



Articles - Year 2004 - Volume 19 -
Retrospective Study of 730 Patients Submitted to Reduction Mammaplasty
Estudo Retrospectivo de 730 Pacientes Submetidas a Mamaplastia Redutora
ABSTRACT
The authors present the studies and results obtained after the assessment of 730 cases operated on for breast hypertrophy, from January 1995 to December 2001, at Hospital Universitário Pedro Ernesto (HUPE). The patients and the surgical technique are analyzed in their most significant details, stressing the care necessary in well conducted preoperative clinical evaluatum, surgery and postoperative care, to attain satisfactory results and natural shaped breasts, maintenance of lactation function and areolomamillary sensitivity, with subtle or non-apparent scars.
Keywords: Breast hypertrophy; breast ptosis; treatment; reduction mammaplasty; patient satisfaction
RESUMO
Os autores apresentam os estudos e resultados obtidos após a avaliação de 730 casos operados de hipertrofia mamária, no período de janeiro de 1995 a dezembro de 2001, no Hospital Universitário Pedro Ernesto (HUPE). As pacientes e a técnica cirúrgica são analisadas em seus mais importantes detalhes, ressaltando os cuidados necessários na avaliação clínica pré-operatória, ato cirúrgico e pós-operatório bem conduzidos, para que os resultados sejam satisfatórios, obtendo mamas de formato natural, manutenção da função de lactação e sensibilidade areolomamilar, obtenção de cicatrizes discretas ou imperceptíveis.
Palavras-chave: Hipertrofia mamária; ptose mamária; tratamento; mamaplastia redutora; satisfação da paciente
The majority of patients at the plastic surgery outpatient service of Hospital Universitário Pedro Ernesto seek reduction mammaplasty, and between 10 and 15 surgeries are performed per month. Patients want to reduce breast size for physical or psychological reasons.
The cult of physical fitness, promoted by the media, and the association between physical beauty and suecess in a person's professional life, social life, and love life have led to an increase in requests for aesthetically motivated surgery.
Patients complain of physical discomfort due to the weight of breasts, backaches, weight on shoulders, and also other situations such as: incorrect-posture, such as kyphosis and lumbar lordosis, grooves or marks on the shoulders due to brassiere straps and dermatitis in the sub mammary groove region, all representing functional alterations. Plastic surgery should correct breast hypertrophy, the causal agent of these deformities.
During the examination of the breasts the inspection is carried out with the patient standing or seated, to assesthe degree of hypertrophy and breast ptosis, symmetry, quality of skin alterations (scars and striae), color and shape of the areolomamillary complex (AMC), nipples (everted, even, inverted, hypertrophic), medial junction of infra mammary grooves, content-container relationship. During palpation, consistency (glandular, mixed, fatty), sensitivity, presence or absence of breast tumors, axillary lymph nodes and nipple discharge upon expression should be assessed. Measurements from the sternal furcula to the nipples, and the intermamillary distance should be taken.
Hypertrophies may be accompanied by breast ptosis, as classified by Binet(1), in 4 (four) grades:
Grade I - lower border of the breast, up to 2 cm from the infra mammary groove.
Grade II - lower border of the breast more than 2 cm from the infra mammary groove, but does not exceed the rib cage.
Grade III - lower border of the breast between the rib cage and the umbilicus.
Grade IV - lower border of the breast, below the umbilicus.
The morphology of the breast in proportion to the patient's chest, size and weight should be assessed and the importance of breast irrigation and innervation should be acknowledged. Vascular anastomoses are abundant, especially at the level of the AMC. The sensitivity of the areolomamillary region is noteworthy, mainly due to the lateral cutaneous branch of the 4th intercostal nerve.
Regarding consistency, Galtier(1) classified breasts histologically into:
a) Pure glandular hypertrophy of puberty or real.
b) Mixed glandular hypertrophy (glandular and fat), found mainly after pregnancy and breastfeeding.
c) Pure or false fat hypertrophy, found in premenopausal or elderly patients.
The reduction mammaplasty technique adopted in our service follows the marking created by Pitanguy(2), modified by curved incisions according to Castro's description(1). The breast tissue is resected in the elassical form, according to the technique of Pitanguy(2) with a keel-shaped resection ar modified with a flat resection, the Pontes variant I(3). Breast tissue contouring is performed along with the skin, without detaching it.
Postoperative dressing is kept with micro pore adhesive replaced every seven days. After 24 postoperative hours the cotton bedded elastic dressing is removed and replaced by the post-surgical brassiere, and the patient is discharged. Suture resting will result in more subtle scars.
Mammaplasties may basically present the following complications: hematomas, dehiscenses, infections, necroses, asymmetries and non-aesthetic scars that generally bother the surgeon more than the patient. Some prophylactic measures may be taken to avoid them, such as: utilization of a suitable technique, absence of suture tension, less skin tissue trauma.

Fig. 1 - Marking recommended by Pitanguy and modified by Castro in curved incisions (left); keel-shaped resection of the lower pole (right).
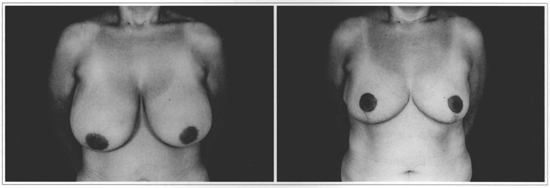
Figs. 2a & 2b - Front view of a 26 year-old patient during pre and postoperative of four years.
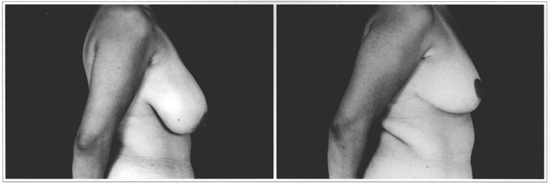
Figs. 2c & 2d - Side view of patient in which 560g of the right breast and 460g of the left breast were resected.
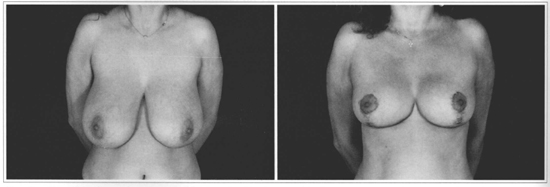
Figs. 3a & 3b - Front view of a 41 year-old patient in pre and postoperative of one year.
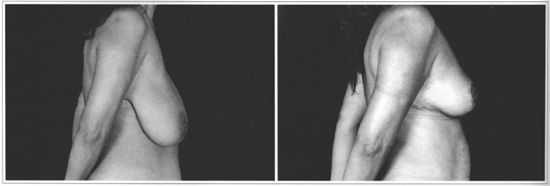
Figs. 3c & 3d - Side view of a patient in whom 770 g of the right breast and 750 g of the left breast were resected.
OBJECTIVE
The objective of the present study was to certify the high applicability of the surgical technique of Pitanguy(2) and its modifications, to attain satisfactory results in the various types of presentation of breast hypertrophy, given that mammaplasties are performed by third year plastic surgery residents, assisted and supervised by teams and residents of Hospital Universitário Pedro Ernesto. A large part of our patients have macromastia, and large resections are performed in order to attain an agreeable shape. The proportion of cases in which more than 1,000 g of breast tissue is resected comes to 31%. Immediate and late complications are analyzed, and the final result is not compromised, given the high levels of satisfaction in 85% of cases.
METHODS
We performed a retrospective study of 730 patients, submitted to breast reduction from January 1995 to December 2001, evaluating patients as to age (Fig.4), shape, consistency, symmetry and degree of ptosis of breasts operated on by the Pitanguy technique(2). We also analyzed the amount of breast tissue resected, level of patient satisfaction, objective evaluation, and immediate and late complications.

Fig. 4 - Distribution of reduction mammaplasties by age group.
RESULTS
The analysis revealed that 63% of patients were in the 20 to 40 year-old age group (Fig. 4), 70% of the breasts were of mixed texture, and 34% had some degree of asymmetry. The classical Pitanguy techniquew with keel-shaped resection of breast tissue was performed in 25% of cases, and a flat resection was performed in 75% of patients. The mean of resected tissue in the study was 800 g per patient (Fig. 5). Immediate adverse events occurred in 14% of cases, and were mainly subtle dehiscence in the inverted "T" region and hematomas, with satisfactory outcome. Late complications or sequelae were observed in 16% of cases, encompassing alterations in sensitivity and positioning of AMC and breast asymmetry. Patients reported high levels of satisfaction (Fig. 6), with 85% of good and excellent scores.

Fig. 5 - Amount of breast tissue resected by patient.

Fig. 6 - Level of patient satisfaction.
CONCLUSION
Whether for functional reasons or not, patients who request mammaplasty always desire the best aesthetical results. Mammaplasry is about changing breasts that the patient does not like for breasts with excellent shape, aspect and texture, but with scars, generally of good quality, when the surgery is performed well. The surgical technique proposed by Pitanguy(2) is easy to perform and standardize, and similar results can be reached by different surgeons, even if in training, and is quite applicable to the various breast types and shapes.
REFERENCES
1. Castro CC, Melki LAH. Aspectos atuais do tratamento das hipertrofias e ptoses mamárias. J Bras Gin. 1977; 83:241-57.
2. Pitanguy I. Mamoplastia: estudo de 245 casos consecutivos e apresentação de técnica pessoal. Rev Bras Cir. 1961; 42:201-20.
3. Pontes R. Reduction mammaplasty - Variations I and II. Ann Plast Surg. 1981; 6:437-44.
4. Castro CC. Mamaplastia redutora nas hipertrofias mamárias. Rev Col Bras Ciro 1975; 2:134-7.
5. Castro CC. The value of non-prefixed marking in reduction mammaplasty Aesth Plast Surg. 1984; 8:237-41.
6. Georgiade G, Georgiade GS, Riefkoh R. Esthetic breast surgery: In: McCarthy JG Plastic Surgery Philadelphia: WB Saunders Company; 1990. p. 3839-97.
7. Keppke EM, Matta S. Plásticas de redução mamária. In: Mélega JM, Zanini AS, Psillakis JM. Cirurgia plástica reparadora e estética. 2.ed. Rio de Janeiro. MEDSI; 1992. p. 707-24.
8. Pitanguy I. Evaluation of body contouring surgery today: a 30-year experience. Plast Reconstr Surg. 2000; 105:1499-514.
9. Schwartzmann E. Die tecnik der Mammaplastik. Chirurg. 1930; 2:932-43.
10. Spear SL, Little JW. Reduction mammoplasthy and mastopexy. In: Grabb W & Smith JW Plastic Surgery. 5.ed. Philadelphia: Lippincott-Raven; 1997. p. 725-55.
11. Strombeck JO. Mammaplasty. In: Grabb W & Smith JW Plastic Surgery. 5. ed. 1997; p. 726-8.
I - Candidate Member to the Brazilian Society of Plastic Surgery; Medical Resident of the Discipline of Plastic Surgery of Hospital Universitário Pedro Ernesto - UERJ.
II - Assistant Professor of the Discipline of Plastic Surgery of Hospital Universitário Pedro Ernesto - UERJ. MSc in Plastic surgery Member of the SBCP.
III - Associate Professor and Head of the Plastic Surgery Service of Rio de Janeiro State University Hospital Pedro Ernesto. Member of the SBCP.
Study performed at Hospital Universitário Pedro Ernesto - Universidade do Estado do Rio de Janeiro, RJ
Address for correspondence:
Rodrigo Corteletti Ronconi, MD
Av. 28 de Setembro, 77
20550-030 - Rio de Janeiro - RJ Brazil
Phone/fax: (55 21) 2587-6675
e-mail: mrcronconi@ig.com.br
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket