



Articles - Year 2003 - Volume 18 -
Anatomical Study of the Superior Pedicle of Retroauricular Skin Flaps
Estudo Anatômico do Pedículo Superior do Retalho Cutâneo Retroauricular
ABSTRACT
Since the description of the flap proposed by Washio in 1969, several vascular pedicle models have been designed for the retroauricular flap, aiming chiefly to reduce the thickness of the pedicle so as to migrate the flap as an island. In spite of those advances, there are still problems such as venous stasis and partial loss of the flap. In a study in cadavers, twenty pedicles were dissected in order to find the presence or absence of veins in the region, maximum length of the pedicle and anatomical reference points for a safe dissection. All pedicles were located. The venous distribution found, that was different from that described in other studies, could account for the problems in venous drainage.
Keywords: retro auricular flap; vascular pedicle
RESUMO
Desde a descrição do retalho proposto por Washio em 1969, foram idealizados diversos modelos de pedículo vascular para o retalho retroauricular, visando principalmente à diminuição da espessura do pedículo a fim de migrar o retalho de forma ilhada. Apesar desses avanços, existem ainda problemas tais como estase venosa e perda parcial do retalho.
Em estudo cadavérico, foram dissecados vinte pedículos procurando estabelecer a presença ou ausência de veias na região, comprimento máximo do pedículo e pontos de reparo anatômicos para uma dissecção segura.Todos os pedículos foram localizados, e a distribuição venosa encontrada, não descrita em outros estudos, poderia explicar os problemas de drenagem venosa.
Palavras-chave: Retalho retroauricular; pedículo vascular
Reconstructions of the face with local skin flaps have always been a problem for repair surgery. This is because, in addition to the need to find thin skin, with a color that is compatible with the facial skin and free from hair, there were also the scars of the donor site, which, no matter how discreet they are, will always be a serious unaesthetic problem that surgeons have to deal with.
In 1969, Washio(1) described a retroauricular flap with a pedicle on the superficial temporal artery, through the superior auricular artery, which seemed to solve the problems mentioned above. This flap would enable taking a hair-free area measuring up to 40 cm2, thus making it possible to satisfactorily correct most of the acquired facial defects. In spite of that, we noticed that the pedicle of Washio(2) flap, because ir contained skin and was 6.0 cm or thicker(2), still left an esthetic sequella for patients who underwent this surgery(3).
Trying to solve this problem, Guyuron(4), in 1985, described a thinner subcutaneous pedicle and reported the successful reconstruction of orbits.
Kolhe & Leonard(5) also suggested alternatives with pedicle flaps on the posterior auricular artery, a branch of the external carotid, even though the pedicle of approximately 7cm had a limited reach for the reconstruction of more distant sites.
Other authors who worked with flaps related to the retroauricular region, with a superior pedicle, were Kobayashi et al.(6) and Song et al.(7). The first group described, in 1995, a technique with a subcutaneous pedicle, whose cutaneous portion had pilous and glabrous areas, thus serving chiefly to the reconstruction of the frontal area. The second group described, in 1996, the skeletization of the pedicle and demonstrated, similarly to Guyuron, excellent reconstructions of orbits.
In spite of all these alternatives (Fig. 1), Kobayashi(8) reported that he lifted ten pedicle retroauricular flaps on the superficial temporal artery, thus obtaining, in most cases, signs of congestion due to the fact that the superior auricular vein provides insufficient venous drainage and recommended further studies on the matter.
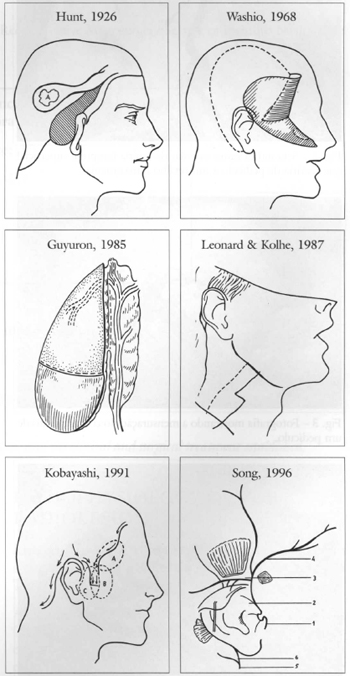
Fig. 1 - Alternatives proposed for the utilization of the retroauricular flap.
This paper, through the dissection of cadavers, tries to identify the causes of the problems mentioned above, and to define anatomical parameters for a safer performance of this flap.
MATERIAL AND METHOD
Seven cadavers with less than 12 hours were dissected in the FMUSP verification of death service, so as to observe the vascular anatomy of the retroauricular region, particularly the anastomoses between the posterior auricular artery and the superficial temporal artery that comprise the superior pedicle of the retroauricular flap.
Once the anatomy of the pedicle had been identified, its length, distance between anatomical reference points (superior border of the external ear canal) and thickness of the superior auricular artery were measured. Measures were determined with a surgical ruler and a pachymeter. For greater precision, the measure of the thickness of the artery was taken with a magnifying lens (three-fold enlargement).
This srudy also used six cadavers in formal de hyde from the Medical School of Santo Amaro University (UNISA), and pre-auricular dissections were performed in one ear of each body.
Spearman's correlation test (Siegel, 1988) was used for the statistical analysis, fixing the level of rejection of the null hypothesis at 0.05, that is, 5%.
RESULTS
We obtained the results observed in Table I by analyzing the dissections we performed.
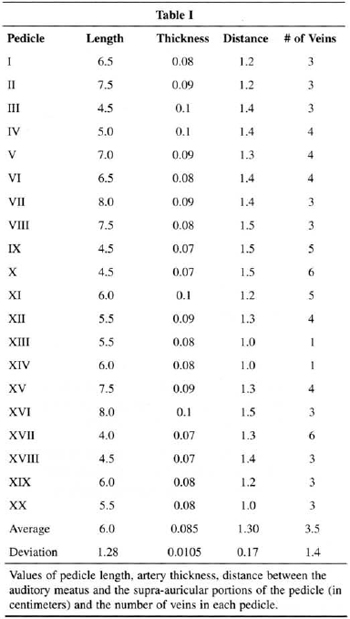
All pedicles were found and they were positioned 1.0 to 1.5 cm above the orifice of the external ear canal (Fig. 2). Average was 1.3 cm and standard deviation was 0.17.
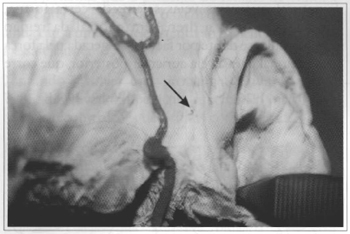
Fig. 2 - Arrow indicates vascular branch of the superficial temporal artery that will serve as a pedicle to a retroauricular fiap.
The measure of the pedicle given by the length of the superior auricular artery, added to the length of the superficial temporal artery ligated and sectioned after the origin of the posterior auricular artery, ranged between 4.0 cm and 8.0 cm, with an average of 6.0 cm (Fig. 3) and standard deviation of 1.28.
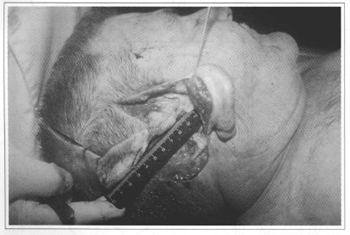
Fig. 3 - Photography showing the measuring of the pedicle length.
The thickness of the superior auricular artery ranged from 0.07 to 0.1 em, with an average of 0.085 cm and standard deviation of 0.0105.
We also noted that the twenty pedicles examined showed the predominance (10:1) of a venous pattern formed by three to six veins with peri-arterial disposition, alternating with subcutaneous cellular tissue over the artery and vein patterns concomitantly. As to the number of veins found per pedicle, 45% of cases had 1 artery and 3 veins. The model with 1 artery and 4 veins was present in 25 % of the cases, and the models with 1 artery and 5 veins, 1 artery and 6 veins, and 1 artery and 1 vein, in 10% of the cases.
After submitting the groups to Spearman's correlation test, we observed that there was no significant correlation between the length of the pedicle and the thickness of the artery (R=0.28).
There was no significant correlation between the groups for the length of the pedicle and the distance between it and the point of reference (R=0.035).
The correlation tests between thickness of the pedicle artery and distance between it and the auditory meatus (point of reference) did not provide a significant correlation either (R=0.0106).
As to the length of the pedicle in relation to the number of veins, we obtained R=0.26 (not significant), and as to the number of veins in relation to the thickness of the artery R=0.08 (not significant).
DISCUSSION
The data collected suggest that the retroauricular flap, dissected and rotated according to the technique proposed by Song et al., presents venous congestion (Fig. 4) and possible necrosis, because its vascular pedicle is usually made up (90%), of an artery of considerable blood flow for the size of the flap and a set of thin veins not large enough for venous drainage, which may, therefore, lead to edema and poor circulation.

Fig. 4 - Congested retroauricular fiap.
It is natural that these veins be somewhat hypoplasic, because the natural drainage of the retraauricular region occurs by facilitation of the gravitational force into the posterior auricular vein, located caudally, and that runs along the posterior auricular artery, ending in the external jugular vein.
We believe that the retraauricular flap may be successfully performed pravided three recommendations are observed. The first refers to the position of the pedicle to be dissected, which should be located fram 1.0 to 1.5 em above the auditory meatus and not necessarily above the implantation of the ear. The second recommendation is that, knowing that the reach of the pedicle is on average 6.0 cm, the coverage of more distant areas should not indicated, so as to avoid exerting traction on its vascular structures. Another recommendation is the autonomization of the flap eight days before its ratation (a technique proposed in Kobayashi's paper), so that the venous flow of the pedicle increases and insufficient postoperative drainage is avoided.
This is a relatively new concept, as autonomization is normally used to increase arterial blood supply.
CONCLUSIONS
Based on the dissection of the superior pedicle of the retraauricular skin flap in 20 specimens, the following conclusions could be drawn:
1. The pedicle was found in a region 1.0 to 1.5 cm vertically above the auditory meatus.
2. This flap is indicated to cover areas up to 6.0 cm away fram the tragus.
3. The autonomization of the flap should be previously performed as a safety measure.
REFERENCES
1. Washio H. Retroauricular temporal fiap. Plast Reconstr Surg. 1969; 43:162-6.
2. Washio H. Further experiences with the retroauricular temporal fiap. Plast Reconstr Surg. 1972; 50:160-2.
3. Maillard G, Montandon D. The Washio tempororetroauricular. Plast Reconstr Surg. 1982; 70:550-9.
4. Retroauricular island flap for eye socket reconstruction. Plast Reconstr Surg. 1985; 76(4):527-30.
5. Kolhe P,Leonard A. The posterior auricular flap: Intra-oral reconstruction. Br J Plast Surg. 1987; 40:570-8l.
6. Kobayashi S, YozaS, Kakibuchi M, Sekiguchi J, Ohmori K. Retroauricular hairline flap transfer to the face. Plast Reconstr Surg. 1995; 96:42-7.
7. Song R, Song Y, Qi K, Jiang H, Pan F. The superior auricular artery and retroauricular arterial island flaps, Plast Reconstr Surg. 1996; 98:657-69.
8. Kobayashi S. Discussion. Plast Reconstr Surg. 1996; 98:668-9
I - Head Medical Resident of the Plastic Surgery Clinic of the Universidade de Santo Amaro.
II - Professor of the Discipline of Collective Health of the Universidade de Santo Amaro.
III - Surgeon of the Head and Neck Clinic of Hospital Heliópolis, Director of the Surgical Clinics of Hospital Heliópolis.
IV - Professor of the Discipline of Plastic Surgery of the Universidade de Santo Amaro.
Universidade de Santo Amaro - Head and Neck Clinic of Hospital Heliópolis - Faculdade de Mecicina da Universidade de São Paulo (FMUSP) Death Verification Service
Address for correspondence:
Oscar Porto, MD
Rua Prof. Artur Ramos, 183 - cj. 113
Jardins 01454-011 - São Paulo - SP Brazil
Phone: (55 11) 3813-0688
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket