



Ideas and Innovation - Year 2014 - Volume 29 -
Inversion of the lateral portion of the orbicularis oculi muscle for the treatment of periocular rhytides (crow's feet)
Inversão da porção lateral do músculo orbicular para tratamento das rítides perioculares (pés-de-galinha)
ABSTRACT
INTRODUCTION:In the continued search for increasingly expressive results, plastic surgeons are combining established techniques with new intraoperative times. This article describes a surgical technique associated with rhytidoplasties based on the resection of the lateral portion of the orbicularis oculi muscle, followed by grafting the muscle itself, however inverted, on the resected area.
METHOD: In a 5-year period, 54 rhytidoplasties associated with the described technique were performed.
RESULTS: The follow-up in the late postoperative period (5 years) was satisfactory, with the permanent disappearance of periocular rhytides due to the neutralization of the forces exerted by the muscle in this area. There was no dissatisfaction on the part of the patients. Consequently, the procedure had excellent results in the resolution of periocular rhytides and in lifting the caudal part of the eyebrow in relation to the orbit.
CONCLUSION: The technique described generates permanent and satisfactory results.
Keywords: Orbicularis oculi muscle; Wrinkles; Facelift; Periocular rhytides; Rhytidoplasty.
RESUMO
INTRODUÇÃO: A cirurgia plástica, sempre em busca de resultados cada vez mais expressivo, vem associando às técnicas já consagradas aos novos tempos intraoperatórios. Este trabalho descreve uma técnica cirúrgica para ser associada às ritidoplastias baseada na ressecção da porção lateral do músculo orbicular, seguida pela enxertia do próprio músculo, porém invertido, sobre a área ressecada.
MÉTODO: Em um período de 5 anos, foram realizadas 54 ritidoplastias associadas a técnica descrita.
RESULTADOS: O seguimento no pós-operatório tardio (5 anos) mostrou-se satisfatório com permanente desaparecimento das ritides perioculares por neutralizar as forças exercidas pelo músculo nesta área. Não houve insatisfação por parte dos pacientes. Logo, trata-se de um procedimento com excelentes resultados na resolução das ritides perioculares e na elevação da porção caudal da sobrancelha em relação a orbita.
CONCLUSÃO: A técnica descrita gera resultados permanentes e satisfatórios.
Palavras-chave: Músculo orbicular; Rugas, Facelift; Ritidoplastia.
Besides playing a fundamental role in human contact, the face also reflects the aging process. Aging is divided classically into intrinsic and extrinsic categories; the clinical course of the aging process is reflected in the flaccidity of the skin, deepening of the expression lines, and planning of the epidermal dermal junction, with significant changes in color, texture, and quality of the skin in general1.
Currently, plastic surgery offers several techniques for facial rejuvenation, based on the concept of "facelifting." The first report of a surgery with this purpose dates back to the beginning of the 20th century (1901) in Berlin, when Eugen Höllander1 described a procedure very similar to the "facelift" done today.
The search for increasingly perfect results means that the major facelift techniques are constantly improved and added to other surgical procedures to meet current aesthetic concerns.
Furthermore, it is known that the best surgical result should be based on two factors: an accurate diagnosis of the facial anatomy and the combination of intraoperative times to optimize the results.
Thus, this article describes a surgical technique associated with rhytidectomy, based on resection of the lateral portion of the orbicularis oculi muscle followed by grafting the muscle itself on the resected area. This procedure provides excellent results in the resolution of periocular rhytides and in raising the caudal portion of the eyebrow in relation to the orbit.
As this technique is based on the manipulation of the orbicularis oculi muscle, it is important to know that this muscle is a thin and flat elliptical sphincter that involves the orbital opening and consists of two portions: orbital and palpebral2. Strong eyelid closure occurs in collaboration with the orbital portion, moving the skin of the forehead, temple, and cheek toward the average angle of the eyelids. This results in radiated skin folds in the lateral angle of the eyelids, which become permanent in older people or those with advanced degrees of photoaging ("crow's feet")1.
METHOD
During a 5-year period, in the private practice of the author, 54 facelift surgeries were performed with rejuvenation purposes, by using a precapillary incision technique (the author's option) associated with the procedure described in this article.
All patients were informed about the technique and its potential complications, and they gave free and informed consent for the surgery.
The postoperative follow-up of 5 years and the final result were based on the satisfaction of the patients and on the absence of rhytides in the lateral region of the orbit.
Technique
The patients were submitted to sedation and blocking with infiltration of a local anesthetic solution (2% lidocaine and ropivacaine). The technique was based on a precapillary skin incision and dissection of the subcutaneous tissue with a no. 15 blade, exposing the superficial temporal fascia (Figure 1), until the complete exposure of the lateral portion of the orbicularis oculi muscle and the inferior margin of the orbit (Figure 2).

Figure 1. Precapillary incision and dissection up to the superficial temporal fascia.
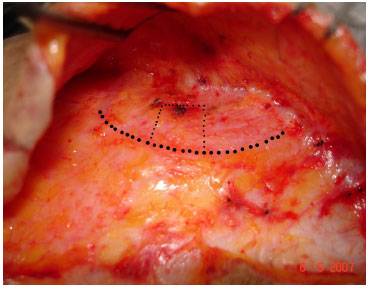
Figure 2. Lateral margin of the orbicularis oculi muscle and projection (minor dots) of the future quadrangular resection of this muscle.
When the lateral face of the orbicularis oculi muscle is fully exposed, the technique described herein consists in the removal of a quadrangular segment of approximately 2.5 cm ' 2 cm of this lateral margin of the muscle (Figures 3 and 4), with grafting of the same muscle segment, but inverted, in the resected area (Figures 5 and 6), in order to avoid a periocular skin depression.
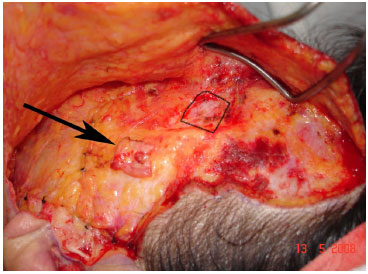
Figure 3. Quadrangular portion (2.0 ' 2.5 cm) of the already resected orbicularis oculi muscle (arrow).
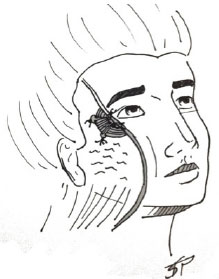
Figure 4. Schematic of the 2.0x2.5cm portion of the orbicularis oculi muscle to be dissected.
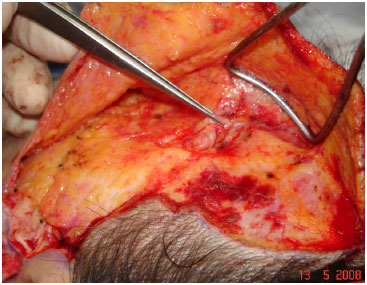
Figure 5. Graft of the orbicularis oculi muscle being repositioned in an inverted position.
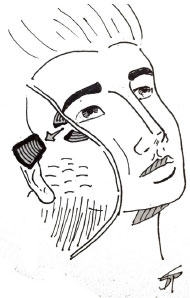
Figure 6. Repositioning the muscle graft with local suture (nylon 6-0).
The grafted muscle is then sutured in its margins with mononylon 6.0, seeking to recreate the previous geometry of the orbicularis oculi muscle (Figure 7).
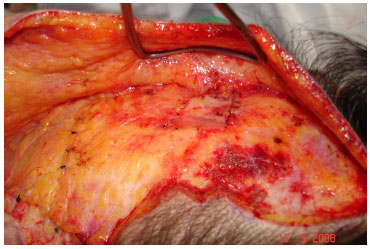
Figure 7. Graft repositioned and sutured with nylon 6-0. Final aspect.
RESULTS
Among the 54 patients who underwent this procedure of resection and grafting of the orbicularis oculi muscle, 53 were female and 1 was male. Their age varied between 45 and 72 years.
The follow-up in the late postoperative period (5 years) was satisfactory, with the permanent disappearance of periocular rhytides due to the neutralization of the forces exerted by the muscle in this area. There were no cases of depression of the periocular cutaneous lift.
Furthermore, the distance between the tail of the eyebrow and the lateral canthus of the orbit increased significantly, due to the decrease of the local muscle tone, thus repositioning the eyebrow (Figures 8-13).

Figure 8. Case 1: preoperative aspect.

Figure 9. Case 1: postoperative aspect.

Figure 10. Case 2: preoperative aspect.

Figure 11. Case 2: postoperative aspect.

Figure 12. Case 3: Preoperative aspect with marking of the orbicularis oculi muscle portion to be resected.

Figure 13. Case 3: postoperative aspect.
In a follow-up period of 5 years after surgery, no permanent late complications were observed. However, as temporary postoperative complications, we observed the presence of residual edema under the manipulated area that later showed 100% resolution.
DISCUSSION
Although rhytidectomy techniques have changed over time with regard to the final results, their main development is based on the contribution of intraoperative time to enhance the result.
The concept of manipulation of the orbicularis oculi muscle has been described by some authors. Viterbo3, in 2003, described a myectomy of the orbicularis oculi muscle, but with a smaller area of muscle resection and a superficial musculoaponeurotic system graft at the site of resection of the lateral portion of the orbicularis muscle3.
We believe that the technique proposed in this article, where a greater muscle resection and grafting with the same tissue (muscle) is done, brings excellent aesthetic quality to the procedure, in addition to lowering the rates of change of the periocular cutaneous lift.
Concerning temporary postoperative complications, a slight edema was observed in the manipulated area, with 100% resolution in the late follow-up period. No late permanent complications were observed in the cases described.
CONCLUSION
The technique described - resection of a quadrangular portion of the lateral portion of the orbicularis oculi muscle - associated with classical rhytidoplasty techniques, generates permanent and satisfactory aesthetic results.
The neutralization of the orbicularis oculi muscle tone through its resection eliminates periocular rhytides (crow's feet), and repositions the eyebrow tail in relation to the orbit.
REFERENCES
1. Freilinger G. Surgical anatomy of the mimic muscle system and the facial nerve: importance for reconstructive and aesthetic surgery. Plast Reconstr Surg. 1987;80:686-90.
2. Gardner E, Gray DJ, O'Rahilly R. Anatomia: Estudo Regional do Corpo Humano. 4. ed. Rio de Janeiro: Guanabara Koogan; 1982. p. 620-50.
3. Viterbo F. New treatment for crow's feet wrinkles by vertical myectomy of the lateral orbicularis oculi. Plast Reconstr Surg. 2003;112(1):275-9.
4. Gardner E, Gray DJ, O'Rahilly R. Anatomia: Estudo Regional do Corpo Humano. 4. ed. Rio de Janeiro: Guanabara Koogan; 1982. p. 620-50.
5. Freilinger G. Surgical anatomy of the mimic muscle system and the facial nerve: Importance for reconstructive and aesthetic surgery. Plast Reconstr Surg. 1987;80:686-90.
6. Foad Nahai, The Art of Aesthetic Surgery Vol. II, Ed. QMP, 2011; p. 828-96.
1. Full Member of the Brazilian Society of Plastic Surgery - Head of the Department of Plastic Surgery of the Faculty of Medicine of Catanduva
2. Associate Member of the Brazilian Society of Plastic Surgery - Assistant Professor in the Department of Plastic Surgery of the Faculty of Medicine of Catanduva
3. Full Member of the Brazilian Society of Plastic Surgery - Assistant Professor in the Department of Plastic Surgery of the Faculty of 4. Resident Physician - Resident, Department of Surgery of the Faculty of Medicine of Catanduva
5. Resident Physician - Resident, Department of Plastic Surgery of the Faculty of Medicine of Catanduva
Institution: Faculty of Medicine of Catanduva.
Corresponding Author:
Manoel Alves Vidal
Avenida Orlando Zancaner, 497
Catanduva, SP, Brazil Zip code: 15801-120
E-mail: manoel.a.vidal@gmail.com
Article submitted: April 1, 2013.
Article accepted: June 29, 2013.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket