



Case Report - Year 2016 - Volume 31 -
Elastic suture as an alternative for the initial wound care in the emergency room
Sutura elástica como alternativa para o primeiro atendimento de ferida na urgência
ABSTRACT
This is a case report of a 44-year-old male patient who was admitted to the emergency room on November 17, 2013, after an accident with a Makita Disc. The patient presented with an extensive wound throughout the dorsal surface of the left thumb, with tendon exposure. The use of elastic suture is demonstrated as the initial care in the emergency department. We present satisfactory resolution in a single surgical procedure of traumatic wounds in a patient presenting with loss of tissue. The chosen surgical approach presented adequate aesthetic result and functional preservation.
Keywords: Sutures; Ambulatory care; Wounds and injuries; Emergency.
RESUMO
Relato do caso de um paciente do sexo masculino, 44 anos, que deu entrada pelo Serviço de Emergência, no dia 17 de novembro de 2013, vítima de acidente com disco de Makita, apresentando ferida extensa em toda face dorsal do primeiro quirodáctilo esquerdo e exposição tendínea. Demonstra a utilização de sutura elástica, em atendimento inicial na urgência, e a possibilidade de tratamento de ferida traumática com perda de substância, com resolução satisfatória em único tempo cirúrgico. A opção cirúrgica apresentou resultado funcional adequado e preservação estética.
Palavras-chave: Suturas; Assistência ambulatorial; Ferimentos e lesões; Urgência.
Various techniques are necessary for the repair of complex wounds and these could be challenging for the surgeon in emergency care. The main objective for the first approach in the emergency department is to achieve a satisfactory functional and aesthetic result.
According to Oliveira and Nigri, care of wounds resulting from trauma continues to present great difficulties for surgeons1.
In relation to the importance of the treatment of complex wounds, authors describe that the traditional methods of tissue coverage in open wounds after high-energy trauma initially need repeated surgical procedures, such as debridement of devitalized tissues, serial dressings, and reconstructions with the use of grafts or flaps in one or more surgical interventions2.
The elastic suture can serve as an additional alternative to the conventional surgical repair prepared with grafts and flaps or primary closure.
The technical option of elastic suture can be used for extensive lesions with an important loss of tissue3.
Petroianu4 reported that the elastic suture of wounds is a frequently used option in closing large wounds, such as those due to larger traumas, excision of large tumors, and in cases of dehiscences after laparotomies.
Wounds treated with elastic sutures will close gradually, by progressive mobilization of the skin due to continuous tension from the elastic band. Additionally, subsequent procedures can be avoided when this technique is used.
There are few published studies in the literature about the importance of elastic suture of extensive wounds. These reports describe that this procedure is an effective alternative, can be used in a large number of cases, and presents satisfactory results1.
Although the elastic suture is used more commonly for treatment of dehisced wounds, the authors describe a case in which it was used in emergency care.
OBJECTIVE
To identify traumatic and complex hand wound using an elastic suture, as a primary approach for wound care in the emergency room
CASE REPORT
LCSB, 44 years, male patient, painter, was admitted to the Hospital Estadual Azevedo Lima (HEAL), Niterói, RJ. Patient was injured in an accident produced by a circular saw disk )Makita®), in November 2013. Physical examination revealed an extensive lesion of the dorsal side of the left thumb (LT), with an important loss of tissue and exposed tendon. This wound had a rectangular form, with dimensions of 4.0 cm (in its largest axis) by 2.0 cm, and was relatively large when compared with the smaller dimensions of the thumb, in addition to its sensitive location and possible functional consequences.
The diagnosis was based on physical examination and hand radiography, which showed no bone injury.
The wound was treated surgically and closed with elastic sutures that remained in place for a week. After anesthetic block of the LT was applied, reconstructed with elastic suture of the dorsal wound of the LT, with elastic material of the grip of sterile gloves, being fixed to the edges of the wound through nylon 3-0 sutures, with a distance of approximately 0.5 cm between sutures, in the Surgical Center (Figure 1). The compression force applied was adequate for approximation of the wound. In the case in question, the segment length of the elastic was the grip of a sterile glove number 8.5, enabling the complete approximation of the wound.

Figure 1. Postoperative aspect of elastic suture.
In the reproduction of the technique, an elastic fixation was initially made with nylon 3-0, in the proximal part and along the wound, with new and successive fixations on the edges of the wound and crosses in "X" up to the distal part, as to favor the compression forces to close the wound edges. At the end of the suture, we added an elastic traction, toward the end of the thumb, as a new and additional strength, in an attempt to improve the reconstruction of the wound.
We believe that this aspect is important for the best result and improvement of the technique.
After a week of maintaining the elastic suture, this was discontinued and conventional suture of the wound with nylon 3-0 was performed. Special attention was paid in order to avoid tension in the suture line during the procedure. Patient was discharged from hospital on the same day. A week later, during an outpatient follow up, interspersed withdrawal of nylon sutures was done and nine days later, sutures of the finger were completely removed.
The study was evaluated and approved by the Ethics Committee of the institution where the study was performed, with the registration number 01/2015.
The immediate complication we observed was a mild local pain, but with good response to common pain medication such as dipyrone. In the immediate postoperative period, the clinical course was favorable, with absence of tissue ischemia and maintenance of capillary perfusion in the affected area. Since the lesion could lead to edema of the thumb and the possibility of impairment of perfusion in the digit, manual vascular Doppler and clinical examinations for tissue perfusion were used to assess the circulation status of the digit.
There were no complications and no wound dehiscence, infection, or seroma were observed (Figure 2). Conventional suture of the wound with nylon 3-0 was performed fifteen days after the withdrawal of the elastic suture.
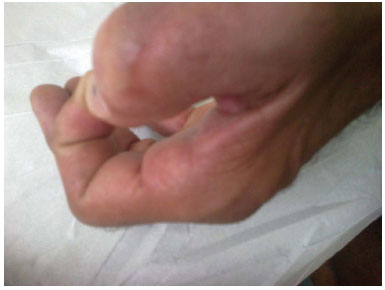
Figure 2. Late postoperative period, satisfactory scar without functional impairment.
The patient recovered well and presented a discreet functional impairment of the left thumb, as a late complication. He was referred for evaluation and follow-up by the Physical Therapy Service, after a month. It was recommended active daily movements of the injured digit in the home environment, under the guidance and supervision of the Physiotherapy Service. Outcome was good with complete resolution of the functional deficit.
In the outpatient follow-up, two months after surgery, the scar presented a good appearance, digit was without functional deficit, with normal range of flexion and extension, and pincer position of the preserved left thumb (Figure 2). Hospital discharge was held with guidance.
DISCUSSION
Repairs of traumatic wounds present great technical difficulty, and there are several procedures that can be used for skin coverage, including grafts and flaps.
In 1993, Raskin5 reported the use of an elastic suture for treatment of compartmental syndrome of the upper limb, approaching the aponeuroses with elastic rubber bands, avoiding closures under tension, or the need for skin grafts for coverage of the injuries left open. The elastic suture described by Raskin has proven to be efficient in the treatment of these skin lesions with tissue loss, with good aesthetic and functional results5.
The elastic suture for wound healing has been reported by Brazilian authors. Petroianu4 used elastic sutures in cases of approximation for extensive lesions with an important loss of substance and for the closure of large wounds. It has been used also, in an extensive number of lesions, such as those arising after the excision of large tumors of the abdominal wall, removal of Marjolin ulcers, secondary wounds after severe infections of the soft parts and abdominal stomas after laparotomy, large wounds resulting from extensive necroses of decubitus ulcers and large, hemorrhagic areas on the scalp. In another study, the author describes the approximation of the edges of large wounds of the abdominal wall, using an elastic rubber strip kept under moderate tension, which can be used in many surgical circumstances3.
Oliveira and Nigri1 showed that the use of an elastic suture is an effective, cheap technique, with good aesthetic results and rapid implementation for the closing of escharotomies and fasciotomies in burned patients.
Nigri and Oliveira2 presented the complete closing of the large wounds secondary to diverse traumas in the lower limbs. They divide the procedure in two stages, the first, by approximation of the opposite edges of the wound with a circular elastic rubber band and the second step few days later, with the withdrawal of the elastic bands, followed by simple suture with mono nylon.
The "elastic technique" has also been used for the treatment of extensive loss of soft tissues after open fractures and after incisions for open reduction or fasciotomy. The wound closes gradually by facilitated mobilization of the skin in response to a continuous tension from the rubber band, being, according to Mosheiff et al.6, a safe, simple and efficient method.
Another use of the elastic method is for protecting the skin graft in its receptor bed, with adequate compression to reduce the size of the dead space and avoid the formation of a hematoma, under the graft7.
Bellón et al.8 analyzed the behavior of two new elastic sutures materials in a rabbit model of midline incision closure. Histological sections of the tissue-embedded sutures were subjected to morphological, collagen expression, macrophage response, and uniaxial tensiometry studies. The authors believe they had a less tense suture because the cicatricial retraction, which usually occurs, was lower, They managed to reduce the closing time of the lesion, resulting in economic gain, by decreasing the time of hospitalization.
In the case described herein, we apply compression forces along the wound (fixing the elastic suture to the edges of the wound), being, for example, on the x-axis, and another compression force, fixed toward the end of the thumb, for example, in the y-axis.
According to Halliday et al.9, classical physical mechanics focuses attention on the movement of a body in particular, where it interacts with neighboring bodies (its neighborhood), such that a change of speed produces an acceleration. Isaac Newton (1642-1727), establishing the laws of the movement, formulated the framework of classical mechanics, where: (1) he introduced the concept of force F (considered a pull or push) and definition of the acceleration of a body; (2) the assignment of a mass m to a body; and (3) found ways to calculate the forces that act on the bodies and its neighborhood9.
In the example in Figure 39, a force of 4 N is applied along the x-axis and a force of 3 N along the y-axis. Experimentally, a force of 4N in the x direction has produced an acceleration of 4 m/s2, and the force of 3N in the y direction has produced an acceleration of 3 m/s2. When the forces are applied simultaneously, one can verify that there is an acceleration of 5 m/s2 and force of 5N, directed along the line with an angle of 37° with the x-axis. Experiments of this nature demonstrate, in conclusion, that the forces are vectors: they have module, direction and magnitude, and are added up according to the law of vector addition9.
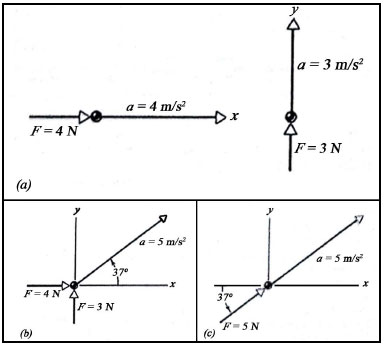
Figure 3. (a) Forces and accelerations in x and y directions; (b) Forces applied simultaneously; (c) Resulting force and acceleration.
The choice of surgical emergency treatment in cases of injuries with loss of skin integrity and functional impairment varies in each case. The main objective of surgical repair is the suture of soft tissues, confection of grafts and flaps when needed, maintenance of the function and the viability of the affected segment.
Despite the satisfactory reports of the authors mentioned above, there are still limitations of the suture method using elastic rubber strips, since there are only few studies published in the literature. Further studies need to be performed and published.
CONCLUSION
This article presents the description of a case with loss of tissue and tendon exposure of the left thumb, treated in the emergency room, where it was possible to surgically close the wound with elastic sutures, with satisfactory aesthetic and functional results.
REFERENCES
1. Oliveira RA, Nigri EL. Sutura elástica no tratamento de escarotomias e fasciotomias de pacientes queimados. Rev Bras Queimaduras. 2012;11(2):63-6.
2. Santos ELN, Oliveira RA. Sutura elástica para tratamento de grandes feridas. Rev Bras Cir Plást. 2012;27(3):475-7. DOI: http://dx.doi.org/10.1590/S1983-51752012000300026
3. Petroianu A. Opção técnica para a síntese de grandes feridas da parede corpórea. Rev Col Bras Cir. 2009;36(4):353-5. DOI: http://dx.doi.org/10.1590/S0100-69912009000400015
4. Petroianu A. Síntese de grandes feridas da parede corpórea com tira elástica de borracha. Acta Med Port. 2011;24(3):427-30.
5. Raskin KB. Acute vascular injuries of the upper extremity. Hand Clin. 1993;9(1):115-30.
6. Mosheiff R, Segal D, Rand N, Liebergall M. The "rubber band technique": a simple method for closing large skin defects. Am J Orthop (Belle Mead NJ). 1999;28(11):665-6.
7. Ersoy B, Şirinoğlu H, Tezel E. Tie-over dressing with criss-cross lacing pattern. Dermatol Surg. 2011;37(11):1671-3. DOI: http://dx.doi.org/10.1111/j.1524-4725.2011.02165.x
8. Bellón JM, Pérez-López P, Simón-Allue R, Sotomayor S, Pérez-Köhler B, Peña E, et al. New suture materials for midline laparotomy closure: an experimental study. BMC Surg. 2014;14:70. DOI: http://dx.doi.org/10.1186/1471-2482-14-70
9. Halliday D, Resnick R, Krane KS. Capítulo 5: Força e Leis de Newton. In: Halliday D, Resnick R, Krane KS. Fundamentos da Física, Volume 1 - Mecânica. Rio de Janeiro: Livros Técnicos e Científicos; 1996. p.72-96.
1. Sociedade Brasileira de Cirurgia Plástica, Rio de Janeiro, RJ, Brazil
2. Hospital Estadual Azevedo Lima, Niterói, RJ, Brazil
3. Universidade Federal do Rio de Janeiro, Rio de Janeiro, RJ, Brazil
Institution: Hospital Estadual Azevedo Lima, Niterói, RJ, Brazil.
Corresponding author:
Antonio Petraglia Neto
Estrada Francisco da Cruz Nunes, 7465
Niterói, RJ, Brazil Zip Code 24350-310
E-mail: a.petraglia@hotmail.com
Article received: May 26, 2014.
Article accepted: October 8, 2015.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket