in studies conducted by Shaw et al.2 and Matros et al.3. Such studies were performed using measurements obtained using computed tomography with 3-dimensional reconstruction and photographic records, and show changes in facial bone structure and volume, as well as repositioning of the eyebrows in their central-medial and medial parts.
In this context, the eyebrow, especially the tail, is the body part with the greatest ability to depict the feelings of individuals and the aging process, through eyebrow movements and positions, as was well characterized by the writer and artist Gordon C. Aymar: "the eyes are the place one looks for the most complete, reliable, and pertinent information about the subject. And the eyebrows can register, almost single-handedly, wonder, pity, fright, pain, cynicism, concentration, wistfulness, displeasure, and expectation, in infinite variations and combinations"4.
Based on the above, the study of the eyebrow is a great challenge for plastic surgery because one of the greatest goals of this medical specialty is to define classic beauty by adjusting the proportions of facial sections and repositioning structures to achieve a youthful and empathic expression.
A literature review of the main databases showed that many studies focus on assessment and brow lift5-12. However, no study has been published that aimed at classifying ptosis of this anatomical structure, thereby guiding treatment for adjustment of the proportions of facial beauty. Accordingly, this is the aim of the present study.
OBJECTIVE
To describe a clinical classification of brow ptosis.
METHODS
This cross-sectional, single-center study included a cohort of patients followed up in the Plastic Surgery outpatient clinic of São Paulo Hospital - School of Medicine of the Federal University of São Paulo (Universidade Federal de São Paulo - UNIFESP), in São Paulo (SP), SP. The study was conducted from March to August 2014. All patients were selected according to inclusion and exclusion criteria and were divided into groups according to age, totaling a sample of 90 patients.
All patients participating in the study signed an Informed Consent Form after being given an explanation of the procedures, risks, and possible complications.
All procedures were performed in compliance with the standards of the Research Ethics Committee of the School of Medicine of the Federal University of São Paulo (Universidade Federal de São Paulo - UNIFESP) and Resolution 196/96 of the National Health Council (Conselho Nacional de Saúde - CNS).
The following inclusion criteria were used: patients aged 18 to 100 years with no prior facial surgery or diagnosis of collagen disease (for example: cutis laxa, Ehlers-Danlos syndrome), and eyebrows without any treatment, including tattoos, regardless of sex.
The following exclusion criteria were used: patients refusing to participate in the study, patients with facial and/or ear malformation syndromes, patients with scars on the middle facial third caused by trauma, patients with peripheral or central facial paralysis, patients using botulinum toxin, and skin diseases that cause eyebrow alopecia.
All patients were subdivided into 3 groups according to age. Group 1: 18 to 30 years, Group 2: 31 to 60 years, and Group 3: 61 to 100 years. Each group had n = 30 patients and all were subjected to the same method of measurement.
Measurements were performed directly and objectively during facial physical examination, with patients standing upright and the eyes open, looking straight ahead, and with facial muscles in a maximally relaxed position. Three measurements were taken on each side by different examiners who were blinded to each other's results, totaling 9 measurements on each side. All data were recorded in a specific table for subsequent analysis, using a weighted average.
A digital caliper (0.01-mm accuracy; OTMT Machines, NY, USA) was used to measure the end-of-eyebrow point (EP) in relation to the Frankfurt plane (FP: Figure 1), defining a line (X) connecting this points at a 90º-angle to the Frankfurt plane (Figures 2A and 2B).

Figure 1. Demonstration of the end-of-eyebrow point (EP) and Frankfurt plane (FP).

Figure 2. A: Demonstration of the line (X) perpendicular to the Frankfurt plane - front view; B: Line (X) perpendicular to the Frankfurt plane - side view.
The Frankfurt plane is defined as the plane passing through the lowest points of the lower margin of the left and right orbits (orbitales) and the most lateral points of the roofs of the left and right ear canals (porions)13, and is a key anatomical reference easily defined by plastic surgeons in the facial examination.
The quantitative data resulting from the measurements were subjected to statistical analysis using Student's t test in each group, and intergroup comparison was performed using the Wilcoxon signed-rank test. After statistical analysis, all results were outlined in tables for improved visualization. A table with the classification of degrees of ptosis was constructed with the data, with surgical indication depending on clinical presentation.
RESULTS
A total of 90 patients with ages ranging from 18 to 94 years, including 39 (43.3%) men and 51 (56.7%) women, were recruited.
The statistical characterization of the groups and their internal relationships are outlined in Tables 1, 2, 3, and 4, which show the mean, mode, median, minimum, maximum, and standard deviation (SD) values of the variables: age (in years), mean measurements of the right eyebrow tail (RET) in centimeters, and mean measurements of the left eyebrow tail (LET) in centimeters, for each study group, as well as the sum of all values, as outlined in Table 4.




Three groups were formed, with the following representative values: mean age of 26.7 years in Group 1, 44.3 years in Group 2, and 72.6 years in Group 3. The standard deviation values for Group 1 (considered the normal standard) in relation to the RET and LET measurements are key data, which express the ranking of the values outlined in the Table of classification of the degree of brow ptosis.
The data analysis outlined in Table 4 shows a mean age for all groups of 47.8 years, a mean RET measurement of 1.78 cm, and a mean LET measurement of 1.79 cm, with a median of 1.8 cm, used to define the reference ranges. Therefore, the initial value considered normal was > 1.8 cm, thereby establishing the degrees of ptosis by subtracting 0.2 standard deviation (SD) from that value. Thus, the values were grouped into 4 degrees of ptosis.
Data collected from patients in Group 3 who complained of eyebrow hair loss were assessed for surgical indications. Table 3 shows a mean age of 72.6 years, with a mean of 1.2 cm for loss of eyebrow tail and a 1.4-cm median. This range defined the starting point for a surgical indication as it corresponds to a decrease by 0.2 standard deviation, and is fully contained in the group with clinical complaint of loss of the eyebrow tail.
Table 5, which outlines the classification proposed in the present study, was constructed following data analysis. It is noteworthy that all data were analyzed for their intragroup and intergroup differences, thus supporting the study conclusions. Statistical data are indicated below Table 5, and demonstrate their validity.
No significant differences in intragroup measurements were observed between RET and LET.
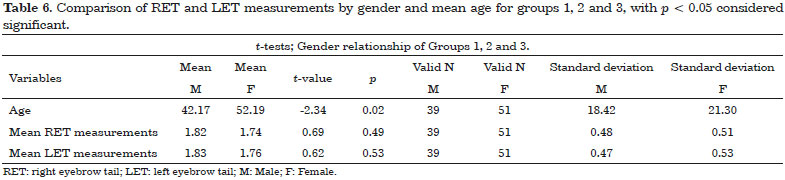
The comparison between sexes and mean ages and the mean RET and LET measurements showed no significant intragroup differences, and no p value < 0.05 was found.
The analysis of the overall data for the sum of mean ages, RET, and LET by gender showed significant differences in age, with an older mean age for women than that of men, consistent with the specific age structure of the country, wherein the prevalence of women increases with age because they have a higher life expectancy. This observation, which qualifies the study sample as representative of the Brazilian population, is outlined in Table 6.
Intergroup data analysis was performed using the Wilcoxon signed-rank test, assessing the relationship between the mean measurements of right (RET) and left (LET) eyebrow tail ptosis and mean ages. All measurements showed significant differences and therefore could be compared and used to construct the Table of classification of the degree of brow ptosis.
The only exception occurred in the comparison of the values of the LET in Group 1 and Group 2. This may be explained by the degree of accuracy of the instrument used, as the statistical analysis showed no difference on the left side. These data may be considered irrelevant to the overall analysis and the construction of the classification Table.
DISCUSSION
Through the centuries, the need for classification permeates the evolution of mankind. Since ancient times, humans have been using classification for their social organization. The oldest known system of classification was defined by Aristotle, who dichotomized living beings into animals and plants14.
In modern times, such need is increasingly relevant because the amount of new knowledge that emerges daily could not be used if not classified and organized. A literature search identified several articles proposing ways to measure eyebrow position5,6,12 and methods of assessment through standardized photographs15. However, no study introduced an objective method with defined anatomical points or proposes a clinical classification enabling plastic surgeons to evaluate their patients in medical consultation for surgical decision-making.
The present study established the Frankfurt plane as the basic measurement reference. This plane is easily characterized without requiring sophisticated devices, considering the need to perform a simple measurement based on points with little individual variation (bone structures). This characteristic permits the final measurement of the eyebrow tail in a perpendicular line to the Frankfurt plane, and is an ideal tool that is easily applied to the assessment of this area by the plastic surgeon.
The present study proposes to use measurements subdivided by age groups, with Group 1 (n = 30, 18 - 30 years of age) as the range of normality, and Group 2 (n = 30, 30 - 60 years of age) and Group 3 (n = 30, 61 - 100 years of age) as having higher degrees of ptosis; this approach is consistent with the data in the literature, which show maintenance of skin characteristics until 30 years of age, with sequential changes of increased collagen loss and dermal matrix breakdown until 60 years of age, followed by faster progression16,17, thus causing increased ptosis.
Hwang16 showed that the epidermal and dermal thickness of the palpebral and eyebrow area thins with age, with mean values of 884 µm at 30 years of age and 818 µm in patients older than 61 years, in a study of a Korean population. This explains and corroborates the values of brow ptosis found, as the thickness decreases after 30 years of age, and the gap between younger and older age groups widens after 61 years of age.
Data analysis showed that the measurements in Group 1, which is considered normal, with a mean age of 26.7 years, ranged from 1.6 cm to 2.7 cm, with a 2.14-cm mean, 2.2-cm median, and 2.2-cm mode of brow ptosis measurements. In Group 2, the mean age was 44.2 years and ptosis ranged from 1.2 cm to 2.5 cm, with a 1.9-cm mean, 1.98-cm median, and 2.1-cm mode; this showed a ptosis trend caused by changes from aging. Data analysis in Group 3 matched the histological findings of skin changes, with a mean age of 72.6 years and ptosis ranging from 0.5 cm to 1.93 cm, with a 1.27-cm mean, 1.4-cm median, and 1.2-cm mode.
No studies reporting measurements and data analysis using the aforementioned methods have been published in the literature, which precludes comparisons with other publications. Packiriswamy et al.6 performed a study in a population of 200 Malaysian and 200 South Indian subjects aged between 18 and 26 years to determine differences between the eyebrow positions in these populations.
The method used consisted of taking measurements with photographs, and quantified the loss of eyebrow tail using an oblique line between the lateral eye corner and the end of the eyebrow. Consequently, the authors found that no difference was present between the populations, with male mean measurements of 16.25 ± 2.39 mm in Malaysian and 16.09 ± 2.29 mm in South Indian men.
The authors found slightly higher values in the female population, with 17.15 ± 2.08 mm in Malaysian and 17.58 ± 2.5 mm in South Indian women. A caveat of the study was its method, which used photographs and computer-assisted measurements, without defining fixed anatomical references, and only performing one-dimensional measurements. Furthermore, the measurements taken to show brow ptosis were based on 2 variable points, which change with age - the eyebrow tail and lateral canthus of the orbital fossa - thereby causing measurement bias.
Matai et al.12 reported an angular measurement of brow ptosis in 261 patients, including 125 children aged between 4 and 6 years, and 136 adults older than 50 years, subdivided into groups aged 50-60, 61-70, and older than 70 years. All patients were recorded for 3 minutes in front view and the measurements were performed using software.
The authors reported no values, only finding a difference between the groups of children and adults. Such study defines very different age groups, even with children in the growth phase and without fully developed craniofacial structures. The front-view recording method and subsequent computer-assisted measurements precludes the actual measurement of the end-of-eyebrow point because the face is a 3-dimensional structure.
The inclusion criteria of that study were not well defined, with very heterogeneous groups leading to sample and comparison bias. Therefore, the need became apparent to establish another method of measurement to guide treatment based on classification.
In the present study, statistical analysis was performed using the aforementioned data, indicating an SD of 0.2. Therefore, the following ranges were established: > 1.8 cm, 1.7 - 1.5 cm, 1.4 - 1.2 cm, 1.1 - 0.9, cm and < 0.8 cm (Table 5), separated by the 0.2 SD. The present study noticeably aimed to introduce a clinical classification that could be used during a medical consultation to aid physicians in surgical decision-making and to identify the best postoperative eyebrow tail position.
Jones & Lo7 reported a 5-year follow-up of patients subjected to endoscopic brow lifts. They used computer software to perform objective measurements of photos of their patients taken in the preoperative and postoperative periods, using the pupil and some points marked in the eyebrow, in a maximally relaxed position with the eyes open, as reference points, but without a fixed reference point for a reliable measurement. Such characteristics render that study difficult to replicate and use in plastic surgery practice. Furthermore, the study fails to report the population measurements, instead reporting the pre- and postoperative measurements of each patient.
The present study assigned a degree of ptosis to each interval, ranging from degree I to degree IV, thereby refining the assessment by the surgeon. Each degree was correlated with a numerical range in which > 1.8 cm is the normal range, 1.7-1.5 cm corresponds to degree I ptosis, 1.4 - 1.2 cm to degree II ptosis, 1.1 - 0.9 cm to degree III ptosis, and < 0.8 cm to degree IV ptosis. Surgery was indicated for degrees II, III, and IV.
Thus, defining the degree of ptosis of the eyebrow tail enables surgical decision-making, by always matching the objective measurement data to the clinical complaint of the patient for improved surgical outcome.
To date, these characteristics and objectives were found in no other publication, which highlights the originality of the present study, defining an unpublished classification based on objective measurements and well-defined, easily established, anatomical parameters with small differences between age groups and ethnicities.
The present study is based on a Brazilian population, which has significant intermixing, and therefore may be useful for populations with similar characteristics.
However, this classification may also be valid for populations on other continents because the values found may reflect the average of the world population, given the characteristics of the Brazilian population.
A caveat is also associated for differences between genders because the individual male values are significantly lower than the female values. Therefore, when suggesting a surgical procedure to a male patient, the physician should seek the best outcome for the patient instead of the value in the classification, which is only meaningful when the patient describes a clinical complaint.
The present study develops a follow-up tool for patients during the aging process, similar to the portraits painted by Albrecht Dürer, who began self-portraits at age 13 and continued until he was no longer able to paint18, thereby recording his aging process. Thus, the classification proposed herein will objectively help plastic surgeons to standardize the follow-up of patients and outcomes, and provides further data for differential diagnosis, including those for palpebral pseudoptosis.
CONCLUSION
The objective measurement of the eyebrow tail position enables classification of the degree of ptosis and can guide surgical decision-making.
COLLABORATIONS
DSSR Data analysis and/or interpretation; statistical analysis; final manuscript approval; study design; performing surgeries and/or experiments; manuscript writing or content review analysis.
RPR Data analysis and/or interpretation; study design.
RGFF Study design; performing surgeries and/or experiments.
EBG Final manuscript approval; study design; manuscript writing or content review analysis.
LMF Final manuscript approval; study design; manuscript writing or content review analysis.
REFERENCES
1. Bramly S. Leonardo da Vinci. Rio de Janeiro: Imago; 1989. 103p.
2. Shaw RB Jr, Katzel EB, Koltz PF, Yaremchuk MJ, Girotto JA, Kahn DM, et al. Aging of the facial skeleton: aesthetic implications and rejuvenation strategies. Plast Reconstr Surg. 2011;127(1):374-83.
3. Matros E, Garcia JA, Yaremchuk MJ. Changes in eyebrow position and shape with aging. Plast Reconstr Surg. 2009;124(4):1296-301.
4. Aymar GC. The Art of Portrait Painting: Portraits through the centuries as seen through the eyes of a practicing portrait painter. Philadelphia: Chilton Book; 1967. 93p.
5. Naif-de-Andrade NT, Hochman B, Naif-de-Andrade CZ, Ferreira LM. Computerized photogrammetry used to calculate the brow position index. Aesthetic Plast Surg. 2012;36(5):1047-51.
6. Packiriswamy V, Kumar P, Bashour M. Photogrammetric analysis of eyebrow and upper eyelid dimensions in South Indians and Malaysian South Indians. Aesthet Surg J. 2013;33(7):975-82.
7. Jones BM, Lo SJ. The impact of endoscopic brow lift on eyebrow morphology, aesthetics, and longevity: objective and subjective measurements over a 5-year period. Plast Reconstr Surg. 2013;132(2):226e-238e.
8. Hamamoto AA, Liu TW, Wong BJ. Identifying ideal brow vector position: empirical analysis of three brow archetypes. Facial Plast Surg. 2013;29(1):76-82.
9. Nahai FR. The varied options in brow lifting. Clin Plast Surg. 2013;40(1):101-4.
10. Lee NG, Callahan AB, Migliori ME, Freitag SK. Minimally invasive approaches to eyebrow lifting. Int Ophthalmol Clin. 2013;53(3):47-57.
11. Lee JW, Cho BC, Lee KY. Direct brow lift combined with suspension of the orbicularis oculi muscle. Arch Plast Surg. 2013;40(5):603-9.
12. Matai O, Lavezzo MM, Schellini SA, Padovani CR, Padovani CR. Evaluation of eyebrow position using angular measures. Arq Bras Oftalmol. 2007;70(1):41-4.
13. Paiva HJ. Noções e Conceitos Básicos em Oclusão: Disfunção Temporomandibular e Dor Orofacial. São Paulo: Santos; 2008.
14. Atran S. Cognitive foundations of natural history: towards an anthropology of science. Cambridge: Cambridge University Press; 1990.
15. Hochman B, Nahas FX, Ferreira LM. Photography in medical research. Acta Cir Bras. 2005;Suppl 2:19-25.
16. Hwang K. Surgical anatomy of the upper eyelid relating to upper blepharoplasty or blepharoptosis surgery. Anat Cell Biol. 2013;46(2):93-100.
17. Fitzgerald R. Contemporary concepts in brow and eyelid aging. Clin Plast Surg. 2013;40(1):21-42.
18. Hope-Hennessy J. The Portrait in the Renaissance. New York: Bollingen Foundation; 1966. 348p.
1. Sociedade Brasileira de Cirurgia Plástica, São Paulo, SP, Brazil
2. Universidade Federal de São Paulo, Escola Paulista de Medicina, São Paulo, SP, Brazil
Institution: Universidade Federal de São Paulo, Escola Paulista de Medicina, São Paulo, SP, Brazil.
Corresponding author:
Daniel Sundfeld Spiga Real
Rua Passeio das Palmeiras, 520, Apto 71 Torre 1 - Parque Faber Castell I
São Carlos, SP, Brazil Zip Code 13561-353
E-mail: daniel.ssr@hotmail.com
Article received: September 8, 2015.
Article accepted: May 12, 2016.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket