



Original Article - Year 2014 - Volume 29 -
Patient profile and results evaluation after breast reduction
Perfil e avaliação dos resultados de pacientes submetidas à mamoplastia redutora
ABSTRACT
INTRODUCTION: In women, breast hypertrophy is a source of physical and emotional pain; several techniques have been described for its treatment.
OBJECTIVE: To demonstrate the appearance and satisfactory results obtained with reductive mammoplasty for the treatment of breast hypertrophy according to Bozola's classification.
METHOD: This descriptive and retrospective study included 94 patients who underwent reductive mammoplasty between January 2011 and October 2013. The patients were evaluated according to age, chief complaint, comorbidities, body mass index (BMI), history of pregnancy, presence of sagging skin, breast contour and consistency, tumors, and hypertrophy grade. The patients underwent reductive mammoplasty using the technique of Ariê and Peixoto with the type I pedicle of Ribeiro as well as Pitanguy's method. During the postoperative period, patient satisfaction was evaluated according to the outcomes observed and regarding breast symmetry, size, complications, and nipple-areola complex (NAC) sensitivity.
RESULTS: The average patient age was 28.5 years and the average BMI was 27.66. The main complaint was discomfort and pain (73.4%). The average weight of resected tissue was 952.5 g. The occurrence of complications was observed in 27.6% of patients. For the evaluation, form, symmetry and NAC sensitivity were considered. The satisfaction rate was great in 51.1% of cases and good in 35.1%.
CONCLUSION: The technique of Ariê and Peixoto as well as Pitanguy's method provided long-term results with durable breast support and enabled the design of a medial upper pole with more pronounced contours.
Keywords: Reductive mammoplasty; Breast hypertrophy; Complications; Satisfaction.
RESUMO
INTRODUÇÃO: A hipertrofia mamária é relatada como fonte de sofrimento físico e emocional em mulheres, sendo que diversas técnicas vêm sendo descritas para seu tratamento.
OBJETIVO: Demonstrar o perfil e resultados satisfatórios da mamoplastia redutora no tratamento de hipertrofias mamárias pela classificação de Bozola.
MÉTODO: Estudo descritivo e retrospectivo, com 94 pacientes submetidas àmamoplastia redutora, entre janeiro de 2011 e outubro de 2013, avaliadas segundo idade, queixa principal, comorbidades, índice de massa corporal (IMC), maternidade prévia, flacidez de pele, contorno e consistência mamária, tumorações, graus de hipertrofia submetidas à mamoplastia com a técnica de Ariê e Peixoto, com pedículo I de Lyacir Ribeiro, e a técnica de Pitanguy. No pós-operatório as pacientes foram avaliadas quanto à satisfação dos resultados observados pela simetria das mamas, tamanho, complicações e sensibilidade do complexo areolopapilar (CAP).
RESULTADOS: A média de idade das pacientes foi de 28,5 anos e IMC médio de 27,66. A principal queixa foi de desconforto e quadro doloroso em 73,4%. Média de tecido total ressecado foi de 952,5 g. Foi evidenciado taxa de complicação em 27,6%. O avaliador considerou forma, simetria e sensibilidade do CAP. A satisfação, quanto ao procedimento, foi evidenciada como ótima em 51,1% dos casos, e boa em 35,1%.
CONCLUSÃO: As técnicas de Ariê e Peixoto, com pedículo inferior, e de Pitanguy promoveram resultados duradouros com maior prazo de sustentação da mama, além de um polo superior medial desenhado com curvas mais acentuadas.
Palavras-chave: Mamoplastia redutora; Hipertrofia mamária; Complicações; Satisfação.
The concept of ideal beauty changes over time. Brazilian literature is rich in descriptions and details reporting the adoration for female curves, which vary from more pronounced to thinner and symmetrical shapes. Social networks and global connections encourage the search for perfection, thus explaining the increased demand for cosmetic surgery procedures, among which mammoplasty is one of the most common1.
The physical changes induced by breast hypertrophy stigmatize women and, as such, are quickly detected even before a patient sits in the physician's office. Women with large and hypertrophic breasts may have dorsal kyphosis caused by moving their shoulders forward to compensate for high breast weight, or even social withdrawal, which varies by hypertrophy grade. Over time, these deformities result in pain and dermatological complaints involving trauma caused by high-pressure friction2.
Counseling a patient who is interested in this procedure requires the understanding of terms commonly used in conferences and coined by talented experts in morphology and breast anatomy in terms of container and content. Palpation and geometric conclusions are closely related to breast examination and how they appear at inspection (in the standing and sitting positions as well as with the arms raised). Systematization in breast care facilitates correct diagnosis and surgical indication. Routine preoperative examinations and opinions of the Gynecology/Mastology and Cardiology Service are essential to ensuring proper monitoring during the intra- and postoperative periods3.
From a histological point of view, mammary acini (15-20 units) are radially arranged interspersed by bundles of connective tissue. These are contained and suspended along the thoracic fascia due to the thickening of these bundles (Cooper's ligaments). The stroma, formed by this connective tissue, surrounds each lobe, whereas the adipose tissue is responsible for breast volume, size, and shape in the different stages of life, such as puberty, pregnancy, and menopause. Stromal composition was classified by Galtier as pure or true glandular hypertrophy in puberty; glandular and fat hypertrophy (mixed), which is observed especially after pregnancy (lactation); and pure or false adipose hypertrophy, which is related to pre-menopausal patients in whom hormonal change and reduced hormone levels are already present3.
According to breast hypertrophy grade, skin and ligament elasticity are pushed to the limit, thus leading to the occurrence of stretch marks in the most sensitive skins (flaccid) and consequent breast falling, characterized by ptosis, a Greek word that means to fall4.
Several grades have been described in an attempt to establish the most appropriate breast position, although this relies upon surgeon experience or the specific clinical situations presented by each patient. According to grade, it was noticed that some analyses change with breast unevenness but not with patient height5. This study was performed according to Bozola's classification6 and assessed breast shape and volume by using points A and M as reference. The inframammary fold was used as the reference point to determine the presence but not degree of ptosis. During surgery, the team considered placing the nipple 2-4 centimeters above Point A.
Using the distance between the inframammary crease and the inferior edge of the breast, Bozola6 classified breast hypertrophy in grades of breast ptosis (Chart 1). This score is based on the distance between the anterior projection of the breast inframammary crease and the most distal point from the inferior edge of the breast, lines A-M (Figure 1).
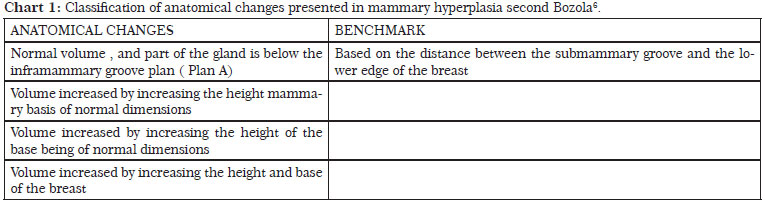
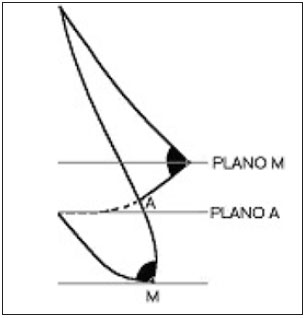
Figure 1. Scale of Bozola.6 Source: Souza,5 page 70.
Analysis of the results obtained in this study requires a good knowledge of embryology and breast histology since these principles ultimately determined the evolution of personal mammoplasty techniques without skin detachment. A strong knowledge of anatomy provides valuable information on the main arterial routes; the internal mammary, lateral thoracic, and intercostal perforating. The veins running the arterial route form anastomosis around the base of the mammary papilla and, deriving also from the gland, converge into the axillary veins, internal thoracic, and azygos circulating system. The lymphatic vessels are on the skin and areola, although the drainage systems of these structures do not coincide. Innervation is provided by the supraclavicular and intercostal perforating branches3.
With these basic notions, large resections can be performed without damaging nerve branches such as the lateral cutaneous or impairing the mammary irrigation and venous drainage. Therefore, good nipple and areola sensitivity is ensured, which is confirmed by patient satisfaction rates of the service. Regarding the surgical technique, a defensive posture is assumed during preservation of the flap tissues to minimize physiological disturbances due to the removal of adjacent regions.
To better understand the surgical technique used in this study, we must trace back the history of breast plastic surgery to 1957, when Ariê published a technique for correcting breast ptosis7. In this procedure, using the Schwarzmann maneuver of decortication8, wedge-shaped infra-areolar excision and periaerolar complex transposition are performed while consideration of surgical marks being performed using the bidigital skin approach to set the edges of the incision and establish the point for areolar fixation.
Three years later, in 1959, Pitanguy reported good results using the technique of Ariê, especially in the treatment of small degrees of ptosis and hypertrophy with some modifications. In 1961, he described the technique of mammoplasty with infra-areolar cutaneous-fat-glandular removal without skin detachment as well as positioning the nipple-areola complex (NAC) at the apex of the cone obtained after the assembly, a procedure commonly used to correct several types of breast ptosis and hypertrophy3,9.
In 1973, Ribeiro and Backer10 published the use of a deepithelized flap 4-5 inches wide that was positioned between the areola and the inframammary crease with the distal pedicle at the level of the crease itself, which is introduced and fixed between the gland and the fascia of the pectoralis major muscle. By the end of the 1970s, great advances has been described in the literature that consisted of small skin excisions, even with large glandular removal, that finally results in an inverted "T" with the horizontal branch in the inframammary crease based on the ability of the skin to contract and re-adapt to surround the reduced content (glandular excision is carried out on the dorsal part of the gland along with the pectoralis major muscle).
After the procedure and in the immediate postoperative period, the patient is followed up with small-caliber portovac suction drainage and micropore dressing and breast elevation and support are maintained. Padded molders with extensive cotton-filled gauze are placed before the patient is transferred to anesthesia recovery. After 24 hours, the physician examines and removes the drain. The patient is then discharged with a hypoallergenic simple micropore, which should be maintained for 60 days and changed during weekly outpatient visits. Moisturizing of the skin, but not the wound itself, with cream is recommended. Only a few low-amplitude movements of the upper limbs are allowed for the first 30 days, while carrying heavier weight is allowed only after 45 days. Events and complications are monitored and treated closely with more frequent returns that aim to obtain better outcomes and satisfaction rates.
OBJECTIVE
The aim of this study is to demonstrate patient profiles and satisfaction with the treatment of different degrees of breast ptosis and hypertrophy performed with the technique of Ariê7 and Peixoto11 as well as the type I pedicle of Ribeiro12.
METHOD
This retrospective descriptive study analyzed data collected from a review of the medical records of patients undergoing reconstructive mammoplasty for presenting breast hypertrophy. A total of 94 patients were evaluated for comparative and observational effects during the pre- and postoperative periods.
The study evaluated the procedures performed by last-year residents at the Plastic Surgery and Burns Service of the Santa Casa de Misericórdia de São José do Rio Preto. The evaluated criteria included chief complaint, comorbidities (hypertension and diabetes mellitus), body mass index (BMI), prior history of pregnancy, presence of sagging skin, breast consistency and contour, tumors, and degree of hypertrophy (breast ptosis).
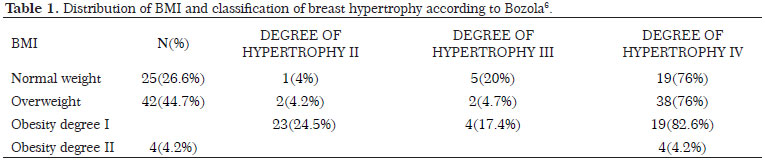
The patients underwent mammoplasty with the technique of Ariê7 and Peixoto11 and using the type I pedicle of Ribeiro12 (Figure 2) as well as the technique of Pitanguy9 (Figure 3) to correct various grades of hypertrophy and ptosis according to the classification proposed by Bozola6 (Table 1).
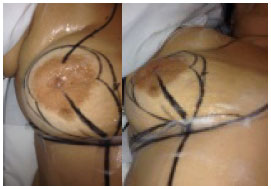
Figure 2. Technique of Ariê for correcting breast ptosis using the maneuver of Schwarzmann8 for decortication, wedge-shaped infraareolar excision, and transposition of the periaerolar complex. The surgical marks were made using a bidigital cutaneous approach to set the limits of the incision and establish the point of areolar fixation.

Figure 3. Pitanguy technique - Breast with dermoadiposa -glandular excision infra areola without detachment of the skin , positioning the CAP in the cone apex obtained after assembly with broad indication to various types of ptosis and breast enlargement.
During the postoperative period, the patients were evaluated for their satisfaction of the procedural outcomes. The following were considering in the analysis: breast symmetry, size, and location according to the researcher; the occurrence of complications (epidermolysis, dehiscence, infection, and secretion/seroma); and NAC sensitivity according to the patients.
This information was processed using Excel® (Microsoft) and the results and summary of absolute numbers and percentages were analyzed by calculating the average, standard deviation, and χ2 presented in numerical order and tables for better interpretation.
RESULTS
The main aim of the study was to compare the body contour improvements of patients who underwent reductive mammoplasty. A total of 94 medical records of female patients who underwent this surgical procedure were analyzed between January 2011 and October 2013.
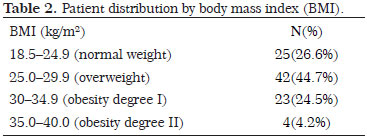
The average patient age was 28.5 ± 10.6 years (range, 15-65 years). The correlation between age and pregnancy demonstrated that it can be used as parameter for breast consistency. The totality of glandular breasts was observed in a group of adolescent patients without a prior history of pregnancy and but with hormonal changes. The average age of these patients was 20.7 ± 10.8 years, while their average BMI was 27.66 ± 3.06 kg/m2 (range, 19.14-36.28 kg/m2) (Table 2).
The chief complaint reported by most patients (69 patients; 73.4%) was pain and discomfort caused by excess breast weight, postural deviations, and dermatitis of the inframammary crease. Moreover, two patients (2.1%) presented with injuries on their shoulders due to bra use. Aesthetic complaints caused by large breasts and ptosis were reported by 23 patients (24.5%). Of these, an association between physical dissatisfaction and pain was observed in two patients (13%).
Comorbidities were observed in 15 (15.9%) patients, of whom 10 (10.6%) had arterial hypertension, two (2.1%) had diabetes mellitus, and thee (3.2%) had both.
The technique of Ariê7 and Peixoto11 was used in 82 (87.2%) cases and Pitanguy's9 technique was used in 12 (12.8%). Both techniques were employed to resect > 1000 g of tissue and provided great postoperative results.
The average total resected volume was 410 ± 40.0 g in 7.3%, 739.2 ± 101.3 g in 45.4%, and 1,241.1 ± 217.5 in 47.3% of patients (Table 3).

Complications in the postoperative period occurred in 26 (27.6%) cases, while epidermolysis was detected in 12 (12.7%) patients. Complications evolving into small wounds occurred in 14 (14.9%) patients and 12 (12.7%) patients at the wound vertex closure. Dehiscence along the scar was detected in five (5.3%) patients, infection occurred in two (2.1%), and dehiscence and infection with seroma occurred in three (3.2%). It is important to emphasize that infections detected when patients develop dehiscence may involve the dermal tissue that may suffer trauma or excessive tension, which results in the inability to keep the edges of the surgical wound closed.
Complications such as asymmetry, slowed healing, and reduced NAC sensitivity influence patients' satisfaction ratings. Pre- and postoperative symmetry were evaluated by the observer, who compared the images taken before and after surgery and assessed NAC sensitivity as reported by the patients. The satisfaction rate was also assessed. To evaluate the quality of the obtained results, pre- and postoperative photographs of the 94 patients were analyzed. Images of representative patients are shown in this study. These patients presented with different hypertrophy grades according to the classification of Bozola6 and the postoperative period was reported for the techniques used in the different age groups (Figures 4A and 4B to Figures 14A to 14B).

Figure 4. Pre- (A) and postoperative (B) images of ACAC, an 18-year-old patient with a body mass index of 33. The patient presented with breasts of mixed consistency, grade IV hypertrophy, marked lateralization of the nipple-areola complex (NAC), and no tumors or comorbidities. Postoperative evaluation revealed a small wound outside the vertex without dehiscence that evolved with good healing. NAC medialization and resection of 1,290 g of cutaneous-fat glandular tissue was performed. The patient reported good procedural satisfaction.

Figure 5. Pre - (A) and postoperative (B) images of MESN, a 17-year-old patient with low self-esteem due to grade IV breast hypertrophy despite a body mass index of 27. She presented with breast glandular consistency but no major asymmetry or tumors. The technique of Ariê was used and resulted in perfect healing. The patient reported great procedural satisfaction but a slightly decreased nipple-areola complex sensitivity.
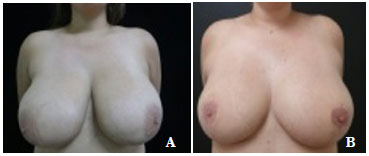
Figure 6. Pre - (A) and postoperative (B) images of DAMS, a 19-year-old patient with grade IV hypertrophy, slight asymmetry, no tumors or comorbidities, and a body mass index of 25. A total of 1,500 g of breast content was resected and the postoperative course was good. However, the patient reported unilateral nipple-areola insensitivity of the right breast and she still had large breasts. The patient's great procedural satisfaction is reflected in the remarkably beautiful healing.

Figure 7. Pre - (A) and postoperative (B) images of OAS, a 59-year-old patient with visible breast asymmetry and grade IV hypertrophy but no diagnosis of tumors. The patient was treated for hypertension and had a body mass index of 24. She underwent the technique of Pitanguy with rounded curves as described by Castro. Good results and symmetrical nipple-areola complex sensitivity were expected with this technique. The patient reported great procedural satisfaction with perfect healing despite reduced mammary asymmetry and the presence of a small wound outside the vertices of the wound observed during the first few postoperative days.

Figure 8. Pre- (A) and postoperative (B) images of ILB, a 65-year-old patient with giant breasts in base and height who was treated for arterial hypertension and presented with shoulder lesions, a body mass index of 30, and a fatty breast consistency. Reductive mammoplasty was performed according to the technique of Pitanguy. The patient reported great procedural satisfaction despite maintenance of the large breast size as well as symmetrical preservation of the nipple-areola complex sensitivity.
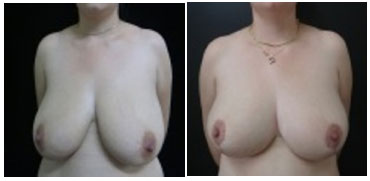
Figure 9. Pre- (A) and postoperative (B) images of SBS, a 26-year-old patient with sagging skin, fatty breast consistency, noticeable asymmetry, no tumors, and a body mass index of 22. The patient underwent breast reduction according to the technique of Ariê with the type I pedicle of Ribeiro and recovered well despite a wound on the vertex that developed dehiscence and an infection that was treated with antibiotics and resolved satisfactorily and did not influence the patient's reported good procedural satisfaction.

Figure 10. Pre- (A) and postoperative (B) images of GF, a 24-year-old patient with normal skin without stretch marks, low self-esteem, asymmetry, and glandular breast consistency. The patient underwent breast reduction using to the technique of Ariê with an inferior pedicle that resulted in good symmetry, great personal satisfaction, and perfect healing without postoperative complications.

Figure 11. Pre- (A) and postoperative (B) images of AHO, a 33-year-old Patient with grade IV hypertrophic and asymmetrical breasts, a body mass index of 31, and no breast tumors or comorbidities. The patient reported the best score of personal satisfaction for reductive mammoplasty, the results of which were not expected, despite the maintenance of asymmetry and decreased nipple-areola complex sensitivity. The healing occurred perfectly and there were no postoperative complications.

Figure 12. Pre- (A) and postoperative (B) images of OSC, a 34-year-old patient with no comorbidities who presented with grade IV hypertrophic breasts and a body mass index of 31. She reported great procedural satisfaction despite decreased nipple-areola complex sensitivity and slight asymmetry.

Figure 13. Pre- (A) and postoperative (B) images of PSB, a 42-year-old patient with grade IV hypertrophy, breast tissue of mixed consistency, and a body mass index of 29. Excellent postoperative symmetry was noted; however, the patient reported average procedural satisfaction due to the maintenance of large breast size.

Figure 14. Pre- (A) and postoperative (B) images of CAVO, a 48-year-old patient complaining of breast asymmetry with fatty breast consistency, grade IV hypertrophy, and no comorbidities or tumors. After the resection of 600 g of breast tissue, the patient presented with good healing and symmetry and reported great procedural satisfaction.
Preoperatively, asymmetry was observed in 78 (83%) breasts; of them, 53 (67.9%) were symmetrical after surgery. Only one case of preoperative symmetry resulted in postoperative asymmetry.
Healing was considered perfect in 36 (38.3%) cases, acceptable in 18 (19.1%), apparent in 39 (41.5%), and unacceptable in one (1.1%). NAC sensitivity was normal in most (59.6%) cases, reduced in 33 (35.1%), and absent in four (4.3%). Only one patient (1.1%) reported NAC pain (1.1%). Most patients reported great procedural satisfaction (51.1%), 33 (35.1%) good, 11 (11.7%) average, and two (2.1%) poor.
DISCUSSION
In women, breast hypertrophy is a source of physical and emotional pain, and several techniques have been described for its treatment13. According to Fernandes and Freitas14, reductive mammoplasty is performed mainly for dysfunction and/or the unsightly appearance of large breasts or those with ptosis. The aim of this surgery is to reduce breast size, maintain symmetry, and incur minimal complications.
The average patient age in this study was 28.5 ± 10.6 years (range, 15-65 years). However age is not a parameter of interest in the procedure since it is also performed in young patients still in puberty (11.7%) and elderly patients with giant breasts (2.1%). Therefore, the age range in this study was wide. Studies published by Costa Sobrinho et al.13 reported an average age of 32.9 ± 10.6 years (range, 16-61 years), whereas Ronconiet al.15 reported an average age of 32.5 years (range, 13-60 years) that confirms the data presented here.
The average BMI of the patients in this study was 27.66 ± 3.06 kg/m2, which is not used as standard analysis parameter for breast hypertrophy graduations or ptosis since patients with different BMI have distinct breast hypertrophy grades as reported by Ronconi et al.15, whose patients had an average BMI of 27.3 ± 2.9 kg/m2.
Age and pregnancy seem to be directly related to breast consistency since glandular breasts were observed in young patients without prior pregnancy history who still are in hormonal development.
Physical discomfort due to breast weight, back pain, shoulder strain, bad posture, dorsal kyphosis, lumbar lordosis, shoulder fold or marks caused by bra straps, and dermatitis in the inframammary groove are reported as functional changes induced by breast hypertrophy. Most of these patients sought surgical correction15, and the complaints above are the leading causes of reductive mammoplasty requests, as in this study.
In several studies, the technique of choice varies by surgeon experience and service protocol. The two techniques used in this study showed satisfactory results13. Choosing the technique of Pitanguy9 as a reconstructive procedure was also reported in another study16. The choice of using both techniques was made in cases of the resection of large amounts of breast content to increase the odds of satisfactory results. The average tissue resected in the study published by Ronconiet al.15 was 800 g per patient, whereas that in this study was 950 g.
Unsightly scars, discrete asymmetry, and hematoma were complications reported by Fischler and Sperli17 without the occurrence of infection or changes in NAC sensitivity. In this study, we observed epidermolysis and the presence of small wounds at the wound vertex closure with or without dehiscence along the scar or infection. Among the main complications observed in the studies published by Fernandes et al.14 were changes in NAC sensitivity, unsightly scars, and postoperative mastodynia. The main challenge of very large breasts is maintaining the pedicle vascularizing the NAC. Fortunately, normal NAC sensitivity was reported by most patients in this study.
A retrospective study demonstrated that late complications or sequelae involving changes in NAC sensitivity or position as well as breast asymmetry were observed in 16% of cases15. However, high satisfaction was reported by the vast majority of patients (85%) and the results varied between good and optimal. Another study reported that 88% of patients were satisfied16, similar to the results obtained in the evaluations of Cho et al.18 and Rohrich et al. 19 and consistent with the results of the current study.
The results obtained in this study reveal a positive analysis of patients with respect to final breast volume and symmetry. The degree of satisfaction varied between good and optimal in 86.2% of cases, while NAC sensitivity was normal in most cases.
Ferreira20 defined mastoplasty as plastic surgery of the breasts. Two mastoplasty procedures are most commonly used: augmentation (usually with silicone prostheses) and reductive mastoplasty. Patients seek surgery to reduce breast size and, therefore, eliminate symptoms (back pain, shoulder strain, intertrigo, and discomfort, among others) and/or improve their aesthetic appearance. Therefore, the results can be evaluated with objective criteria - particularly, the elimination of symptoms - although surgery can also be performed for aesthetic and personal reasons.
CONCLUSION
We can conclude that the technique of Ariê7 and Peixoto11, with the inferior pedicle, as well as Pitanguy's9 method, provides long-lasting results and confers long-term breast support in addition to the design of a medial upper pole with more pronounced contours. The resection of large amounts of cutaneous-fat glandular tissue results in almost emptying of the breast, especially when a patient presents with high-grade hypertrophy, and the substantial loss of tissue is then missed during breast re-assembly. The actual truth is revealed over time, as the breast bascule fills asymmetries and small retractions. In summary, the rate of patient satisfaction regardless of the technique used relies on the scar appearance, which was considered the main parameter here, followed by breast form and contour.
REFERENCES
1. Moceline PR, Martins OJ, Brito LM, Souza RD, Pinheiro GL. Hipertrofia de mama: estudo comparativo dos achados histopatológicos e de imagem. Rev Pesq Saúde. 2012;13(1):50-4.
2. Sperli AE. Mastoplastias estéticas enlasptosis: el limite entre el uso de lassiliconas y lasmastopexias. Rev Arg C Estética. 1977;2(2):93-8.
3. Melega JM, Viterbo F, Mendes FH. Cirurgia plástica: princípios e atualidades. Rio de Janeiro: Guanabara Koogan. 2011.
4. Castro ML. Aspectos atuais do tratamento das hipertrofias mamárias. J Bras Gin. 1997;83(5):241-57.
5. Souza SC. Graduações de ptose mamária. Arq Catarin Med. 2008;37(3):66-71.
6. Bozola AR. Breast reduction with short L scar. Plást Reconstr Surg. 1990;85(5):728-38.
7. Ariè G. Nova técnica em mamoplastia. Rev Lat Amer Cir Plást. 1975;3-28.
8. Schwartzman E. Die technik der mammaplastick. Chirurgie. 1930;2:932-43.
9. Pitanguy I. Mamaplastia. 1. Ed. Rio de Janeiro: Guanabara Koogan; 1978.
10. Ribeiro L, Backer E. Mastoplastia com pedìculo de seguridad. Rev Esp Cir Plást. 1973;16:223-34.
11. Peixoto G. Reduction mammaplasty: a personal technique. Plást Reconstr Surg. 1980;65(2):217-26.
12. Ribeiro L. Cirurgia plástica de mama. Redução mamária. Rio de Janeiro: Medsi; 1989.
13. Costa Sobrinho JB, Portocarrero ML, Portocarrero ML, Campos JH. Avaliação da técnica de mastologia redutora com cicatriz em "L" nas hipertrofias mamárias. Rev Bras Cir Plást. 2011;27(4):562-8.
14. Fernandes THA, Freitas JOG, Sperli AE. Estudo de alterações de sensibilidade do complexo areolopapilar após mamoplastias com a técnica de retalhos cruzados. Rev Bras Cir Plást. 2012;27(4):73-6.
15. Ronconi RC, Vieira FA, Boechat CE, Nunes PS, Aboudib JH, Castro CC. Estudo retrospectivo de 730 pacientes submetidas a mamaplastia redutora. Rev Soc Bras Cir Plást. 2004;19(2):58-62.
16. Aboudib JH, Roxo AC. Avaliação dos resultados tardios de mamoplastia redutora. Rev Bras Cir Plást. 2011;26(1):74-80.
17. Fischler R, Sperli A. Mastoplastia pela técnica dos retalhos cruzados: reavaliação de técnica. Rev Bras Cir Plást. 2008;23(3):173-8.
18. Cho BC, Yang JD, Baik BS. Periareolar reduction mammaplasty using an inferior dermal pedicle or a central pedicle. J Plást Reconstr Aesthet Surg. 2008;61(3):275-81.
19. Rohrich RJ, Gosmann AA, Brown SA, Reisch J. Mastopexy references: a survey of board-certified plastic surgeons. Plást Reconst Surg. 2006;118(7):1631-8.
20. Ferreira MC. Cirurgia plástica estética-avaliação de resultados. Rev Soc Bras Cir Plást. 2000;15(1):55-66.
1. Physician - Resident at the Plastic Surgery Service of the Santa Casa de Misericórdia de São José do Rio Preto, SP, Brazil
2. Specialist Physician - Preceptor of the Plastic Surgery and Burns Service of the Santa Casa de Misericórdia de São José do Rio Preto, SP, Brazil
3. Specialist Physician - Preceptor of the Plastic Surgery and Burns Service of the Santa Casa de Misericórdia de São José do Rio Preto, SP, Brazil
4. Specialist Physician and Titular Member - Regent of the Plastic Surgery and Burns Service of the Santa Casa de Misericórdia de São José do Rio Preto, SP, Brazil
Institution: Plastic Surgery and Burns Service of the Santa Casa de Misericórdia de São José do Rio Preto, SP, Brazil.
Corresponding author:
Raul Marinho Corrêa
Rua T, 30 - Quadra 70 - Lote 18 - Setor Bueno
Goiânia, GO, Brazil Zip code: 74215-060
E-mail: raulmarinhocorrea@hotmail.com
Article submitted: January 14, 2014.
Article accepted: January 25, 2014.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket