



Original Article - Year 2015 - Volume 30 -
Results of the correction of syndactyly of the hand by using Skoog's technique
Resultados da correção da sindactilia na mão com a técnica de Skoog
ABSTRACT
INTRODUCTION: Syndactyly is a congenital anomaly of the hand, occurring in approximately 1 in every 2000 births. It is more common in male patients and is present in both hands in 50% of the cases. The objective of this study was to describe a series of cases of patients with hand syndactyly, operated at the Sarah Hospital in Brasília using modified Skoog's technique and orthosis.
METHODS: The modified Skoog's technique was performed to correct syndactyly. Wrist-hand and finger orthosis was applied postoperatively, and the appearance of the scar was assessed according to the Vancouver Scar Scale.
RESULTS: Forty-five patients were assessed during five years, of whom 30 (66%) were male and 15 were female, all aged between 1 and 4 years (mean age: 2 years [60%]); 37% of cases were associated with syndromes and 50% were simple bilateral cases. Complications observed in simple syndactyly occurred in 8% of patients and included scar retraction, visible scars, and ungual changes; three patients (6%) underwent revision surgery with z-plasty and confection of a new web space commissure to correct scar retraction, and four patients required finger realignment, observed in complex syndactyly.
CONCLUSION: This technique resulted in 92% good functional outcomes, 8% complications associated with the surgical technique, and three revision procedures with z-plasty and confection of the web space commissure with a new flap and skin graft to correct scar retraction. The Vancouver scale was used to assess scar quality, and pigmentation between the fingers (due to skin graft) had the highest score.
Keywords: Syndactyly; Congenital syndactyly; Syndactyly Correction.
RESUMO
INTRODUÇÃO: A sindactilia é uma anomalia congênita comum da mão, tem incidência de aproximadamente um em 2.000 nascimentos, predomínio no sexo masculino e é bilateral em 50% dos casos. Objetivo é descrever uma série de casos de pacientes com sindactilia nas mãos, operados no Hospital Sarah Brasília, com a técnica de Skoog modificada e o uso de órtese.
MÉTODOS: Realizou-se a técnica de Skoog modificada para correção de sindactilia. No pós-operatório, foi confeccionada órtese punho-mão e dedos, e procedeu-se à avaliação do resultado da cicatriz conforme a Escala de Vancouver.
RESULTADO: Durante cinco anos, avaliaram-se 45 pacientes, sendo 30 (66%) homens e 15 mulheres, com idade de um a quatro anos (média de dois anos - 60%), 37% dos casos mostraram-se associados a síndromes, 50% eram simples e bilateral. As complicações observadas nas sindactilias simples foram encontradas em 8% dos pacientes e caracterizaram-se por retração cicatricial, cicatriz visível e alteração ungueal; três casos (6%) foram reoperados para liberação de retração cicatricial com zetaplastia e confecção de neocomissura e quatro casos demandaram realinhamento digital, observado nas sindactilias complexas.
CONCLUSÃO: Com esta técnica, obtiveram-se 92% de resultados funcionais, 8% de complicações relacionadas à técnica cirúrgica e três reoperações para liberação de retração cicatricial, por meio de zetaplastia e aprofundamento da comissura com novo retalho e enxerto de pele Em relação à avaliação quanto à Escala de Vancouver, o item predominante foi a pigmentação existente entre os dedos devido ao enxerto de pele.
Palavras-chave: Sindactilia; Sindactilia congênita; Correção da sindactilia.
Syndactyly is a common congenital anomaly of the hand, occurring in approximately 1 in every 2000 births. It is more common in male patients and is present in both hands in 50% of the cases1-4. Family history is present in 10-40% of cases because of dominant autosomal inheritance; it has variable expression, incomplete penetrance, and variable phenotype within a family lineage. Syndactyly is characterized by the fusion of soft tissue and/or skeletal elements of adjacent fingers, and may be associated with other anomalies such as polydactyly, clinodactyly, symphalangism, synostosis, brachysyndactyly, and syndromes such as Apert and Pfeiffer syndromes. It is usually noticed immediately after birth, unless the anomaly is incomplete and mild. It is categorized into five forms, from simple to complex; the third space is the most affected (57%), followed by the fourth space (27%)4. The characteristics that should be analyzed are the affected space, the extension of the syndactyly, the involvement of the nail and bone tissue, and the presence of other anomalies. The surgery should be performed at a minimum age of 1 year, depending on the clinical and local conditions and ensuring that finger growth is not compromised. Various techniques have been used to separate fingers with syndactyly, with or without skin grafts. Dorsal flap techniques result in dorsal and more visible scars. Some techniques lead to short or visible web space commissures, whereas others do not apply to certain types of syndactyly1.
OBJECTIVE
The objective of this study was to describe a series of cases of patients with syndactyly who underwent surgery at the Rehabilitation Hospital, using modified Skoog's3 technique and orthosis placement in the postoperative period.
METHODS
The study was evaluated and approved by the ethics committee of the Associação das Pioneiras Sociais (CAAE: 39220514.7.0000.0022).
Surgical technique
The procedures were performed under general anesthesia. A pneumatic tourniquet cuff was used at a mean pressure of 150 mm Hg. A new web space commissure was confectioned with volar and dorsal flaps (Figure 1). A proximal triangular flap was created in the volar region; the reference was a line corresponding to the fold in the finger of the remaining web spaces and to half of the width of the finger and the apex at 50% of the proximal phalanx; a proximal triangular flap was created in the dorsal region and located between the two metacarpal heads and the apex at 50% of the proximal phalanx (Figure 2). The release of the fingers was performed by using zigzag incisions, avoiding the interphalangeal fold. The dorsal and volar markings were then initiated, with the priority being the creation of a flap for the joints; the raw spaces were covered with full-thickness skin grafts from the ulnar side of the hand, anterior region of the wrist, inguinal region, or lower abdomen. Suture was performed with absorbable thread, and occlusive dressing was applied for 1 week.

Figure 1. Preoperative appearance of syndactyly. From left to right: transoperative sequence of syndactyly correction using Skoog's technique.

Figure 2. Preoperative appearance of the patient with syndactyly and postaxial polydactyly (above); 1 year after surgical correction of an interdigital space and removal of supernumerary finger (below).
Postoperative period
The dressings were changed weekly until complete healing of the skin grafts (average 15 days). Custom-made static orthosis (Figure 3), with the wrist in the neutral position and hand and fingers extended, was worn postoperatively during the night for 6 months to 1 year. Follow-up assessment occurred every 6 months. The Vancouver Scar Scale5 (Figure 4) was used to assess vascularization, pigmentation, malleability, and thickness of the scar in the late postoperative period.

Figure 3. Wrist-hand and finger volar orthosis worn postoperatively.
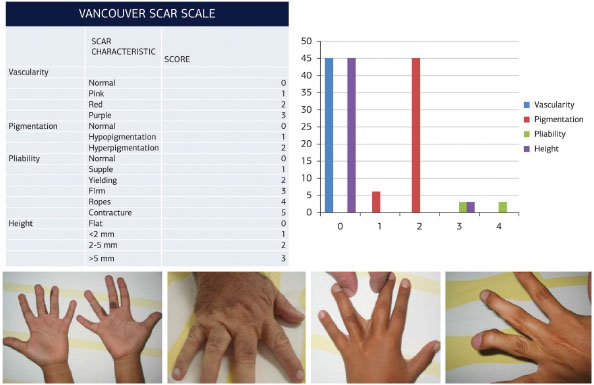
Figure 4. Results according to the Vancouver Scar Scale5.
RESULTS
In the period between 1996 and 2010, 685 cases of syndactyly were treated (Figure 5). The Sarah Network had 48 patients per year, 52% of whom were treated in Brazil (Figure 6); of these, 56% were male patients. In the cross-sectional study from 2005 to 2010, 45 patients who had undergone hand syndactyly correction were assessed, of whom 30 (66%) were male and 15 were female. The age at the time of surgery was 1-4 years (mean, 2 years [60%]). Of the cases, 37% were associated with Greig, amniotic band, Poland (Figures 7-10), Cornelia de Lange, Rubinstein Taybi, and Apert syndromes; macrodactyly; and other anomalies. Fifty percent were simple bilateral syndactyly cases; more than one space was affected in 17% of cases; and the third interdigital space was affected in 84% of cases (Figures 11 and 12). Complications in cases of simple syndactyly occurred in 8% of patients and included scar retraction, visible scar, and ungual changes; 6% (three patients) underwent revision surgery with z-plasty and confection of a new web space commissure to release scar retraction; and four patients with complex syndactyly exhibited complications related to associated bone deformities, regardless of the technique. The mean duration of the follow-up was 18 years. According to the Vancouver Scar Scale5, pigmentation had the highest score because the skin graft between the interdigital spaces remained visible throughout life; the remaining parameters showed results comparable to normal skin.
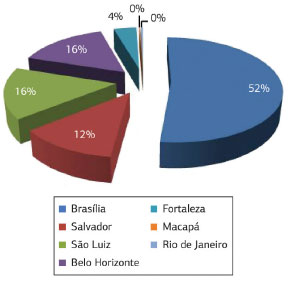
Figure 5. Distribution of the syndactyly cases treated at the Hospitals of the Sarah Hospital Network, from 1996 to 2010.
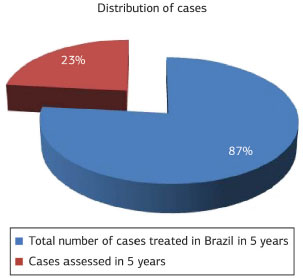
Figure 6. Percentage of cases studied among the cases treated at the Hospital Sarah Brasília, from 2005 to 2010.
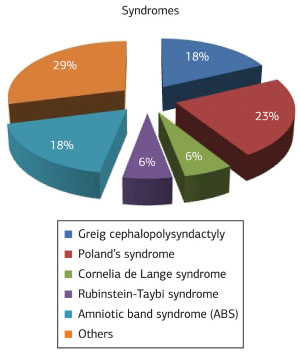
Figure 7. Distribution of association between syndactyly and syndromes.
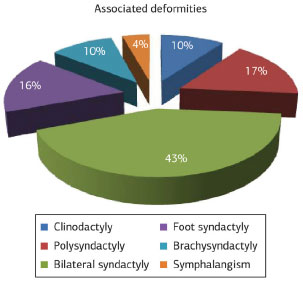
Figure 8. Distribution of deformities associated with cases of syndactyly assessed from 2005 to 2010.
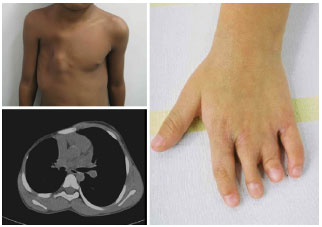
Figure 9. Example of a case of associated with Poland syndrome, brachysyndactyly, and thoracic deformity; thoracic computed tomography (below) and brachysyndactyly after correction of two interdigital spaces (right).

Figure 10. Case of brachysyndactyly, preoperatively (above) and after the correction of the interdigital spaces (below).

Figure 11. Before and after the correction of syndactyly.

Figure 12. Late postoperative result of bilateral syndactyly correction of the third interdigital space.
DISCUSSION
In this series of cases, syndactyly occurred mostly in male patients and was associated with syndromes and other malformations, which is in line with the results of relevant literature1,4,6. The technique described in this study was a modified version of that proposed by Skoog3 and included confection of proximal triangular flaps with rich blood supply. Flap transposition and joining in the interdigital space resulted in an appearance similar to that of normal space web skin. In addition, this technique allowed the full-thickness grafts to be hidden in the radial and ulnar sides of the fingers and palm. The zigzag incision and the interposition of the flaps increased the extension of the finger's length when palm skin was scarce; the priority was to cover the finger using tweezer function and to cover the interphalangeal joints using flaps.
Various techniques have been described by Bauer7, Marumo2, and others4,6, and the variations are mainly related to the flap created to reconstruct the commissure. Skoog's technique3 showed good results and prevented the risk of a cross-sectional scar between the fingers that leaves a visible interdigital membrane postoperatively. Moreover, full-thickness skin graft was used to cover raw areas and custom-made orthosis was used to prevent scar retraction, which is associated with more complex deformities1,4,6. Percival8 conducted a 10-year review of 218 patients who had undergone syndactyly correction, and reported that the preoperative factors that influenced the result were complexity of the syndactyly and the presence of other congenital anomalies of the hand. The technique-related factor that most influenced the result was the type of skin graft used: partial-thickness skin graft resulted in more complications. At least one revision surgery was necessary in 42 cases to obtain an acceptable result; these included 22% with synechia of the interdigital space, 26% with flexion contracture, and five patients developed both contracture and synechia. By contrast, the type of flap used to reconstruct the interdigital space had little influence on the result. In this study, the use of full-thickness skin grafts in all cases and the wearing of palm orthosis during the night resulted in a low incidence of scar retraction (three cases). Furthermore, the timing of surgery, at 2-4 years of age (before the end bone growth), was an important factor because late surgical correction of multiple complex syndactyly can progress to flexion deformity, angulation, and finger rotation. With regard to scar quality, pigmentation had the highest score (score 2), i.e., the color of scars from skin grafting was that of the graft and thus different from the receiving skin.
CONCLUSION
The proposed technique resulted in 92% good results and 8% complications; three patients underwent revision surgery with z-plasty and confection of a web space commissure with a new flap and skin graft to relieve scar retraction. This technique has been widely used since 1970 and has provided versatility and satisfactory results with the use of triangular flaps. The Vancouver scale was used to assess scar quality, and pigmentation had the highest score because of the abdominal full-thickness skin graft; however, the use of full-thickness skin graft combined with the wearing of postoperative wrist-hand orthosis during the scar maturation period provided good functional results.
REFERENCES
1. Jordan D, Hindocha S, Dhital M, Saleh M, Khan W. The epidemiology, genetics and future management of syndactyly. Open Orthop J. 2012;6(1):14-27. http://dx.doi.org/10.2174/1874325001206010014. PMid:22448207.
2. Dib CC, Monteiro CGZ, Vieira JGC JR, Arzuaga MM. Sindactilia: técnica de Marumo modificada. Revista Bras. Cir. Plast. 2009;24(1):110-4.
3. Skoog T. Atlas de cirurgia plástica. Barcelona: Salvat; 1976. p. 414-27.
4. Green DP, Hotchkiss RN, Pederson WC, Wolfe SW. Green's operative hand surgery. 5th ed. Philadelphia: Elsevier; 2005. p. 1381-2. (vol. 2).
5. eHow. Vancouver Scar Scale scores [cited 2013 June 10]. Available from: disponível em http://www.ehow.com/how_7824385_train-vancouver-scar-scale.html.
6. Kozin SH. Syndactyly. J Hand Surg Am. 2001;1(1):1-13. http://dx.doi.org/10.1053/jssh.2001.21778.
7. Bauer TB, Tondra JM, Trusler HM. Technical modification in repair of syndactylism. Plast Reconstr Surg. 1956;17(5):385-92. http://dx.doi.org/10.1097/00006534-195605000-00007. PMid:13335516.
8. Percival NJ, Sykes PJ. Syndactyly: a review of the factors which influence surgical treatment. J Hand Surg. 1989;14(2):196-200. http://dx.doi.org/10.1016/0266-7681(89)90125-3.
Hospital Sarah Brasília, Brasília, DF, Brazil
Institution: Study carried out at Hospital Sarah Brasília, Brasília, DF, Brazil.
Corresponding author:
Katia Torres Batista
Hospital Sarah Brasília, SMHS, Qd. 501, Conjunto A
Brasília, DF, Brazil Zip Code 70335-901
E-mail: katiatb@terra.com.br
Article received: June 19, 2014
Article accepted: December 13, 2014
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket