



Review Article - Year 2015 - Volume 30 -
Nutritional considerations for plastic surgery in post-bariatric surgery patients
Considerações nutricionais para cirurgia plástica em paciente após cirurgia bariátrica
ABSTRACT
Bariatric surgery continues to be the most effective treatment for morbid obesity and most other associated metabolic conditions such as type 2 diabetes mellitus, gastroesophageal reflux disease, and obstructive sleep apnea. In the obese population, common nutritional deficiencies include vitamins A, C, D, and B12, folate, thiamine, iron, ferritin, zinc, and selenium. With massive weight loss, many patients may utilize body contouring for deformities. After massive weight loss following bariatric surgery, patients often develop significant nutritional deficiencies that increase the risk of postoperative morbidity and mortality with any subsequent surgeries. Some unique patients will require additional evaluation during illness or when considering elective surgery due to alterations to the alimentary tract, in order to optimize outcomes and prevent complications from nutritional deficiencies.
Keywords: Nutrition; Deficiency diseases; Bariatric surgery; Drug-Related side effects and Adverse reactions.
RESUMO
A cirurgia bariátrica continua a ser o tratamento mais efetivo para obesidade mórbida e a mais associada a outras condições metabólicas tais como diabetes tipo 2, doença refluxo gastroesofágico, e apneia do sono obstrutiva. Na população obesa, deficiências nutricionais comuns incluem vitaminas A, C, D, e B12, folato, tiamina, ferro, ferritina, zinco e selênio. Com a perda de peso ponderal, muitos pacientes podem utilizar o contorno corporal para deformidades. Após perda de peso ponderal seguida de cirurgia bariátrica, os pacientes geralmente desenvolvem deficiência nutricional significante que aumenta o risco de morbidade e mortalidade pós-operatória com quaisquer cirurgias subsequentes. Alguns pacientes requererem avaliação adicional durante a doença, ou quando candidatos eletivos pré-cirurgia, devido a alterações no trato alimentar com objetivo de melhorar os resultados e prevenir complicações devido a deficiências nutricionais.
Palavras-chave: Nutrição; Deficiências Nutricionais; Cirurgia Bariátrica; feitos Colaterais e Reações Adversas Relacionados a Medicamentos.
The World Health Organization (WHO) reported in 2008 that over 200 million men and 300 million women were obese worldwide. A disease no longer limited to industrialized countries, overweight obesity kills more people than underweight in over 65% of the world1,2. Obesity has been associated with increased hazard ratio of all-cause mortality as well as significant medical and psychological comorbidity. Obesity is a chronic medical condition that should be regarded as a disease state. Although the number of bariatric surgical procedures has plateaued in the United States, the rates of severe obesity continue to rise. Approximately 15 million people in the United States have a body mass index (BMI) of > 40 kg/m2. Only 1% of this eligible population receives surgical treatment2.
After massive weight loss, the majority of patients, are left with loose or redundant skin that may cause pain, fungal infections, and problems with personal hygiene, and affect posture and mobility. Plastic surgery is the most common procedure following weight loss surgery1. Nearly 60,000 body contouring procedures were performed in 20083,4. The reported number of patients undergoing body contouring surgery after massive weight loss varies from 12% to 44%5. This number is inversely proportional to the time interval between bariatric and plastic surgery5. These body contouring procedures have the potential for significant postoperative morbidity and mortality. Wound healing complications are very common after body contouring surgery, with reports varying anywhere from 8% to 66% in the massive weight loss population. Complications include seroma, wound infection, wound dehiscence, flap necrosis, delayed healing, lymphoceles/lymphorrhea, asymmetry, and thrombosis4,6-8. Optimization of the nutritional state plays a key role in reducing these complications. This article reviews the current knowledge of nutritional deficiencies in the morbidly obese and following weight loss surgeries. We present a summary review for screening deficiencies and recommending supplements for optimal surgical outcome to reduce complications in this patient population.
METHODS
An extensive literature review using MEDLINE and PUBMED for abstracts from the years 2008-2013, with a focus on reviews, primary research, and case studies with additional searches in Surgery for Obesity and Related Disease, Journal of Clinical Endocrinology and Metabolism, and in an approved article reference list using the key words: bariatric surgery, plastic surgery, nutrition deficiencies, massive weight loss, and wound complications was performed. We identified 125 articles and 1 poster presentation; of these, 50 full articles were reviewed, and 28 articles were selected, along with selected practice references from the American Association of Clinical Endocrinologists, the Obesity Society, and the American Society for Metabolic and Bariatric Surgery Medical Guidelines for Clinical Practice for the Perioperative Nutritional, Metabolic, and Nonsurgical Support of the Bariatric Surgery Patient.
Mechanisms Contributing to Nutritional Deficiencies in Obesity and After Bariatric Surgery
After significant weight loss following weight loss surgery, patients may meet the candidacy requirements for other elective procedures such as orthopedic back, hip, or knee procedures, hernia repair, or body contouring surgery that might have been denied to them prior to weight loss because of extenuating operative risk.
A comprehensive pre-operative evaluation is mandatory before any elective surgery following massive weight loss, with emphasis on weight loss history, type of bariatric procedure, diet, exercise habits, residual medical problems, physical examination, and laboratory studies. Malnutrition profoundly increases the risk for postoperative complications. Elective body contouring surgery is not recommended in the active weight loss phase that may last up to18 months from weight loss surgery, to decrease the risk for significant postoperative complications and obtain more satisfactory cosmetic outcomes2,9,10. Additionally, it is advisable to have a weight plateau phase of at least 3 months, during which these nutritional deficiencies may be identified and optimized before the elective surgery.
Obesity, long considered a state of over-nutrition, has been found to be a state of malnourishment of vital macro- and micro-nutrients. The cause of this paradoxical problem is likely secondary to consumption of high calorie processed foods associated with poor nutritional quality that are relatively inexpensive and readily available in abundance2,9,11. The extent of the macro- and micronutrient deficiencies is dependent on the type of bariatric surgery. The incidence of deficiencies, laboratory tests, and incidence following metabolic-bariatric surgery can be found in Chart 1. Understanding these procedures helps to anticipate and correct the major nutritional deficiencies that may be one might encountered when dealing with patients who have undergone massive weight loss.

Surgical weight loss procedures fall into three categories: purely restrictive, mal-absorptive, and a combination of both. The vertical banded gastroplasty (VBG), adjustable gastric band (AGB) (Figure 1), and sleeve gastrectomy (SG) (Figure 2) are purely restrictive in nature. The Roux-en-Y gastric bypass (RYGB) (Figure 3), bilio-pancreatic diversion (BPD), and bilio-pancreatic diversion with duodenal switch (BPD-DS) (Figure 4) cause weight loss by a combination of restriction and malabsorption. The jejunal-ileal bypass (JIB), which involves bypassing the majority of the small intestine, has been completely abandoned because of serious and significant metabolic and nutritional complications. The degree of nutritional deficiencies depends on the bypassed portion of the small intestine, which is higher in the BPD and BPD-DS compared to the RYGB (Figure 5).

Figure 1. Adjustable Gastric Band in body.

Figure 2. Vertical Sleeve Gastrectomy.

Figure 3. Roux-en-Y Gastric Bypass.

Figure 4. Bilio-Pancreatic Diversion with Duodenal Switch.
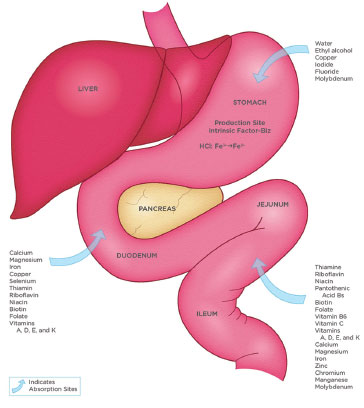
Figure 5. Schematic representation of absorption of various nutrients in the gastrointestinal.
Nutritional deficiencies in purely restrictive procedures are most commonly related to restricted intake, especially in the early postoperative period. This is sometimes exacerbated by postoperative nausea and vomiting. Gastric restriction in the SG and resectional gastric bypass reduce mechanical digestion and acid secretion, which impairs both the digestion and absorption of vitamin B12, iron, and other protein-bound nutrients, as well as secretion of intrinsic factor, which is vital for absorption of vitamin B12. Pre-operative obese adults are found to have lower levels of vitamin B12, folate, thiamine, vitamins A, C, and D, iron, magnesium, ferritin, zinc, folate, and selenium2,6,8,11-13. Extremely obese patients have the additional potential to develop vitamin B12 and vitamin E deficiencies, as many take acid reducers for reflux treatment or metformin for diabetes management, which may induce B12 and magnesium deficiencies2,8,9,11,12. Surgical treatment of severe obesity may exacerbate pre-existing protein, vitamin, and mineral deficiencies or produce new ones, depending on dietary intake, adherence to recommended post-bariatric surgery supplements, and the degree of malabsorption associated with the type of bariatric surgery.
Protein
Up to 25% of weight loss surgery patients are at risk of developing protein calorie malnutrition. Protein deficiency impairs wound healing, because protein is needed for fibroblast proliferation, angiogenesis, and collagen production4,14. Obesity is a pro-inflammatory state with increased levels of tumor necrosis factor alpha, and obese patients have increased risk for wound complications secondary to immunosuppression. Although the reasons for abnormal wound healing and postoperative complications are multi-factorial, nutrition plays a key role in the healing process. Patients who undergo weight loss surgery are routinely recommended to eat a high protein diet with at least 60 to 80 gm/day, or 1.5 grams of protein per kilogram of ideal body weight to prevent the loss of lean body mass. The added catabolic stress of a major body contouring surgery can potentially push a marginally nourished patient into a malnourished state2,11. The nutritional deficiency is secondary to low food intake, food intolerance secondary to micro-nutrient deficiency such as thiamine that causes nausea and vomiting, dumping syndrome, and the extent of malabsorption, depending on the type of weight loss surgery. Albumin, pre-albumin, and protein intake logs are valid measures to assess the pre-operative nutritional state8,9,14.
Anemia
Iron deficiency anemia is the earliest and most common deficiency after weight loss surgery, occurring in 12%-47% of patients after weight loss surgery, particularly after procedures resulting in malabsorption2,5,9-14. The deficiency can also have multi-factorial causes such as, impaired iron absorption, decreased iron intake, and potentially bleeding lesions such as in gastritis, esophagitis, and marginal ulcers. Menstruating and pregnant females are at a greater risk of iron deficiency anemia. Iron supplements of 40-200 mg elemental units per day with vitamin C to enhance absorption are recommended after bariatric surgery2,3,5,9. Some patients who are refractory to oral therapy may require parenteral iron or blood transfusions11.
Calcium and Vitamin D
Vitamin D deficiency may contribute to dysfunction of the innate immune system, which in turn increases the risk of wound infection and complications following surgery. Morbidly obese patients are at increased risk for vitamin D and calcium deficiencies, possibly because of decreased dietary intake of dairy products, a sedentary life-style, reduced exposure to bright sunlight, as well as increased sequestration of lipid-soluble vitamin in adipose tissue stores. The most common source of vitamin D is ultraviolet light exposure, with less than 10% coming from dietary intake. The recommended calcium dose is 1200-1500 mg in divided doses, along with 3000 IU of vitamin D2,3,5,9.
Other Fat Soluble Vitamins-A, E, and K
Vitamin A and E have antioxidant properties and play a strong role in wound healing. Although not recommended to be taken as a separate supplement, the intake of adult multivitamins twice daily should be adequate to avoid deficiency of these two vitamins. Excess supplementation of vitamin E can inhibit collagen synthesis and decrease the tensile strength of wounds. Vitamin K deficiency is rare, except in severe malabsorption that can be associated with BPD or BPD-DS, and can lead to increased risk of bruising or blood loss during surgery2,11.
Vitamin B1, B12, B6, and Folate
B complex vitamins are very important for neurological and hematological functions. Thiamine deficiency can exacerbate nausea, which could in turn potentiate other nutritional deficiencies. Severe thiamine deficiency should be treated with intravenous thiamine 500 mg for 3 to 5 days, followed by 250 mg for 3 to 5 days, then orally 100 mg per day indefinitely. Oral supplementation with crystalline B12 1000 mcg per day, intranasal 500 mcg per week, or 1000 mcg per month intramuscularly to maintain normal vitamin B12 levels is recommended. Folic acid supplementation can be accomplished through a mineral containing multivitamin with 400 mg per day. Increased supplementation is recommended in pregnant women and those in their child-bearing years. Multivitamin supplements that contain B2 and B6 should be sufficient to support normal levels2,13.
Vitamin C, Zinc, Copper, Selenium
Vitamin C has powerful anti-oxidant and anti-inflammatory properties that can improve neutrophil function and enhance angiogenesis. Vitamin C increases non-heme iron absorption, and plays an important role in wound healing. It is an essential co-factor in the synthesis of collagen, proteoglycans, and other components of the intracellular matrix such as bones, skin, capillaries, and other connective tissues. Deficiency leads to impaired wound healing due to the production of abnormal collagen fibers as well as changes in the intracellular matrix and poor adhesion of endothelial cells and fibrous tissues. Vitamin C is important for hydroxylation of proline and lysine residues that converts pro-collagen to collagen, which is essential for collagen stabilization. Supplementation with 1 to 2 grams of vitamin C is recommended for patients with injuries or surgery until healing is complete5.
Zinc is essential in all stages of cell repair and healing and plays an important role in supporting the immune system. Severe malabsorption states associated with diarrhea can lead to significant zinc deficiency. In bariatric surgery patients preparing for body contouring surgery, a daily supplement of 40 mg is recommended5,9. Selenium also plays an important role in muscle metabolism and immune regulation14. Selenium deficiency can lead to secondary iron malabsorption deficiency. Although not routinely screened, deficiency of the micronutrients zinc and copper can also lead to anemia. This should be considered in cases of anemia which resist routine treatment2,3.
The aggressiveness of nutrition supplementation depends on the extent of malabsorption created by the weight loss surgery. During the equilibrium state, finite supplements may be sufficient; however, the stress of surgery may require a temporary increase in supplementation. Wound healing complications as high as 8%-66% have been reported in the literature in the massive weight loss population8. Commercial dietary formulations for post-bariatric patients scheduled for body contour surgery have been developed as a complement to a commercial brand bariatric supplement. These formula supplements provide approximately 90 grams of protein and amino acids, in addition to vitamins at levels indicated for wound healing. This supplement taken daily for 3 weeks prior to surgery significantly decreased complications from 66% to 18.9% and also accelerated wound healing14.
The degree of deficiency of any of these nutrients is dependent on nutritional practice guidelines of the specific bariatric program, adherence to the recommended supplements, and regular patient evaluation and follow-up after weight loss surgery. After bariatric surgery, additional preoperative evaluations should include a detailed history, as well as clinical and laboratory evaluations with pretreatment of nutritional abnormalities.
CONCLUSION
Prior to elective procedures such as abdominal contouring, nutritional assessment may include clinical and biochemical analysis of protein, micronutrients, and minerals to optimize patient safety and decrease the risk for wound complications. Extensive preoperative testing may not be cost effective, but should include complete blood count, electrolytes, albumin, pre-albumin, and transferrin, which are often sufficient with clinical correlation. Alternatively, a cost effective nutritional evaluation by a registered dietitian may be beneficial for protein and micronutrient deficiency risk prevention peri-operatively. We routinely recommend the following to all bariatric surgery patients in our practice: a daily minimum of 60 grams protein, two adult multi-vitamins with iron and 350 mcg B12, 1500 mg calcium/800 IU vitamin D. Our suggestions for nutritional optimization can be found in Table 1 and the ASMBS recommendations in Table 2. Other micro-nutrition is treated based on symptoms. Patients are scheduled for regular follow up for assessment and treatment of deficiencies. Our program recommendations are akin to those put forward in the 2013 American Society for Metabolic and Bariatric Surgery nutritional guidelines. Patients who have undergone bariatric surgery should have an annual chemistry and clinical evaluation for common deficiencies related to the specific modification to the alimentary system on record. Regular follow-up and annual screening of all post-weight loss surgery patients helps encourage them, reminds them to take the recommended supplements, and avoids having a nutritionally-depleted patient who is then at high risk for complications. High-risk patients should have a low threshold for referral back to the Metabolic and Bariatric services for nutritional optimization preoperatively.


Limitations of this review include various ranges of the lesser-supplemented nutrients and minerals. More randomized studies are needed to further the understanding of the supplementation needs of these patients after massive weight loss.
REFERENCES
1. World Health Organization (WHO) 2013. Overweight and obesity. Factsheet Nº311 [Accessed October, 3 2013]. Available at: http://www.who.int/mediacentre/factsheets/fs311/en/index.html
2. Mechanick JI, Youdim A, Jones DB, Timothy Garvey W, Hurley DL, Molly McMahon M, et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient--2013 update: cosponsored by American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic & Bariatric Surgery. Surg Obes Relat Dis. 2013;9(2):159-91. DOI: http://dx.doi.org/10.1016/j.soard.2012.12.010
3. Allied Health Sciences Section Ad Hoc Nutrition Committee; Aills L, Blankenship J, Buffington C, Furtado M, Parrott J. ASMBS Allied Health Nutritional Guidelines for the Surgical Weight Loss Patient. Surg Obes Relat Dis. 2008;4(5 Suppl):S73-108. DOI: http://dx.doi.org/10.1016/j.soard.2008.03.002
4. Naghshineh N, O'Brien Coon D, McTigue K, Courcoulas AP, Fernstrom M, Rubin JP. Nutritional assessment of bariatric surgery patients presenting for plastic surgery: a prospective analysis. Plast Reconstr Surg 2010;126(2):602-10. DOI: http://dx.doi.org/10.1097/PRS.0b013e3181de2473
5. Faria SL, Faria OP, Careeal MA, Gouvêa HR. Nutritional management related to plastic surgery among bariatric patients: a meta-analysis. Bariatric Times. 2012;9(8):14-9.
6. Davison SP, Clemens MW. Safety first: precautions for the massive weight loss patient. Clin Plast Surg. 2008;35(1):173-83. PMID: 18061812 DOI: http://dx.doi.org/10.1016/j.cps.2007.08.002
7. Shrivastava P, Aggarwal A, Khazanchi RK. Body contouring surgery in a massive weight loss patient: An overview. Indian J Plast Surg. 2008;41(Suppl):S114-29.
8. Albino FP, Koltz PF, Gusenoff JA. A comparative analysis and systematic review of the wound-healing milieu: implications for body contouring after massive weight loss. Plast Reconstr Surg. 2009;124(5):1675-82. PMID: 20009855 DOI: http://dx.doi.org/10.1097/PRS.0b013e3181b98bb4
9. Xanthakos SA. Nutritional deficiencies in obesity and after bariatric surgery. Pediatr Clin North Am. 2009;56(5):1105-21. DOI: http://dx.doi.org/10.1016/j.pcl.2009.07.002
10. Colwell AS, Borud LJ. Optimization of patient safety in postbariatric body contouring: a current review. Aesthet Surg J. 2008;28(4):437-42. DOI: http://dx.doi.org/10.1016/j.asj.2008.04.007
11. Mechanick JI, Kushner RF, Sugerman HJ, Gonzalez-Campoy JM, Collazo-Clavell ML, Guven S, et al. American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic & Bariatric Surgery Medical Guidelines for Clinical Practice for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient. Surg Obes Relat Dis. 2008;4(5 Suppl):S109-84. DOI: http://dx.doi.org/10.4158/EP.14.S1.1
12. Heber D, Greenway FL, Kaplan LM, Livingston E, Salvador J, Still C; Endocrine Society. Endocrine and nutritional management of the post-bariatric surgery patient: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2010;95(11):4823 43. DOI: http://dx.doi.org/10.1210/jc.2009-2128
13. Fullmer MA, Abrams SH, Hrovat K, Mooney L, Scheimann AO, Hillman JB, et al.; National Association of Children's Hospitals and Related Institutions; North American Society of Pediatric Gastroenterology, Hepatology, and Nutrition. Nutritional strategy for adolescents undergoing bariatric surgery: report of a working group of the Nutrition Committee of NASPGHAN/NACHRI. J Pediatr Gastroenterol Nutr. 2012;54(1):125-35. DOI: http://dx.doi.org/10.1097/MPG.0b013e318231db79
14. Agha-Mohammadai S, Hurwitz DJ. Potential impacts of nutritional deficiency of postbariatric patients on body contouring surgery. Plast Reconstr Surg. 2008;122(6):1901 14. DOI: http://dx.doi.org/10.1097/PRS.0b013e31818d20d6
Marshfield Clinic, Marshfield, WI, USA
Institution: Program for Metabolic & Bariatric Surgery., Marshfield, WI, USA.
Corresponding author:
Vijaya L. Nirujogi
1000 North Oak Ave, Marshfield
WI, USA 54449
E-mail: nirujogi.vijaya@marshfieldclinic.org
Article received: January 20, 2014.
Article accepted: March 4, 2014.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket