



Original Article - Year 2016 - Volume 31 -
Circumferential suture of the breast with the Brito-Moscozo needle: an alternative suture technique for the breast pillars during mammoplasty
Sutura circunferencial da mama com agulha de Brito-Moscozo: técnica alternativa para sutura dos pilares nas mamoplastias
ABSTRACT
INTRODUCTION: Mammoplasty is one of the most common plastic surgeries in the world. Several techniques have been described for breast volume reduction and mastopexy. For maintaining the conical shape of the breast, breast pillars have been traditionally fixed with sutures from the center of the breast by using commercially available standardized needles. This paper reports an alternative suture technique that uses a Brito-Moscozo needle to create circumferential sutures around the breast pillars during mammoplasty.
METHODS: We describe a circumferential suture technique for the breast pillars and the material used.
RESULTS: From December 2013 to January 2015, 22 cases of reduction mammoplasty and mastopexy were performed with circumferential sutures around the breast pillars. No complications related to the technique were observed.
CONCLUSION: This study verified the applicability of our circumferential suture technique that used a Brito-Moscozo needle to fix the breast pillars. In all the patients who underwent the procedure as an alternative to conventional suture in the center of the breast, fewer sutures and shorter surgical time were required.
Keywords: Mammoplasty; Equipment; Suture techniques; Reconstructive surgical procedures.
RESUMO
INTRODUÇÃO: A mamoplastia é uma das cirurgias plásticas mais realizadas no mundo. Diversas técnicas são descritas para redução do volume mamário e mastopexia. A fixação dos pilares da mama tem sido feita tradicionalmente com suturas a partir do centro da mama, empregando agulhas padronizadas, comercialmente disponíveis, com objetivo de manter a forma cônica da mama. O artigo relata uma técnica alternativa para sutura dos pilares da mama nas mamoplastias, empregando suturas circunferenciais, utilizando a agulha de Brito-Moscozo.
MÉTODO: Foi descrita a técnica de sutura circunferencial dos pilares da mama e material empregado.
RESULTADOS: No período de dezembro de 2013 a janeiro de 2015 foram operados 22 casos de Mamoplastia redutora e mastopexia com sutura circunferencial dos pilares. Não houve complicações relacionadas à técnica empregada.
CONCLUSÃO: Pôde-se constatar a aplicabilidade da sutura circunferencial dos pilares da mama com emprego da agulha de Brito-Moscozo, como alternativa à sutura clássica no centro da mama, em todos os casos operados, com menos uso de suturas e menor tempo cirúrgico.
Palavras-chave: Mamoplastia; Equipamento; Técnicas de sutura; Procedimentos cirúrgicos reconstrutivos.
Mammoplasty continues to be one of the most frequently performed surgeries by plastic surgeons in the world.
Many techniques have been described for breast volume reduction or mastopexy that are aimed at maintaining or providing a conical shape to the breast tissue1-8. Suture of the breast pillars that support the "new" breast is performed from the center of the breast by using standardized and commercially available wires or needles.
OBJECTIVE
The objective of this report was to describe an alternative suture technique for the breast pillars that support the breast, in which circumferential sutures are made by using a Brito-Moscozo needle during mammoplasties. The surgical technique and results are presented herein.
METHODS
From December 2013 to January 2015, 22 female patients underwent reduction mammoplasty or mastopexy, performed by the present author in his private clinic, in which circumferential sutures were made around the breast pillars by using a Brito-Moscozo needle.
Of the 22 patients, 6 underwent mastopexy (resected breast volume, < 100 g) and 16 underwent reduction mammoplasty (> 100 and < 3000 g/breast).
The patients' ages ranged from 22 to 71 years, with a mean of 41 years.
The mean amount of tissue removed was 360 g, ranging from 80 to 2880 g/breast.
The needle used for the suture of the breasts pillars was created on the basis of the Reverdin needles, in which the whole needle pierces the tissue, the suture is introduced at its end, and in a retrograde movement of the needle, the suture passes through the entire path of the needle, capturing the tissue completely. Owing to the conical shape of the breast, a Stocchero circular needle was initially used9,10 for this purpose.
Subsequently, there was a need to create specific needles, called the Brito-Moscozo needles (Figure 1), that adapt to the position of the breast in the chest and the difference in the diameter of the breast base in relation to the apex, providing better ergonomics. Two models were then developed as follows: one needle with a semicircular base of 9 cm to apply the suture at the base of the breast, and another smaller needle, with a semicircular base of 5 cm, to apply the suture in the apex of the breast or in breasts with narrower bases. Both models have a cable at 180º continuous with the needles and a hole in the needle tip for passage of the suture wire.
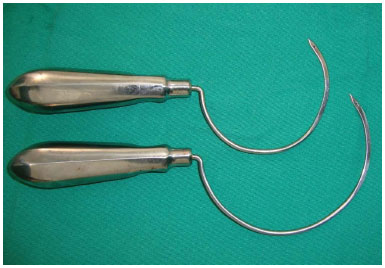
Figure 1. Brito-Moscozo needles, in 2 sizes, for suture of the breast pillars.
Unlike the commercially available needles with predetermined standards that allow the suture of only a part of the breast tissue, the Brito-Moscozo needles feature a semicircular shape that allows the passage of the suture through the entire circumference of the breast.
Technique
The mammoplasty technique adopted in this study used markings with a modified Wise pattern2, made in the orthostatic position, with an inverted-T-shaped final scar. General or epidural anesthesia was used according to the choice of the anesthesia service of the hospital. The dermis was infiltrated with adrenaline and saline (1:500,000). Decortication of the skin, bipartition of the breast, resection of the base and or wedge of breast tissue (in accordance with the need), and maintenance of a Lyacir Ribeiro type I lower pedicle, fixed to the breastplate, in cases that required greater mammary projection were performed.
The breasts were mounted from the suture of the vertical pillars after the passage of the semicircular Brito-Moscozo needle, in a circumferential direction, transversely, entering from the medial, posterior pillar and exiting to the lateral pillar, previously marked with methylene blue (Figures 2 A e B). After passage of the nylon 2.0 suture through the hole of the needle in retrograde movement, the needle was removed, transporting the suture. The pillars were brought together, and a surgical knot was made to project the breast cone (Figures 2 C e D). A second semicircular Brito-Moscozo needle, with a smaller diameter, was passed in the upper part of the pillars by using the same technique, with the same objective (Figures 2 E e F e Figure 3). Suction drains were used in cases of reductive mammoplasty. The procedure was completed with subdermal and intradermal sutures.
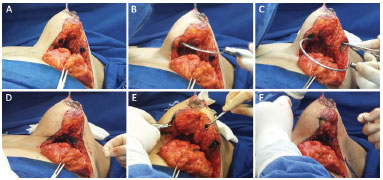
Figure 2. A: Marking of the pillars to be brought together, using methylene blue. Inlet and outlet openings of the Brito-Moscozo needle. B: The needle passing through the medial posterior pillar and exiting from the lateral pillar. C: Passage of the suture through the tip of the needle and retrograde exit of the needle, bringing the suture thread through the entire circumference of the breast. D: Approximation of the pillars and making of the suture knot. E: The smaller-diameter Brito-Moscozo needle passing through the apex of the breast. F: Approximation of the breast pillars superiorly.

Figure 3. Overview of the breasts at the end of surgery.
RESULTS
The patients were followed up postoperatively for at least 6 months (Figures 4-15).
Figure 4. Mastopexy: preoperative appearance.

Figure 5. Mastopexy: appearance after 6 months.

Figure 6. Mastopexy: preoperative appearance (¾).

Figure 7. Mastopexy: appearance after 6 months (¾).

Figure 8. Mastopexy: preoperative profile.

Figure 9. Mastopexy: profile after 6 months.

Figure 10. Reduction mammoplasty: preoperative appearance.

Figure 11. Reduction mammoplasty - postoperative 6 months.

Figure 12. Reduction mammoplasty: preoperative appearance (¾).

Figure 13. Reduction mammoplasty: appearance after 6 months (¾).

Figure 14. Reduction mammoplasty: preoperative profile.

Figure 15. Reduction mammoplasty: profile after 6 months.
The use of circumferential sutures for the breast was possible with the Brito-Moscozo needle, regardless of breast characteristics, in all the 22 patients who underwent the procedure.
In 2 patients, dehiscence occurred approximately 2 cm from the dermal sutures in the vertical scars, which healed by second intention.
In one case, a granulomatous reaction to the foreign body due to the use of polyglecaprone in the subdermal suture of the areola was observed, necessitating the withdrawal of sutures in the clinic, with healing by second intention.
No complications related to the use of the Brito-Moscozo needle and circumferential suture that affected the shape and projection of the breasts were observed during follow-up.
As only 2 or 3 sutures were used to mount the breast cone, the surgical time for suturing of the breast pillars was shortened.
DISCUSSION
The choice of a mammoplasty technique may vary depending on breast volume and size, degree of ptosis, glandular or fatty composition of the breast, type of final scar desired, surgeon experience, and so on.
Regardless of the chosen method, the use of special techniques and instruments aims to maintain the conical shape of the breast and for as long as possible.
The circumferential suture technique that uses the Brito-Moscozo needle to fix the breast pillars that support the breast, involving the entire breast cone, from its base to the apex, facilitates mounting of the breasts and allows the complete fixation of the breast pillars. The technique is applicable in the most varied types of breast tissue, mainly in fatty and large breasts, which are known to be difficult to suture and project.
Some authors have sought alternatives such as a biocompatible mesh to replace the function of the suspension ligaments of the breast. In general, meshes are used in periareolar mammoplasty, with concepts of remodeling the gland independently of the skin and/or provide circumferential support to the breast in its most external part11-13. The use of circumferential needles is based on the concept of fixing the circular shape of the breast, without separating the gland from the skin.
The use of the Brito-Moscozo needle in suturing the pillars and in maintaining the conical shape of the breast decreased the number of sutures needed to sustain the pillars at the time of surgery.
In the present study, nylon 2.0 was used in all the cases. The use of the Brito-Moscozo needle allows the use of sutures of different brands, diameters, and compositions. The surgeon has a wider choice of sutures to be used, being not restricted to the standardization of a certain manufacturer or hospital. Polypropylene or even absorbable sutures such as those derived from polyglactin and polidioxanone may eventually be accepted as substitutes to the commonly used nylon. Similarly, the use of circumferential needles opens the possibility of using barbed sutures to sustain the mammary gland. However, this requires studies about its use in these cases.
Comparative studies are necessary to define whether results differ between the suture of the breast pillars from the center and that from the circumference of the breast, or even the combination of these 2 techniques in the maintenance of the shape and projection of the breast cone.
CONCLUSION
The authors propose the use of circumferential sutures with the Brito-Moscozo needle for fixing the breast pillars, as an alternative to the conventional suture, which is performed at the center of the breast, during mammoplasty.
REFERENCES
1. Skoog T. A technique of breast reduction; transposition of the nipple on a cutaneous vascular pedicle. Acta Chir Scand. 1963;126:453-65. PMID: 14072329
2. Wise RJ, Gannon JP, Hill JR. Further experience with reduction mammoplasty. Plast Reconstr Surg. 1963;32:12-20.
3. Ribeiro L. A new technique for reduction mammaplasty. Plast Reconstr Surg. 1975;55(3):330-4. DOI: http://dx.doi.org/10.1097/00006534-197555030-00010
4. Pitanguy I. Surgical treatment of breast hypertrophy. Br J Plast Surg. 1967;20(1):78-85. DOI: http://dx.doi.org/10.1016/S0007-1226(67)80009-2
5. Peixoto G. Reduction mammaplasty: a personal technique. Plast Reconstr Surg. 1980;65(2):217-26. DOI: http://dx.doi.org/10.1097/00006534-198002000-00015
6. Bozola AR. Breast reduction with short L scar. Plast Reconstr Surg. 1990;85(5):728-38. DOI: http://dx.doi.org/10.1097/00006534-199005000-00013
7. Benelli L. A new periareolar mammaplasty: the "round block" technique. Aesthetic Plast Surg. 1990;14(2):93-100. DOI: http://dx.doi.org/10.1007/BF01578332
8. Sperli AE. Mammaplasty utilizing the crossed flap technique. A critical analysis of 23 years experience. Rev Soc Bras Cir Plást. 1994;9(2):34-44.
9. Stocchero IN. The roundblock SMAS treatment. Plast Reconstr Surg. 2001;107(7):1921-3. DOI: http://dx.doi.org/10.1097/00006534-200106000-00064
10. Stocchero I. Shortscar face-lift with the RoundBlock SMAS treatment: a younger face for all. Aesthetic Plast Surg. 2007;31(3):275-8. DOI: http://dx.doi.org/10.1007/s00266-006-0197-2
11. Góes JC. Periareolar mammaplasty: double skin technique with application of polyglactine or mixed mesh. Plast Reconstr Surg. 1996;97(5):959-68.
12. Sampaio Góes JC. Periareolar mammaplasty: double-skin technique with application of mesh support. Clin Plast Surg. 2002;29(3):349-64. DOI: http://dx.doi.org/10.1016/S0094-1298(02)00005-6
13. van Deventer PV, Graewe FR, Würinger E. Improving the longevity and results of mastopexy and breast reduction procedures: reconstructing an internal breast support system with biocompatible mesh to replace the supporting function of the ligamentous suspension. Aesthetic Plast Surg. 2012;36(3):578-89. DOI: http://dx.doi.org/10.1007/s00266-011-9845-2
1. Sociedade Brasileira de Cirurgia Plástica, São Paulos, SP, Brazil
2. Aesthetics Centro de Cirurgia Plástica Feira de Santana, Bahia, Brazil
3. Hospital São Rafael, Salvador, BA, Brazil
Institution: Aesthetics Centro de Cirurgia Plástica Feira de Santana, Bahia, Brazil
Corresponding author:
Francisco Aníbal Passos de Brito
Av. Getúlio Vargas, 968, Centro, Feira de Santana
Bahia, BA, Brazil, Zip Code 44001-496
E-mail: drfranciscoanibal@gmail.com
Article received: May 30, 2015.
Article accepted: November 20, 2015.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket