



Original Article - Year 2014 - Volume 29 -
Evaluation of four techniques for nipple reconstruction
Avaliação de quatro técnicas de confecção de papila
ABSTRACT
INTRODUCTION: Reconstruction of the nipple-areola complex represents the final and perhaps most difficult stage in breast reconstruction. Several techniques have been described; however, most of the methods do not seem to achieve adequate projection and are associated with the loss of projection over time, leading to an inadequate final aesthetic result. The objective of this study is to compare and evaluate the results and effectiveness of four different surgical nipple reconstruction techniques in the last 3 years.
METHOD: Sixty-four reconstructed nipples were evaluated using the skate flap (n = 17), double-opposing-tab flap (n = 15), four petals (n = 22), and contralateral nipple graft (n = 10) techniques. The results were evaluated in the long term by a blinded examiner who classified the results as fully satisfactory, satisfactory, partially satisfactory, or unsatisfactory.
RESULTS: The nipple graft showed significantly better results than the other groups (p = 0.012). There was no statistical difference when only the flaps (excluding the contralateral nipple graft) were evaluated (p = 0.102). However, when evaluating the outcome of nipple reconstruction according to primary reconstruction type, no difference was observed among the groups (p = 0.563).
CONCLUSION: The contralateral nipple graft technique proved to be the most efficient method that yielded better results; however, no difference was seen among the other evaluated techniques. Hence, when the contralateral nipple graft technique is not possible, surgeons should select the one with which they are most familiar.
Keywords: Breast Reconstruction; Nipple Reconstruction; Breast Cancer; Post-operative Complications.
RESUMO
INTRODUÇÃO: A confecção do complexo areolopapilar representa o estágio final nas reconstruções de mama, e talvez seja o mais difícil deles. Diversas técnicas são descritas, entretanto, a maioria delas não parece atingir a projeção adequada e sofre com a perda dessas com o passar do tempo, levando a um resultado final estético inadequado. O objetivo do trabalho é comparar e avaliar os resultados e eficácia de quatro técnicas cirúrgicas diferentes de confecção de papila, em cirurgias de reconstrução de mama nos últimos 3 anos.
MÉTODO: Foram avaliados 64 papilas reconstruídas, utilizando as técnicas de skate flap (n=17), double opposing flap (n=15), "4 pétalas" (n=22) e enxerto de papila contralateral (n=10). Os resultados foram avaliados, a longo prazo, por um examinador cego que classificou os resultados como totalmente satisfatório, satisfatório, parcialmente satisfatório e insatisfatório.
RESULTADOS: O enxerto de papila apresentou resultados significativamente melhores que dos outros grupos (p= 0,012). Não houve diferença estatística quando, somente, avaliados os retalhos (excluindo o enxerto de papila)(p=0,102). Já avaliando o resultado da papila confeccionada em função do tipo de reconstrução primária feita, não houve diferença entre os grupos (p=0,563).
CONCLUSÃO: O enxerto de papila contralateral se mostrou uma técnica mais efetiva e com melhores resultados. Na impossibilidade do seu uso, não há diferença entre as outras técnicas avaliadas, ficando a sua indicação àquela que se sinta mais familiarizado e capacitado a realizar.
Palavras-chave: Reconstrução da Mama; Reconstrução de Papila; Câncer de Mama; Complicações pós - operatórias.
Reconstruction of the nipple-areola complex (NAC) is the final stage in breast reconstruction in which the newly formed breast acquires an appearance as similar as possible to that of the contralateral breast. The diagnosis of breast cancer and its treatment with mastectomy have various important consequences for patients, particularly with regard to what it represents the most-their femininity.
Breast reconstruction, using either autologous tissues with musculocutaneous flaps or implants, is very important since it leads to a better self-assessment of body image as previously observed in several studies1,2,3. NAC reconstruction is the final, and perhaps most difficult, step in this process3.
Several retrospective studies4,5,6 have shown that patient satisfaction with breast reconstruction is directly related to NAC reconstruction, which demonstrates the importance of this surgical procedure in the final surgical result. In recent years, various surgical techniques have been developed with the aim of achieving the best NAC reconstruction method4-16. However, most do not seem to achieve the proper projection, which is are lost over time. Moreover, the loss of projection seems to be more prominent in certain techniques as compared to others.
OBJECTIVE
The present study aimed to compare and evaluate the results and effectiveness of four different nipple reconstruction techniques used in breast reconstruction surgeries in the last 3 years.
METHODS
All patients undergoing a secondary breast reconstruction between January 1, 2010 and January 1, 2013 in three clinics in Brasilia, Brazil, were included in the study.
Three plastic surgeons with extensive experience in breast reconstruction were selected, each of whom used a particular nipple reconstruction technique (skate flap, double-opposing-tab flap, or four petals) or the contralateral nipple graft. The indication for the use of such techniques was based on the inability to use the contralateral nipple (cases of small nipple or bilateral mastectomy) and on the personal experience of each surgeon; all surgeries for a given technique were performed by the same surgeon (skate flap, double-opposing-tab flap, or four petals) except for the contralateral nipple graft, which was performed by all three surgeons. Patients who underwent bilateral reconstruction were treated with the same surgical technique on both sides.
The results were evaluated through photographic documentation at various post-operative time points. This evaluation was made by a fourth plastic surgeon with experience in breast reconstruction who was blinded to the type of surgical technique used. He evaluated the photos according to certain criteria. In unilateral reconstruction cases, the similarity between the new nipple and the contralateral nipple (projection, base size) and the resulting natural appearance were assessed. In bilateral reconstruction cases, projection similarity and natural appearance (base wider than apex) were considered. Based on these criteria, the new nipple was classified as fully satisfactory (grade 3), satisfactory (grade 2), partially satisfactory (grade 1), or unsatisfactory (grade 0).
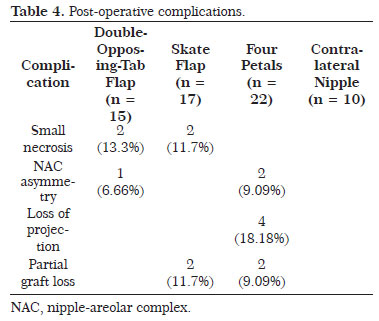
Data such as primary reconstruction type, laterality, comorbidities, and post-operative complications were collected during the medical records analysis.
The statistical evaluation of the results was performed using the Kruskal-Wallis test, and values of p<0.05 were considered significant.
RESULTS
Retrospective analysis of the medical records identified that 107 patients underwent a secondary breast reconstruction during the study period. Of them, only 53 met the inclusion criteria. The other 54 did not meet the inclusion criteria (having post-operative photo and good documentation in the medical records). The mean patient age was 48.11 years (Table 1).
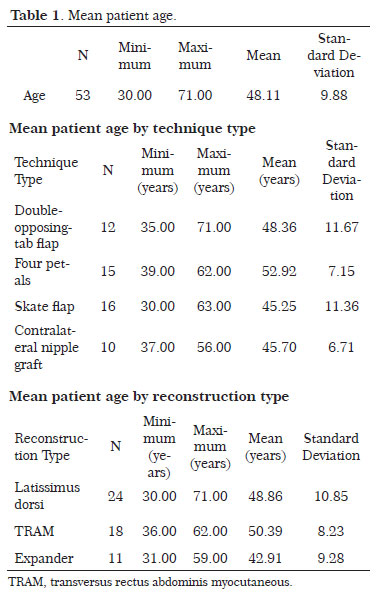
Forty-two unilateral nipple reconstructions and 11 bilateral reconstructions were performed for a total of 64 new nipples. Fifteen nipple reconstructions were performed using the double-opposing-tab flap technique, 17 were performed using the flap skate technique, 22 were performed using the four petals technique, and 10 were performed using the contralateral nipple graft technique.
Table 2 shows the post-operative evaluation results according to nipple reconstruction technique type. Analysis using the Kruskall-Wallis test (Figure 1) revealed that the contralateral nipple graft technique provided a greater number of fully satisfactory results (p = 0.012), while the other techniques had greater variation in post-operative assessment result. Compared to the techniques using flap reconstruction (excluding a contralateral nipple graft), no statistical difference was found among the groups in terms of the post-operative assessment result (p = 0.102).
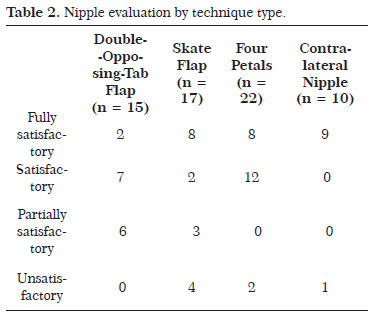
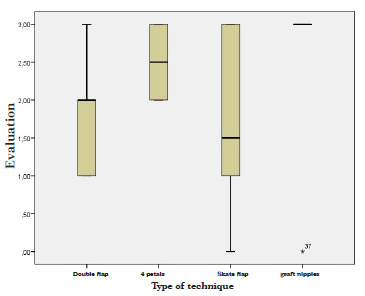
Figure 1. The contralateral nipple graft technique showed a greater number of fully satisfactory results (p = 0.012).
The most common primary reconstruction method involved the use of autologous tissue, mostly from the latissimus dorsi muscle (n = 31), followed by the use of transversus rectus abdominis myocutaneous flaps (n = 22) and the use of expanders (n = 11).
Table 3 compares the post-operative nipple evaluation results by primary breast reconstruction type. The Kruskall-Wallis test analysis demonstrated that all reconstruction types showed wide variation in terms of postoperative assessment with no significant difference (p = 0.563) (Figure 2).
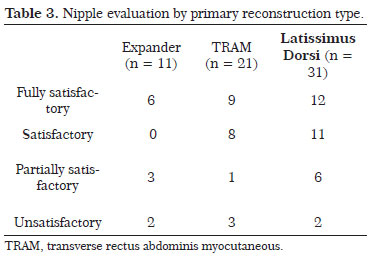
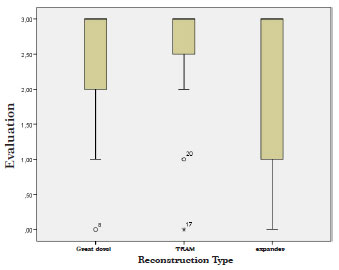
Figure 2. When only the flaps were evaluated, no difference was found among the techniques used (p = 0.102).
Figures 3-6 show the pre- and post-operative results for each of the techniques.
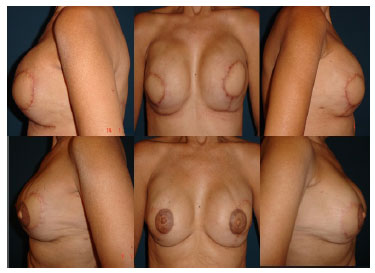
Figure 3. Double-opposing-tab flap technique.

Figure 4. Pre-operative and 3-month post-operative photos of flap skate technique results.

Figure 5. Pre- and post-operative photos of the four petals technique results.
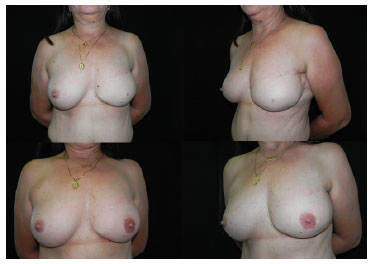
Figure 6. Pre- and post-operative photos of the contralateral nipple graft technique results.
DISCUSSION
The final appearance of the reconstructed nipple has an important emotional and aesthetic impact on breast reconstruction. Although this procedure is often considered to be minor by the patient, its results can affect the outcome of the entire breast reconstruction process17. Thus, perfectly reconstructed breasts may be considered aesthetically unacceptable in cases in which patients perceive the nipples as asymmetrical, flat, or unnatural in appearance17.
Loss of projection and a poor final nipple reconstruction result have a number of causes: small amount of subcutaneous tissue flaps, bad flap planning, natural wound-healing process, tissue memory, increased internal (strained sutures) or external (pressure applied by the use of a bra) pressure, infection, or prior radiation1,18. Thus, the main challenge is reconstructing a nipple while overcoming these local obstacles and natural tendencies18.
In the international literature, few prospective studies compare the various techniques for long-term nipple reconstruction, and none have evaluated contralateral nipple grafting. In Brazil, this work is the first to evaluate secondary breast reconstruction. In addition, most studies only evaluate the final nipple projection. It is not uncommon for nipple over-projection to occur during reconstruction since surgeons anticipate loss in projection18,19,20. Some precautions must be taken because distortions can occur in the final outcome and flatness of the breast outline can appear with the closure of the donor site, especially in the reconstruction of smaller breasts1. We believe that the beauty of breast reconstruction is based not only on the final nipple projection but in its natural appearance and the bilateral nipple similarity.
If shrinkage of the reconstructed nipple is significant and the final projection is insufficient compared with that on the contralateral side, refinements can be conducted within 12 months with extreme safety18.
In the present study, we observed better results in patients who underwent contralateral nipple grafting (p=0.012). This may be due to the ease of predicting loss of projection and asymmetry compared with other techniques. Furthermore, there is a tendency toward a low rate of complications at the donor site compared to that of local flaps, including distortions and flattening of the breast outline as mentioned above. However, not all patients are candidates for contralateral nipple grafts, particularly those with a small contralateral nipple or those who underwent bilateral mastectomy. Comparison of the flap techniques only (i.e., without contralateral nipple grafting) showed no significant difference among the various techniques (p=0.102). These data combined with the low complication rate of each technique indicate that each procedure is extremely safe and yields appropriate results; therefore, when the contralateral nipple grafting technique is not indicated, the surgeon should choose the technique with which they are the most familiar and feel the most confident performing.
In the literature, we found one article that evaluates nipple reconstruction according to the primary type performed (expander versus autologous tissue), and no change was observed in the resulting final nipple projection using the modified star, skate, and bell flap techniques1. Although the present study does not evaluate the same techniques, it showed no statistical difference among the techniques (p=0.563), which suggests that the nipple reconstruction result is more closely related to the type of technique used in the secondary reconstruction than to the type of donor area in the primary breast reconstruction.
The strength of this study is, in addition to its blind design, it is the first to compare three extremely common nipple reconstruction techniques with contralateral nipple grafting. This study's main disadvantage is the fact that we experienced great loss in the number of patients due to the lack of post-operative photos. Hence, further studies with larger samples are required to confirm the results reported here.
CONCLUSION
After comparing the four nipple reconstruction techniques used in secondary breast reconstruction, we noted that the contralateral nipple grafting was more effective with better post-operative results. We also found that the primary reconstruction method does not influence the final reconstructed nipple result. When the use of contralateral nipple grafting is not possible, the skate flap, double-opposing-tab flap, and four petals techniques are all safe alternatives.
REFERENCES
1. Shestak KC, Gabriel A, Landecker A, Peters S, Shestak A, Kim J. Assessment of Long-Term Nipple Projection: A comparison of three techniques. Plast Reconstr Surg. 2002;110(3):780-6.
2. Wilkins EG, Cederna PS, Lowery JC, et al. Prospective analysis of psychological outcomes in breast reconstruction: One Year post-operative results from the Michigan Breast Reconstruction Outcome Study. Plast Reconstr Surg. 2000;106:1014.
3. Yurek D, Farrar W, Andersen BL. Breast cancer surgery: Comparing surgical groups and determining individual differences in post-operative sexuality and body changes stress. J Consult Clin Psychol. 2000;68(4):697-709.
4. Little JW. Nipple - areolar reconstruction. In M. Cohen (Ed.) Mastery of Plastic and Reconstructive Surgery, Vol 2. Boston: Little, Brown, 1994.
5. Kroll SS. Integrated breast mound reduction and nipple reconstruction with the wraparound flap. Plast Reconstr Surg. 1999;104(3):687-93.
6. Wellisch DK, Schain WS, Noone RB, Little JW. The psychological contribution of nipple addition in breast reconstruction. Plast Reconstr Surg. 1987;80(5):699-704.
7. Bhatty MA, Berry RB. Nipple - areolar reconstruction by tattooing and nipple sharing. Br J Plast Surg. 1997;50(5):331-4.
8. Tanabe HY, Tai Y, Kiyokawa K, Yamauchi T. Nipple-areolar reconstruction with a dermal-fat flap and rolled auricular cartilage. Plast Reconstr Surg. 1997;100(2):431-8.
9. Lossing C, Brongo S, Holmstrom H. Nipple reconstruction with a modified S-flap technique. Scand. Scand J Plast Reconstr Surg Hand Surg. 1998;32(3):275-9.
10. Kroll SS, Reece GP, Miller MJ, et al. Comparison of nipple projection with the modified double - opposing tab and star flaps. Plast Reconstr Surg. 1997;99(6):1602-5.
11. Van Wingerden JJ. Nummular nipple hypertrophy and repair as part of an aesthetic nipple - areola unit. Aesthetic Plast Surg. 1997;21(6):408-11.
12. Eng JS. Bell Flap nipple reconstruction: A new wrinkle. Ann Plast Surg. 1996;36(5):485-8.
13. Thomas SV, Gellis MB, Pool R. Nipple reconstruction with a new local tissue flap. Plast Reconstr Surg. 1996;97(5):1053-6.
14. Eskenazi LA. One - stage nipple reconstruction with the "modified star" flap and immediate tattoo: A review of 100 cases. Plast Reconstr Surg. 1993;92(4):671-80.
15. Hugo NE, Sultan MR, Hardy SP. Nipple - areola reconstruction with intradermal tattoo and double-opposing pennant flaps. Ann Plast Surg. 1993;31(4):380.
16. Allison AB, Howorth MB. Carcinoma in a nipple preserved for heterotopic autotransplantation. N Engl J Med. 1978;298(20):1132.
17. Zhong T, Antony A, Cordeiro P. Outcomes and nipple projection using the modified skate flap for nipple - areolar reconstruction in a series of 422 implant reconstructions. Ann Plast Surg. 2009;62(5):591-5.
18. Nahabedian MY. Secondary nipple reconstruction using local flaps and AlloDerm. Plast Reconstr Surg. 2005;115(7):2056-61.
1. Full Member of the Brazilian Society of Plastic Surgery - Plastic Surgeon. Preceptor of the Plastic Surgery Service at the Daher Hospital in Lago Sul
2. Full Member of the Brazilian Society of Plastic Surgery - Plastic Surgeon. Director of the Plastic Surgery Service at the Military Hospital (HFA)-
3. Preceptor of the Plastic Surgery Service at the Daher Hospital in Lago Sul
4. Full Member of the Brazilian Society of Plastic Surgery - Plastic Surgeon. Preceptor of the Plastic Surgery Service at the Daher Hospital in Lago Sul
5. Full Member of the Brazilian Society of Plastic Surgery - Plastic Surgeon. Preceptor of the Plastic Surgery Service at the Daher Hospital in Lago Sul
6. Aspiring Member in training of the SBCP. Medical resident of the Plastic Surgery Service at the Hospital Daher Hospital in Lago Sul
7. Aspiring Member in training of the SBCP. Medical resident of the Plastic Surgery Service at the Hospital Daher Hospital in Lago Sul
8. Aspiring Member in training of the SBCP. Medical resident of the Plastic Surgery Service at the Hospital Daher Hospital in Lago Sul
Institution: Plastic Surgery Service at the Daher Hospital in Lago Sul.
Corresponding Author:
Rafael Quaresma de Lima
Daher Hospital in Lago Sul, SHIS QI 7, Conjunto F Lago Sul
Brasilia, DF, Brazil. Zip code: 71615-570
E-mail: rafaquaresma@gmail.com
Article submitted: February 7, 2014.
Article accepted: September 31, 2014.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket