



Original Article - Year 2016 - Volume 31 -
Segmented scalp peninsula to prevent a raised hairline and misalignment in rhytidoplasty
Península capilar segmentada, como prevenção da ascensão capilar e seu desalinhamento nas ritidoplastias
ABSTRACT
INTRODUCTION: Rhytidoplasty has shown excellent results in the treatment of facial laxity over the years, but in a few cases in which the patient has increased facial laxity associated with high preauricular scalp implantation, we observed elevation of implantation above the root of the helix after flap traction, resulting in an unesthetic facial appearance and marring the surgical procedure. The objective of this study was to demonstrate a surgical technique designed to prevent hairline recession and maintain correct alignment for the facelift.
METHODS: Of 25 patients who underwent rhytidoplasty, 12 received a segmented scalp peninsula. Descriptive analysis in this group included age, level of scalp implantation, surgical time, elevation of the hairline, necrosis, postoperative hematoma, unesthetic scars, and neuropraxia.
RESULTS: We analyzed the results of a segmented scalp peninsula in 12 patients, ranging in age between 41 and 74 years, with a mean of 60 years. The return to usual activities ranged from 10 to 21 days. No unesthetic changes resulted from placement of the hairline on the sideburn in these 12 patients; there was one (4%) case of hematoma, but no case of necrosis or neuropraxia.
CONCLUSION: The segmented scalp peninsula is an easily performed technique, with a low risk of complications and with satisfactory esthetic results.
Keywords: Rhytidoplasty; Plastic surgery/methods; Rejuvenation; Hair.
RESUMO
INTRODUÇÃO: A ritidoplastia tem demonstrado excelentes resultados no tratamento da flacidez facial ao longo dos tempos, porém em alguns casos selecionados, nos quais o paciente apresenta flacidez facial acentuada associada com implantação capilar pré-auricular alta, observamos, após a tração dos retalhos, uma ascensão da implantação capilar acima da raiz da helix, causando um aspecto inestético facial e configurando um estigma cirúrgico para o procedimento. O objetivo desse estudo é demonstrar uma técnica cirúrgica com intuito de prevenir a ascensão capilar e manter o seu correto alinhamento, no lifting facial.
MÉTODOS: Foram operados 25 pacientes, submetidos à ritidoplastia, dos quais 12 realizamos a península capilar segmentada. Foi realizada uma análise descritiva desse grupo, quanto à idade, altura da implantação capilar, tempo cirúrgico, elevação do "pé do cabelo", necrose, hematoma pós-operatório, cicatrizes inestéticas e neuropraxia.
RESULTADOS: Em relação à população analisada, realizamos a península capilar segmentada em 12 pacientes, ou seja, 48%, a idade variou entre 41 e 74 anos, sendo a média de 60 anos. O retorno às atividades habituais variou de 10 a 21 dias. Não ocorreram alterações inestéticas da implantação da linha capilar na "costeleta" nos 12 pacientes submetidos à península capilar segmentada, houve um (4%) caso de hematoma, nenhum caso de necrose ou neuropraxia.
CONCLUSÃO: A península capilar segmentada demonstrou ser uma técnica de fácil execução, baixo índice de complicações e com resultados estéticos satisfatórios.
Palavras-chave: Ritidoplastia; Cirurgia plástica/Métodos; Rejuvenescimento; Cabelo.
Aging is one of the certainties of life that we must face, with the passage of time. The perception of aging and the way we deal with self-image varies among individuals, with different beliefs and behaviors. Surgery has emerged as a tool to freeze time or to regain the youthfulness lost with the uncertainties of life.
Rhytidoplasty has shown excellent results in the treatment of facial laxity since the procedure was described by Charles Conrad Miller in 1907. However, in selected cases in which the patient had increased facial laxity associated with high preauricular scalp implantation, we observed an elevation in hairline implantation above the root of the helix after oblique flap traction, resulting in unesthetic facial appearance and marring the surgical procedure. Our initial intention was to categorize the level of the hairline as high, medium, or low, thus enabling improved prognosis and prevention of elevation of the sideburn. This standardization simplifies learning of the technique, making it teachable and reproducible for medical residents.
OBJECTIVES
Describe and systematize the technique of the segmented scalp peninsula procedure, with the indications and preparation of patients undergoing rhytidoplasty.
Describe a sample of the patients operated on in the past three years using this method.
Demonstrate the indices of recession and misalignment of the hairline.
METHODS
Female patients who underwent rhytidoplasty were analyzed prospectively, with a segmented scalp peninsula performed in the group classified as having a high or medium hairline in the preauricular region between 2011 and 2014 at the Fluminense Plastic Surgery Clinic/Niterói D'or Hospital, Niterói - RJ, and at the University Hospital of Marília - SP. All surgeries were performed by the author.
We will proceed to the description of the sample without the use of statistical comparisons. The data collected included:
1. Age
2. Level of the hairline in the preauricular region
3. Surgical time
4. Elevation of the hairline in the preauricular region
5. Unsightly scars
6. Hematoma
7. Cutaneous necrosis
8. Neuropraxia
Surgical Technique
1. The preparation of the patient involved: shaving, anesthesia, antisepsis, and field infiltration, for a procedure duration of approximately 45 minutes.
2. General anesthesia was supplemented with local infiltration as described below.
3. The infiltration of the surgical field was performed with a solution of 20 ml of 2% lidocaine hydrochloride (400 mg), 20 ml of 0.75% ropivacaine hydrochloride (150 mg), 0.5 ml of 1:1,000 epinephrine, and 460 ml of 0.9% saline solution, for a total of 500.5 ml. The epinephrine concentration was approximately 1:1,000,000.
4. The operative time ranged from 4.5 to 6.0 h.
5. All patients were drained with a closed suction system, which was removed 24 h after surgery.
6. The patients were discharged 24 h after the procedure in all cases.
We performed the peninsula technique introduced by Professor Ronaldo Pontes1,2 in 1999, and modified the procedure in order to preserve the hairline and alignment at the end of the sideburn with less scarring. We followed the parameters of the technique to circumvent the hairline by approximately 2.5 to 3 cm, but unlike the original procedure, we preserved a "mutton chop" the end of the sideburn of approximately 1 to 2 cm (Figures 1, 2, and 3), and continued the incision into the temporal scalp. The fact that the incision is interrupted by the transition to the hairline implantation at the end of the sideburn eliminates the risk of misalignment in this region (Figure 2 and 4).

Figure 1. When marking for the segmented capillary peninsula, maintain a circle defining the preservation of a skin segment at the end of the sideburn.

Figure 2. Incision for the segmented capillary peninsula.

Figure 3. Flap traction with preservation of the scalp implantation (hairline).

Figure 4. Temporal traction with preservation of the hairline alignment at the end of the sideburn.
RESULTS
From March 2011 to March 2014, of 25 patients who underwent rhytidoplasty, a segmented scalp peninsula procedure was performed in 12 (48%), for a high or medium hairline implantation. The age ranged between 41 and 74 years (Figure 5), with an average of 60 years. The return to usual activities ranged from 10 to 21 days. No unesthetic changes occurred with the implantation of the hairline on the sideburns in these 12 patients; one (4%) patient had an elevation of the hairline implantation above a desirable level because the segmented peninsula was not performed due to a classification error. There was one (4%) case of hematoma with closed suction drainage, which resolved with a manual drain. In one case, a seroma located in the lateral cervical region developed on the 6th postoperative day, and was treated with needle (1.20 x 40 mm) puncture and aspiration, as suggested by Destro et al.3. No necrosis, unsightly scarring, or neuropraxia was observed.
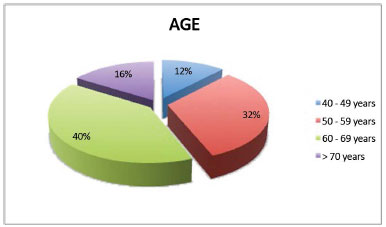
Figure 5. Population distribution by age.
We optimized the level of standardization of the preauricular hairline implantation as shown in (Chart 1) and illustrated in (Figures 6, 7, and 8).
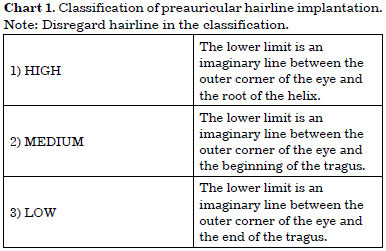

Figure 6. Implantation above the root of the helix, considered high, pre- and post-segmented capillary peninsula.

Figure 7. Secondary facelift: high implantation, with pre- and post-segmented capillary peninsula.

Figure 8. Average implantation of the sideburn, pre- and post-segmented capillary peninsula.
The patients were divided by hairline level as high (Figures 9 and 10), medium, (Figure 11), or low.

Figure 9. Average implantation, pre- and post-segmented capillary peninsula.

Figure 10. Average implantation, previously classified as low, without the peninsula. Note the elevation of the "hairline." Note: Disregard the hairline in the classification.

Figure 11. Low implantation, without the peninsula. Elevation of the capillary implantation without compromising the esthetic result, pre and post.
DISCUSSION
Castro et al.4 and Menezes et al.5 reported optimal analysis of results after the 4th postoperative month, and we also adopted this approach. Despite the many publications on rhytidoplasty, few studies describe methods designed to prevent a raised hairline.
A raised hairline is unsightly and undesirable in rhytidoplasty, especially in patients with high or average preauricular scalp implantation who do not undergo any technique designed to preserve the level of the sideburn. Professor Pontes introduced the peninsula in 1999 to remedy the problem of excessive elevation of the hairline, as did the compensating triangle described by Neves et al.6. Both techniques have demonstrated effectiveness in preservation of hairline implantation, with excellent esthetic results.
This work aimed to systematize the indication for a technique designed to preserve high or medium hairline implantation, regardless of whether the peninsula, compensation triangle, or the segmented scalp peninsula is used. Patients with low scalp implantation have a contraindication to any method of preservation of the hairline. The segmented scalp peninsula is a technique designed to preserve the level of the hairline and alignment to the end of the sideburn, with less scarring. It is one more option, among others7-15, in facial surgery.
Positive results and satisfactory evaluation by many patients will lead to improvement in techniques, in search of natural and lasting results.
CONCLUSION
The objective of facial rejuvenation surgery is to achieve a fresh and natural appearance. The peninsula, especially as a segmented procedure, fulfills these criteria with satisfactory results.
REFERENCES
1. Pontes R. Península. In: Pontes R, ed. O universo da ritidoplastia. Rio de Janeiro: Revinter; 2011. p.119-46.
2. Pontes R, ed. O universo da ritidoplastia. Rio de Janeiro: Revinter; 2011. 489p.
3. Destro MWB, Destro C, Baroudi R. Pontos de adesão nas ritidoplastias: estudo comparativo. Rev Bras Cir Plást. 2013;28(1):55-8. DOI: http://dx.doi.org/10.1590/S1983-51752013000100010
4. Castro CC, Aboudib JHC, Giaquinto MGC, Moreira MBL. Avaliação sobre resultados tardios em ritidoplastia. Rev Bras Cir Plást. 2005;20(2):124-6.
5. Menezes MVA, Abla LEF, Dutra LB, Junqueira AE, Ferreira LM. Avaliação dos resultados do mini-lifting modificado: estudo prospectivo. Rev Bras Cir Plást. 2010;25(2):285-90.
6. Neves RE, Vasconcellos ZZA, Vasconcellos JJA. Terço médio da ritidoplastia cervicofacial. In: Mélega JM, Baroudi R, eds. Cirurgia plástica fundamentos e arte: cirurgia estética. Rio de Janeiro: Medsi; 2003. p.25-42.
7. Pontes G. Preparo do paciente. In: O universo da ritidoplastia. Rio de Janeiro: Revinter; 2011. p.45-8.
8. D' Assunção EA. Problemas e soluções em ritidoplastia. In: Melega JM, Baroudi R, eds. Cirurgia plástica fundamentos e arte: cirurgia estética. Rio de Janeiro: Medsi; 2003. p.147-65.
9. Melega JM, Baroudi R, eds. Cirurgia plástica fundamentos e arte: cirurgia estética. Rio de Janeiro: Medsi; 2003.
10. Baker TJ, Gordon HL. Complications of rhytidectomy. Plast Reconstr Surg. 1967;40(1):31-9. PMID: 6027664 DOI: http://dx.doi.org/10.1097/00006534-196707000-00004
11. Pitanguy I. La ritidoplastia: soluzione eclética del problema. Minerva Chir. 1967;22(17):942-7.
12. Silva MLA, Aboudib JH, Castro CC. Anatomia aplicada do ramo temporal do nervo facial: estudo do risco potencial de lesão durante a cirurgia do rejuvenescimento facial. Rev Bras Cir Plást. 2010;25(4):604-13. DOI: http://dx.doi.org/10.1590/S1983-51752010000400007
13. Stuzin JM, Baker TJ, Gordon HL. Reoperative rhytidectomy. In: Grotting JC. Reoperative Aesthetic & Reconstructive Plastic Surgery. St Louis: Quality Medical Publishing, 1995. p.205-44.
14. Daher M, Zanini LS. Reconstrução das costeletas. Rev Soc Bras Cir Plást. 1991;14(2):31-6.
15. Knize DM. Periauricular face lift incisions and the auricular anchor. Plast Reconstr Surg. 1999;104(5):1508-20; discussion 1521-3. DOI: http://dx.doi.org/10.1097/00006534-199910000-00043
1. Sociedade Brasileira de Cirurgia Plástica, São Paulo, SP, Brazil
2. Hospital Niterói D'or, Niterói, RJ, Brazil
3. Universidade de Marília, Marília, SP, Brazil
4. Universidade Federal Fluminense, Niterói, RJ, Brazil
Institution: Clínica Fluminense de Cirurgia Plástica/Hospital Niterói D'or - Niterói -RJ e Hospital Universitário de Marília - Marília, SP
Corresponding author:
Getúlio Duarte Junior
Rua Alameda das Quaresmeiras, 248 - Vale do Canãa
Marília, SP, Brazil Zip Code 17525-454
E-mail: getuliojunior@yahoo.com.br
Article received: July 28, 2014.
Article accepted: November 17, 2014.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket