



Original Article - Year 2015 - Volume 30 -
Aesthetic evaluation and therapeutic procedures related to main facial profiles
Avaliação estética e condutas terapêuticas relacionadas aos principais perfis faciais
ABSTRACT
INTRODUCTION: Orthognathic surgery for correction of dentofacial deformities provides a more-symmetrical face, and functional and aesthetic benefits. The aim of this study was to evaluate the perception of buccomaxillofacial surgeons regarding the aesthetics of facial profiles patterns I, II, and III in related to sex, ethnicity, and the main therapeutic procedures.
METHODS: We interviewed 18 specialist surgeons or surgeons in training in buccomaxillofacial surgery by using a standardized clinical report form for aesthetic evaluation and therapeutic procedures of 12 manipulated images simulating facial profiles, sex, and race.
RESULTS: As for aesthetics, the highlights were that facial profile type I had the highest mean values, whereas facial profile type III had the lowest mean values. However, no significant differences were found between the mean values obtained in different facial profiles in relation to sex and race. The therapeutic procedures were homogeneous in profiles II and III, with higher percentages for classical procedures in the orthosurgical treatment of these dentofacial deformities.
CONCLUSION: Facial profile I was considered more aesthetic. Furthermore, sex and racial type effects on aesthetics for the studied sample. Facial profiles I were the most difficult to assess as to therapeutic procedures, which resulted in a wide range of options in relation to profiles II and III.
Keywords: Perception; Therapeutic procedures; Maxillofacial abnormalities; Dental aesthetics.
RESUMO
INTRODUÇÃO: A cirurgia ortognática para correções de deformidades dentofaciais proporciona uma face mais harmoniosa, funcional e estética. O objetivo desse estudo foi avaliar a percepção dos cirurgiões bucomaxilofaciais quanto à estética dos perfis faciais padrões I, II e III, relacionada ao sexo, etnia e às principais condutas terapêuticas.
MÉTODOS: Foram entrevistados 18 cirurgiões especialistas ou em formação em Cirurgia e Traumatologia Bucomaxilofacial, utilizando uma ficha clínica padronizada para avaliação estética e condutas terapêuticas de 12 imagens manipuladas simulando os perfis faciais, sexo e raças.
RESULTADOS: Quanto à estética, destacaram-se os perfis faciais tipo I, que apresentaram as melhores médias, enquanto os perfis faciais tipo III as menores; entretanto, não houve diferenças significativas entre as médias obtidas nos diferentes perfis faciais em relação ao sexo e à raça. As condutas terapêuticas foram homogêneas nos perfis II e III, com maiores percentuais para condutas clássicas no tratamento ortocirúrgico destas deformidades dentofaciais.
CONCLUSÃO: O perfil facial I foi o considerado mais estético; então, houve influência do sexo e do tipo racial na estética para a amostra estudada. Os perfis faciais I foram os mais difíceis de avaliar quanto às condutas terapêuticas, o que resultou em grande variedade de opções em relação aos perfis II e III.
Palavras-chave: Percepção; Condutas terapêuticas; Anormalidades maxilofaciais; Estética dentária.
Aesthetics and facial attractiveness are important human concerns and have always exerted a fascination on all organized societies over the centuries. To this day, the prevailing assumption is that a pleasant facial aesthetics is an important factor in psychosocial well-being and success in various professional and cultural areas, a fact that makes the quest for pleasant facial aesthetics almost constant, consciously or unconsciously1.
Dentistry is a prime area of health that acts predominantly on the face and plays an important role in the diagnosis and treatment of problems that impact aesthetics and facial attractiveness. Studies show that dental arcade rebound significantly in the facial appearance of individuals2 and that more than 70% of parents think that their children will become more attractive, more socially acceptable, and successful in their future professional life after dental3 treatment. Psychological problems related to self-esteem and sociability also have a close relationship with self-image concepts of a patient with deformities, not to mention the interpersonal problems of those subject to bullying4. There are also association and reports of orofacial pain to masticatory skeleton disproportions, yet despite that functional changes are always present, aesthetic complaints are most of the time the reason these patients seek treatment5.
In this context, it is increasingly common for patients to desire for a symmetrical face, both aesthetically and functionally, achieved through dental treatments that alter the dentofacial morphological structures. Therefore, it is essential that professionals evaluate the expectations of their patients and cautiously analyze facial features to define an adequate1,6 treatment plan.
Angle's classification, as cited by Reis et al.7, is used to determine the main dentofacial deformities, which can be divided into standard I, II, and III, in addition to long and short facial shapes. Pattern I is identified by the facial balance in which the malocclusion, when present is only dental and not associated with any sagittal or vertical8 skeletal discrepancy. Standards II and III are characterized by the sagittal level, respectively positive and negative, between the maxilla and mandible. In the long and short facial shapes, the discrepancy is vertical. In patients with skeletal disorders, malocclusions are usually a consequence of these discrepancies7.
The dental treatment associated with orthognathic surgery constitutes one of the dental procedures with greater chances of facial morphology changes for the purpose of functional, aesthetic, and psychological improvements. Orthognathic surgery refers to a group of corrective bone operations involving movement of the mandible and/or the mandible as a whole, as well as the adjacent soft tissue. Patients with dentofacial deformities should be carefully evaluated by using analysis of facial, cephalometric, and dental models representing the detailed analysis of soft tissues and maxillofacial skeleton, and the relationship dentoalveolar in various perspectives9.
Facial aesthetics is an important component in diagnosis and treatment planning in orthodontics and orthognathic surgery and are therefore of fundamental importance in various studies that aim to define normality, symmetry, and balance features. Nevertheless, professional opinion should coincide with the opinions and expectations of patients10. According to Todd et al.11, the clinical perception of the facial aesthetic professionals is not always the same as that of the general public. Hence, the subjectivity of morphological evaluation features in the dentofacial region significantly differ between surgeon dentists and amateurs.
Consequently, assessing the perception of professionals who are involved with dental surgical treatments on aesthetics and facial attractiveness regarding main facial profiles, sex, and predominant racial types and relating them to the main facial dentoskeletal movements for symmetrical correction of the face would become an important diagnostic parameter and correction of dentofacial deformities. Thus, these fill the gap in the national literature mapping of what professionals are thinking/judging and deciding/acting across a population as diverse and racially mixed as Brazil's.
OBJECTIVE
This study aimed to evaluate the perception of postgraduate dentists or postgraduate process in surgery and buccomaxillofacial trauma (SBMFT) on the aesthetics and attractiveness of facial profiles of patterns I, II, and III in relation to sex, race, and main dentoskeletal facial movements.
METHOD
This study was approved by the ethics in research committee (ERC) of Platform Brazil, with delivered consolidated written opinions (nº 144.239). Thus, in this pilot study, methodologically classified as an observational, analytical, prospective, transversal type inquiry12, we interviewed dentists of both sexes and different socioeconomic and cultural aspects of the city of Caruaru-PE, with specialist registration and active in SBMFT specialty or training program (residency in SBMFT). Data collection was performed by using a standardized clinical report form that initially had questions about the identification and demographic data of interviewed professionals, and then a scale to assess the aesthetics and facial attractiveness, and questionnaire on therapeutic procedures.
Twelve preselected images of individuals were available in the standard right-side profile, as seen in other methodologies13-15. Each of the 12 images corresponded to a facial profile, sex, and different race, printed on matte photo paper 15 × 21 cm in size and laminated individually, containing no identification written or numerical. Each picture was presented individually to each interviewed professional, which provided the necessary analysis time on the aesthetics and facial attractiveness observed, as well as its therapeutic decision for the case. After the available time or the indicated response, each image was taken and no longer available to the respondent, until he/she completed 12 different images. To avoid bias in the judgment of aesthetics and attractiveness, the sequence of 12 images was randomized.
Along with every available picture, a numbered scale, staggered16,17 from 0 to 10, was delivered to the interviewed professionals for its assessment as to the facial aesthetic of the corresponding image. Interviewed professionals were informed only that the tag number on the scale corresponds to an increasing sequence of aesthetics, that is, 0 being the least aesthetic appearance and 10 being the most aesthetic to him/her according to each image16,17.
The values obtained from the scale were analyzed by average points achieved (taking into account two decimal places) for each image of the facial profile and then grouped into the following four categories: category 1 (0-2.99), unattractive facial aesthetics; category 2 (3-5.99), facial aesthetics and regular attractiveness; category 3 (68.99), facial aesthetics and pleasant attractiveness; category 4 (9-10), very attractive facial aesthetics16,17.
In addition to the available scale, with each image, we presented a short multiple-choice questionnaire regarding the therapeutic options for each displayed case (image). Thus, the interviewed professional scored only one option regarding the procedure that he/she would like/prefer to adopt for that case demonstrated and analyzed. Treatment options were about dentoskeletal movement patterns for orthosurgical routine management of patients with dentofacial deformities and options were the same for all images (Chart 1).

The images were obtained through standardized photographs of four young adult volunteers (a white man, a black man, a white woman, and a black woman), photographed with a camera and taken in a professional studio. From the obtained and scanned images (12 in total), manipulations were performed by using the Dolphin Image program (version 11.5) in order to obtain the desired simulation of profiles according to the cephalometric measures of each standard facial, sexual, and racial type profiles (Figures 1 and 2). No other forms of diagnosis for judging the procedures were provided besides the profile images, such as images on other patterns, intrabuccal photographs, radiographs, plaster models, and bite records.
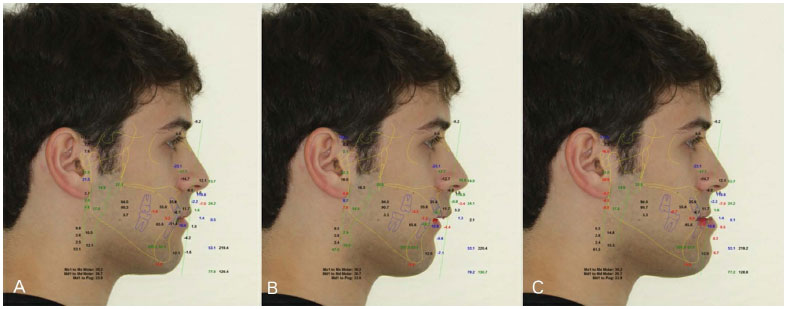
Figure 1. Example of images and cephalometric manipulations of facial profiles. The manipulation of profile I was obtained by mandibular retreat of 2 mm and plasty in the mentocervical line (A), while profile II was reached with mandibular retreat of 7 mm and maxillary advance of 2 mm (B) and profile III with mandibular advance of 7 mm (C).
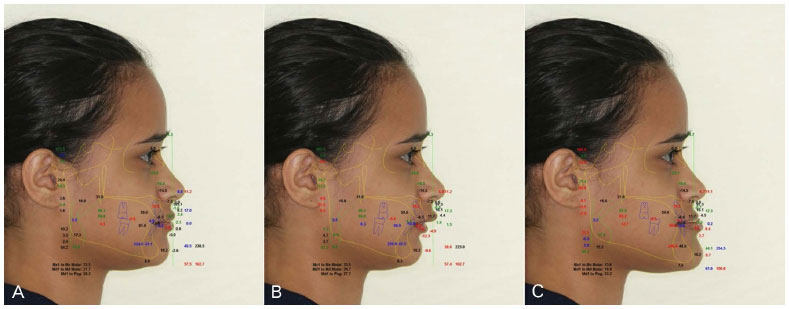
Figure 2. Example of images and cephalometric manipulations of facial profiles. The manipulation of profile I was obtained from mandibular advancement of 2 mm and the mento of 2 mm (A), while profile II was reached with mandibular retreat of 2 mm (B) and profile III was reached with a mandibular advancement of 10 mm, mento advancement of 5 mm, with a vertical increase of 4 mm (C).
From the methodology proposed for this pilot study, we included 18 professionals (14 men and 4 woman) who were included in the study and interviewed. Most were professional experts in SBMFT (n = 13) while only 5 were professionals still in their processes of training and expertise (residency in SBMFT). The mean age of the respondents was 35 years, and all reported some kind of activity with orthosurgery plans and procedures.
In the data analysis, absolute and percentage distributions and statistical measurements were obtained and presented as mean and standard deviation values. The following statistical tests were used: F test (analysis of variance) with Tukey comparisons and Student t test with equal or unequal variances. We emphasize that we established the variance equality hypothesis, which we performed by using the F Levene test. A P < 0.05 for bilateral hypothesis tests indicated a significant difference. All analyses were performed by using the SPSS statistical program (version 17).
RESULTS
Regarding facial aesthetics of the main patterns of the studied facial profiles, the averages showed that white male profiles class I (mean ± SD, 7.22 ± 2.32), black female class I (mean ± SD 6.94 ± 2.18), and white class I woman (mean ± SD 6.61 ± 1.94) were those best evaluated and classified as facial aesthetic and pleasant attractiveness. Meanwhile, the class III profiles, namely white woman class III (mean ± SD, 3.72 ± 2.37), black woman class III (mean ± SD, 3.56 ± 2.48), male white class III (mean ± SD, 3.56 ± 2.59), and male black class III (mean ± SD, 3.28 ± 2.47) were the ones with the lowest scores (Table 1), framed in the regular aesthetic and facial attractiveness classification. In Table 1, we can observe a significant difference between the means of facial profiles of the same racial type and sex, while no significant differences were found between sex and race for the same facial profile.

Tables 2, 3 and 4 show the results of the recommended procedures by 18 professionals for each sex and ethnicity in facial patterns I, II, and III, respectively. In the facial profile class I (Table 2), answers selecting therapeutic options for "no treatment needed" were for white male profile (44%) and for women's black profile (61.1%), followed by optional therapies, including "only corrections and/or orthodontic compensation," for white and black female profiles (22.2%). In the overall group, the most cited procedures were 33.3% for the "no treatment needed," 19.4% with "only corrections and/or orthodontic compensation," and 13.9% with "mandibular advancement."

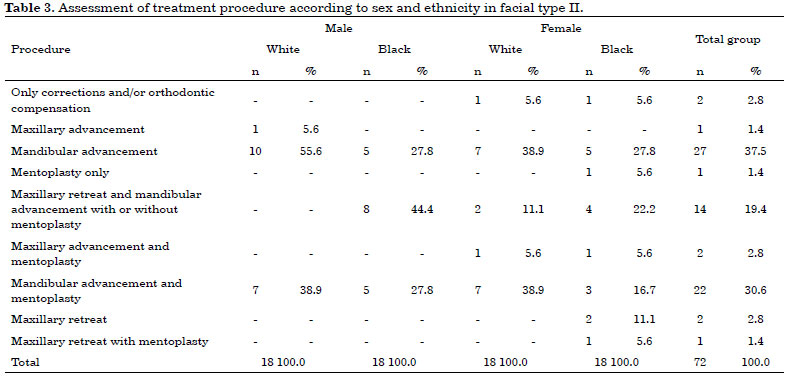
In the facial type II (Table 3), the most cited procedures were "mandibular advancement" in 10 and "mandibular advancement and mentoplasty" in 7 white male patients, "mandibular retreat and mandibular advancement with or without mentoplasty" in 8 black male patients, "mandibular advancement" in 5 patients, and "mandibular advancement and mentoplasty" in 5 patients. Among the black female patients, 7 underwent "mandibular advancement" and 7 underwent "mandibular advancement with mentoplasty." Among the black female patients, 5 underwent "mandibular advancement" and 4 underwent "mandibular retreat and mandibular advancement with or without mentoplasty." In the entire group, the most cited procedures were "mandibular advancement" (37.5%), "mandibular advancement and mentoplasty" (30.6%), and "maxillary retreat and mandibular advance with or without mentoplasty."
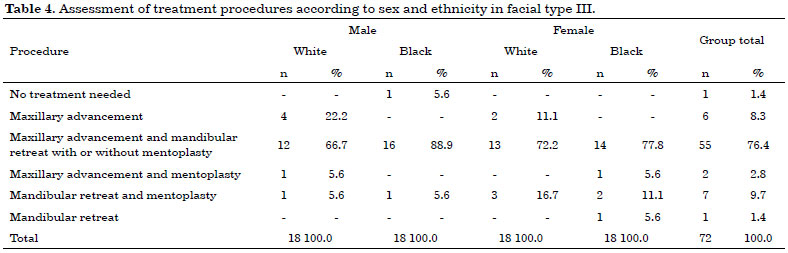
In the facial type III (Table 4), the procedure "advance and retreat mandibular with or without mentoplasty" was cited by most professionals, with percentages of 66.7% in white patients, 88.9% in black patients, 72.2% in white patients, and 77.8% in black patients. In the entire group, the percentage corresponding to the said procedure was about three-fourths (76.4%) of 18 professionals.
DISCUSSION
Facial aesthetics is an important component in the diagnosis and treatment plan in orthodontics and orthognathic surgery, as the appearance directly affects the classification of dentofacial deformities. Although the concept of beauty is subjective, a consensus indicates that an asymmetrical face, besides being aesthetically uncomfortable, is the cause for corrective treatments for greater social integration and self-esteem. However, the professionals involved in these types of treatments have training conditions and techniques to establish the classification parameters of the main facial patterns. Thus, studies in this area become important to define features of normality, dentofacial symmetry, and balance. In this way, professional advice and treatment plan will approach opinions and expectations of patients10. Still, no information was available about the views of dentists on the aesthetic impression of main facial profiles, taking into account sex and ethnicity, and above all, decision making when facing such profiles. In this pilot study, we first decided to study a small sample, but representative of active buccomaxillofacial surgeons in Caruaru-PE. Second, we intend to extend this research to other municipalities and other specialties such as orthodontics.
Facial analysis is essential in the diagnostic process and treatment planning for dentofacial deformities. What was once based on pure cephalometric concepts started to use a more consistent analysis with the patients' aesthetic needs to a new diagnosis based on facial morphological analysis. Thus, this established defined rules in the treatment of bad dental positions and facial asymmetries. Currently, this analysis is based not only on cephalometric numbers but also on the patient's direct visual analysis or on frontal and profile photographs in order to classify faces in profiles I, II, and III, short and long facial shapes, with or without asymmetries7,18. The authors of this study acknowledge that there was a methodological limitation to present only images on standard right-side profile for each facial, sex, and ethnicity pattern, despite being in line with other studies that used only pictures in profile13-15,18.
Thus, the results of this research showed that for the studied sample, the male facial profile I obtained more points with the facial aesthetic questionnaire and that, overall, facial profile I was best significantly evaluated in relation to profiles II and III. In this context, it was already expected that profile I would be better evaluated, considering that is the profile with greater balance and symmetry between the facial thirds. Noteworthy was the fact that profile II was better assessed than profile III, the latter being the one with the lowest mean in facial aesthetic aspect, as some studies show the opposite18. Thus, it is estimated that profile III requires more attention from professionals regarding aesthetic changes than profiles II in both sexes and ethnic groups, or the manipulations performed on the images have negatively affected the interpretation of aesthetics by the professionals.
As for ethnicity, assessment of individuals of white race prevailed that of individuals of African descent. Except from black female facial profile I, all other studied profiles had assessment means of aesthetics superior to the corresponding white ethnicity. Nevertheless, as the differences were not statistically significant, we cannot say that for this sample, there were significant racial effects on the judgment of facial aesthetics by professionals. The same thing happened with regard to sex, where there were no significant differences between the means of aesthetics' evaluations in different facial profiles. These results become interesting when we know that the sample studied outside professionals might consider the more technical aspects of the facial features rather than ethnic or sex criteria in judging aesthetics as an amateur13 person normally would.
When we analyzed the data on therapeutic procedures in the studied facial profiles, we found a greater heterogeneity in responses especially in profile I, while profiles II and III had a greater homogeneity in the responses of procedures. At first, it seems contradictory that facial profile I, which is already in facial symmetry, obtained yet heterogeneous answers about procedures, when it was expected that almost all of the answers would fall on the "no treatment needed" or "only corrections and/or orthodontic compensation," which generally occurred in only one-third of interviewed professionals. Furthermore, precisely because they are of profile I, the professionals' interpretations became more difficult, coupled with the fact that they were not provided other forms of diagnosis for the judgment of procedures, such as images on other patterns and other radiographs and models with bite records.
When we analyzed the responses of professionals regarding procedures of facial profiles II, we observed a larger and more homogeneous concentration of responses in just three options most commonly indicated for patients with this profile. Thus, analyzing the total group, the options "mandibular advancement," "mandibular advancement and mentoplasty," and "maxillary retreat and mandibular advancement with or without mentoplasty" were the most chosen and are consistent with treatment proposals of patients with retrognathia profile II.
Similarly, facial profile III also had good homogeneous responses regarding therapeutic procedures and about 80% of respondents indicated "maxillary advancement and mandibular retreat" as the most suitable option for facial profiles studied and with diagnosis limitations. For these dentofacial deformities, especially with large discrepancies between the arches, usually orthosurgical treatments are combined with movements spread between the maxilla and mandible, a fact that was observed in this research.
It is clear that this pilot study also has some limitations, and its results cannot be extrapolated to a more globalized reality. The fact that we use only a single image of each facial profile makes it not quite possible to perform a complete and thorough professional evaluation to judge the case therapeutics' procedure. Normally, in addition to standard profile facial analysis, we also use the frontal standards, three-fourth profile, and submental-vertex. However, other analyses such as the cephalometric analysis and the study of dental arches models were performed. Another limitation concerns the manipulation of images to achieve the desired facial profiles, which for some, can be a complicating factor in the aesthetic evaluation. Even as a negative point was the nonprobabilistic and small sample size, limited to just a single municipality. The authors agree with such study limitations. However, in the case of a pilot study, we assume that at this time, we aimed to preliminarily assess the aesthetic and therapeutic management from a single profile image, these being manipulated to avoid potential interference with the judgment of aesthetics by external factors that were not the patient's own dentofacial deformity (e.g., hair, nose, ear, accessories, etc.). Even dealing with a small sample, it represented all the active dental surgeons active in surgery and buccomaxillofacial trauma in Caruaru-PE. Based on this methodology and results, other studies will be developed to minimize failures and achieve results with a bigger and better validation and include in the sample more professionals and other specialties related to dentofacial deformities.
CONCLUSIONS
In this study, we found that for the studied sample, profile I is the most aesthetic compared with profiles II and III, and profile III was rated as the least aesthetic. For this sample and methodology, sex and ethnicity have no significant effect on the judgment of facial aesthetic by interviewed professionals. However, the facial profile of Caucasians obtained, in general, better evaluation means.
The therapeutic procedures were more diverse and heterogeneous in facial profile I, while in profiles II and III, uniformity in the answers with a predominance of combined orthosurgical treatments was greater.
REFERENCES
1. Delalíbera HVC, Silva MC, Pascotto RC, Terada HH, Terada RSS. Avaliação estética de pacientes submetidos a tratamento ortodôntico. Acta Scient Health Sci. 2010;32(1):93-100.
2. Feitosa DAS, Dantas DCRE, Guênes GMT, Ribeiro AIAM, Cavalcanti AL, Braz R. Percepção de pacientes e acadêmicos de odontologia sobre estética facial e dentária. Rev Fac Odontol Univ Passo Fundo. 2009;14(1):23-6.
3. Kiekens RM, Maltha JC, van 't Hof MA, Kuijpers-Jagtman AM. A measuring system for facial aesthetics in Caucasian adolescents: reproducibility and validity. Eur J Orthod. 2005;27(6):579-84. DOI: http://dx.doi.org/10.1093/ejo/cji053
4. Veronez FS, Tavano LDA. Modificações psicossociais observadas pós-cirurgia ortognática em pacientes com e sem fissuras labiopalatinas. Arq Ciênc Saúde. 2005;12(3):133-37.
5. Ambrizzi DR, Franzi SA, Pereira Filho VA, Gabrielli MAC, Gimenez CMM, Bertoz FA. Avaliação das queixas estético-faciais em pacientes portadores de deformidades dentofaciais. R Dental Press Ortodon Ortop Facial. 2007;12(5):63-70. DOI: http://dx.doi.org/10.1590/S1415-54192007000500009
6. Reis SAB, Abrão J, Claro CAA, Capelozza Filho L. Avaliação dos fatores determinantes da estética do perfil facial. Dental Press J Orthod. 2011;16(1):57-67. DOI: http://dx.doi.org/10.1590/S2176-94512011000100010
7. Reis SAB, Abrão J, Capelozza Filho L, Claro CAA. Estudo comparativo do perfil facial de indivíduos Padrões I, II e III portadores de selamento labial passivo. R Dental Press Ortodon Ortop Facial. 2006;11(4):36-45.
8. Ferreira FV. Ortodontia: Diagnóstico e Planejamento Clínico. 7a ed. São Paulo: Artes Médicas; 2008.
9. To EWH, King WWK, Au O. Reshaping the face with orthognathic surgery: an overview [Acesso 20 Jul 2012]. Disponível em: http://www.fmshk.org/article/862.pdf
10. Almeida MD, Farias ACR, Bittencourt MAV. Influência do posicionamento sagital mandibular na estética facial. Dental Press J Orthod. 2010;15(2):87-96. DOI: http://dx.doi.org/10.1590/S2176-94512010000200012
11. Todd SA, Hammond P, Hutton T, Cochrane S, Cunningham S. Perceptions of facial aesthetics in two and three dimensions. Eur J Orthod. 2005;27(4):363-9. DOI: http://dx.doi.org/10.1093/ejo/cji024
12. Peres MA, Ferreira A. O método epidemiológico de investigação e sua contribuição para a Saúde Bucal. In: Antunes JLF, Peres MA, Org. Epidemiologia da Saúde Bucal. Rio de Janeiro: Guanabara Koogan; 2006. p.3-17.
13. Johnston DJ, Hunt O, Johnston CD, Burden DJ, Stevenson M, Hepper P. The influence of lower face vertical proportion on facial attractiveness. Eur J Orthod. 2005;27(4):349-54. DOI: http://dx.doi.org/10.1093/ejo/cji023
14. Lee LH, Jun JH, Danganan M, Pogrel MA, Kushner H, Lee JS. Orthognathic surgery for the Asian patient and the influence of the surgeon's background on treatment. Int J Oral Maxillofac Surg. 2011;40(5):458-63.
15. Soares DM, Palmeira PTSS, Pereira VF, Santos MESM, Tassitano RM, Laureano Filho JR. Avaliação dos principais padrões de perfil facial quanto a estética e atratividade. Rev Bras Cir Plást. 2012;27(4):547-51. DOI: http://dx.doi.org/10.1590/S1983-51752012000400013
16. Vargo JK, Gladwin M, Ngan P. Association between ratings of facial attractivess and patients' motivation for orthognathic surgery. Orthod Craniofac Res. 2003;6(1):63-71. DOI: http://dx.doi.org/10.1046/j.1439-0280.2003.2c097.x
17. Kiekens RM, Maltha JC, van't Hof MA, Kuijpers-Jagtman AM. Objective measures as indicators for facial esthetics in white adolescents. Angle Orthod. 2006;76(4):551-6.
18. Cavichiolo JC, Salazar M, Cuoghi OA, Mendonça MR, Furquim LZ. Avaliação da agradabilidade facial de pacientes portadores de padrão facial II e III por ortodontistas e leigos. Odonto. 2010;18(36):73-81. DOI: http://dx.doi.org/10.15603/2176-1000/odonto.v18n36p73-81
1. Faculdade ASCES, Caruaru, PE, Brazil
2. Universidade Federal de Pernambuco - UFPE, Recife, PE, Brazil
3. Universidade de Pernambuco - UPE, Recife, PE, Brazil
Institution: Faculdade ASCES - Associação Caruaruense de Ensino Superior, Caruaru, PE, Brazil.
Corresponding author:
Marconi Eduardo Sousa Maciel Santos
Av. Portugal, 584, Bairro Universitário
Caruaru, PE, Brazil Zip code 55016-400
E-mail: marconimaciel@gmail.com
Article received: July 28, 2014.
Article accepted: April 21, 2015.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket