



Original Article - Year 2014 - Volume 29 -
Mandibular distraction osteogenesis: experience of the INTO-RJ
Distracção osteogênica mandibular: experiência do INTO-RJ
ABSTRACT
INTRODUCTION: The introduction of distraction of the craniofacial skeleton represented a great advancement in the practice of craniofacial surgery. Distraction is a less invasive technique that is faster and with an apparently lower morbidity than the traditional craniofacial reconstruction techniques. In 2013, the craniomaxillofacial surgery service of the Institute of Traumatology and Orthopaedics performed a series of mandibular distraction surgeries. In this article, we aim to present our experience.
METHODS: From January to March 2013, seven patients underwent mandibular distraction surgery. All patients exhibited unilateral or bilateral mandibular hypoplasia due to ankylosis of the temporomandibular joint (TMJ), or craniofacial microsomia. In some patients with ankylosis of the TMJ, resection of the anlylotic block was also performed concomitantly with the distraction.
RESULTS: Postoperative improvement was noted in all the stomatognathic functions: weight gain, decannulation of a tracheostomized patient, and improved quality of sleep. There was an improvement in facial profiles: the laterognathism was eased and the mouth opening increased in most patients. The mouth opening increased more significantly in patients in whom ankylosis surgery was done in conjunction with the distraction. The most common complication was pain upon distraction, reported by five patients (71%).
CONCLUSION: Mandibular distraction osteogenesis is a good alternative for the treatment of mandibular hypoplasia, often being the first indication in some clinical situations. It apparently has a lower morbidity than the classic mandible reconstructions and has the added benefit of also lengthening the soft tissues.
Keywords: Distraction osteogenesis; Distraction; Mandibular hypoplasia; Mandible; Ankylosis; TMJ ankylosis.
RESUMO
INTRODUÇÃO: O desenvolvimento das técnicas de distracção do esqueleto craniofacial representou um grande avanço na prática da cirurgia cranio-facial. A distracção é uma técnica menos invasiva, mais rápida e com uma morbidade aparentemente menor comparada com as técnicas tradicionais de reconstrução craniofacial. No ano de 2013, o serviço de Cirurgia Crânio Maxilo Facial do INTO realizou uma série de casos de distracção mandibular. Este trabalho objetiva apresentar nossa experiência.
MÉTODOS: De janeiro a março de 2013, sete pacientes realizaram cirurgia de distracção mandibular. Todos os pacientes operados apresentavam hipoplasia mandibular uni ou bilateral em decorrência de anquilose de ATM ou microssomia craniofacial. Em alguns pacientes com anquilose de ATM foi realizada também a ressecção do bloco anquilótico no mesmo tempo da distracção.
RESULTADOS: No pós-operatório houve melhora de todas as funções estomatognáticas, ganho de peso, decanulação da paciente traqueostomizada e melhora na qualidade do sono. Houve melhora nos perfis faciais, as laterognatias foram amenizadas e a abertura oral aumentou na maioria dos pacientes. A abertura oral aumentou de maneira mais significativa naqueles pacientes onde a cirurgia de anquilose foi realizada em conjunto com a distracção. A complicação mais comum foi dor à ativação, relato de cinco pacientes (71%).
CONCLUSÃO: A distracção osteogênica da mandíbula é uma boa alternativa para o tratamento das hipoplasias mandibulares, muitas vezes sendo a primeira indicação em algumas situações clínicas. Aparentemente tem morbidade menor do que as reconstruções clássicas de mandíbula e possui o bônus de alongar também os tecidos moles.
Palavras-chave: Distracção osteogênica; Distracção; Hipoplasia mandibular; Mandíbula; Anquilose; Anquilose de ATM.
The introduction of the technique of distraction of the craniofacial skeleton represented a great advancement in the practice of craniofacial surgery. Distraction is a less invasive, faster technique with an apparently lower morbidity than the traditional craniofacial reconstruction methods. It allows the surgeon to promote the formation of bone tissue instead of having to add grafts or free flaps harvested from other areas of the body1, 2.
Osteogenic distraction has become a widely accepted technique for the reconstruction of hypoplastic mandibles since the publication of McCarthy et al.1 in 1992, and Molina et al.3 in 1995. Distraction has been considered as the technique of choice in many clinical situations owing to the relative safety of the procedure, reduced hospitalization duration, low requirement for blood transfusions, and elimination of the need to harvest bone grafts, in addition to the desired expansion of soft tissues that occurs concomitantly with local bone formation4. Finally, mandibular distraction can improve not only the appearance of the face but also the airways of these patients5.
Mandibular distraction may be a treatment option for several facial deformities, such as hemifacial microsomia, Goldenhar syndrome, Pierre Robin syndrome, temporomandibular joint (TMJ) ankylosis, Treacher Collins syndrome, Nager syndrome, posttraumatic disabilities, obstructive sleep apnea, and mandibular hypoplasia class II1,5.
In 2013, the craniomaxillofacial surgery service of the National Institute of Traumatology and Orthopaedics (INTO) performed a series of mandibular distraction surgeries.
OBJECTIVE
In this work, we aim to present and evaluate our results, and compare them with the results of other services.
METHOD
From January to March 2013, seven patients underwent mandibular distraction surgery in the INTO. All patients who underwent surgery exhibited unilateral or bilateral mandibular hypoplasia due to TMJ ankylosis or craniofacial microsomia. In some patients with TMJ ankylosis, resection of the ankylotic block was also performed concomitantly with the distraction.
All these patients, from the preoperative period to date, were monitored by a multidisciplinary team including craniomaxillofacial surgeons, oral and maxillofacial surgeons, speech therapists, nurses, psychologists, nutritionists, and social workers. Radiological examinations (panoramic dental radiography, antero-posterior cephalometry, and profile cephalometry) were performed before and after surgery.
Surgical Technique1
With the patient anesthetized and intubated (oro- or nasotracheal intubation), the basilar line of the mandible and the vector of the distraction are marked. Depending on the characteristics of the patient, an external or an internal distractor is used6-12. In patients who need a unidirectional elongation and have a good amount of mandibular bone tissue, internal distractors are used. In patients who need an elongation in more than one vector and/or have little amount of mandibular bone, external distractors are used. The surgical access is created either with an extra-oral submandibular (Risdon) incision or with an intra-oral incision along the oblique line of the ramus of the mandible1,3-6. The preference of the surgeon is an important factor in the decision of the surgical access. In any event, in the case of an external distractor, there should be an externalization through the skin of four retaining pins that will "cut" the skin during the activation phase; in the case of an internal distractor, there should be a punctiform incision on the skin to allow passage of the trocar during the mounting of the distractor and the passage through the skin of a single pin that will be used to activate the internal mechanism. The exposure of the mandibular ramus (the osteotomy site) is performed through the subperiosteal detachment of this whole area. Of course, if the intention is a mandibular body distraction, the body will be exposed in the same way. After exposure, a reciprocating saw is used to perform lateral, anterior, and posterior corticotomy of the mandibular ramus. The direction of these corticotomies is defined by the desired distraction vector, taking into account the patient's mandibular deficiency and the presence of possible dental bacteria in the path. The choice of the distraction vector is a critical decision. Before converting corticotomies in a de facto osteotomy by performing a medial corticotomy, the distractor mechanism is installed on the mandibular ramus. In case of an external distractor, four percutaneous pins are fixed to the bone that will engage the distractor, which will be outside of the body; in the case of internal distractors, two clamping plates that are crossed by two pins are placed, one of which passes through the skin and is responsible for the activation of the system. Once the distractors are installed, the osteotomy is completed with an osteotome, a medial corticotomy is performed, and the mandibular segment for distraction is released. Before closing, the distraction mechanism is tested to confirm its proper functioning.
RESULTS
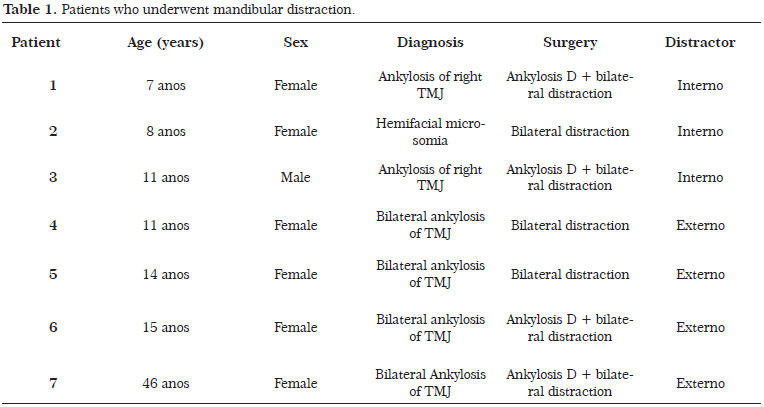
From January to March 2013, seven patients were operated for mandibular distraction in the INTO. Their age ranged from 7 to 46 years (mean age, 16 years). Six patients (86%) were female and only one (14%) was male. The most common etiology of mandibular hypoplasia and, consequently, facial asymmetry, was bilateral TMJ ankylosis (four patients), followed by unilateral TMJ ankylosis (two patients), and craniofacial microsomia (one patient). Of the six patients with TMJ ankylosis, four (66%) underwent unilateral resection of the ankylotic block concomitantly with distraction and five (83%) had a previous surgical treatment for ankylosis, including one with an unsuccessful attempt of bilateral distraction.
All distractors placed were bilateral and applied in native bone. That is, there was no case of distraction of a bone segment grafted beforehand. The osteotomy used in all cases was oblique/angle of the ramus. Four patients (57%) received external distractors (Figure 1), and three (43%) received internal distractors (Figure 2) (Table 1).

Figure 1. Patient 5: carrier of bilateral temporomandibular joint ankylosis submitted to bilateral distraction with external distractors (preoperative period and consolidation phase). There was a slight hypercorrection.

Figure 2. Patient 1 Carrier ATM D ankylosis surgical approach of bilateral ankylosis + distraction with internal distractors preoperatively and already in the consolidation phase.
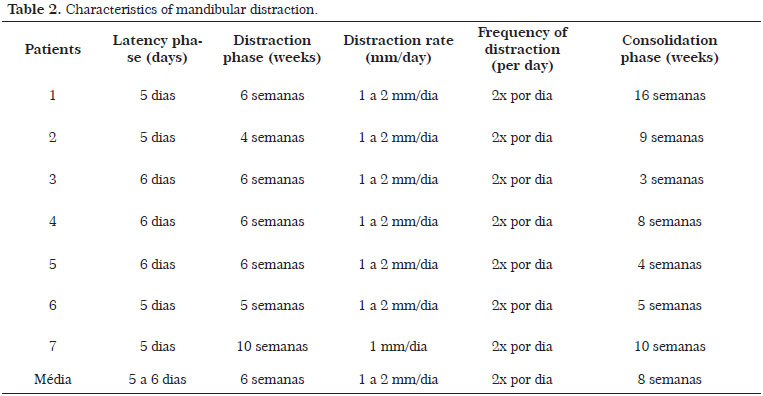
The latency phase, the interval between surgery and the beginning of the distraction, was between 5 and 6 days in all patients.
Distraction Phase
The distraction phase, during which the distractor is activated daily in a gradual manner, was performed by the patients themselves or by the tutors under the guidance of the multidisciplinary team. The distraction phase lasted from 4 to 10 weeks. The mean distraction time was 6 weeks. The distraction rate was 1-2 mm/day in all patients.
Consolidation Phase
In the consolidation phase, the time between the end of the distraction and the withdrawal of distractors, the distraction apparatus itself works as an anchoring system for which there is a consolidation of bone formed at the position reached. The consolidation phase lasted from 5 to 16 weeks. The average consolidation phase was 8 weeks (Table 2).
All patients with TMJ ankylosis presented difficulties in stomatognathic function (mastication, swallowing, and phonation) because of the limitation in oral opening. Concerning the airways, one patient with bilateral TMJ ankylosis (14%) was tracheostomized and four (66%) had considerable snoring during sleep. In the case of patients with craniofacial microsomia, the mouth opening was normal, there was no snoring, and mastication presented with a unilateral default contralateral to the affected side.
In the postoperative period, there was improvement in all stomatognathic function and weight gain in all patients, decannulation of the tracheostomized patient, and considerable improvement in the quality of sleep in patients who snored. The improvement of snoring was reported by patients and family members; we did not perform pre- and postoperative polysomnography.
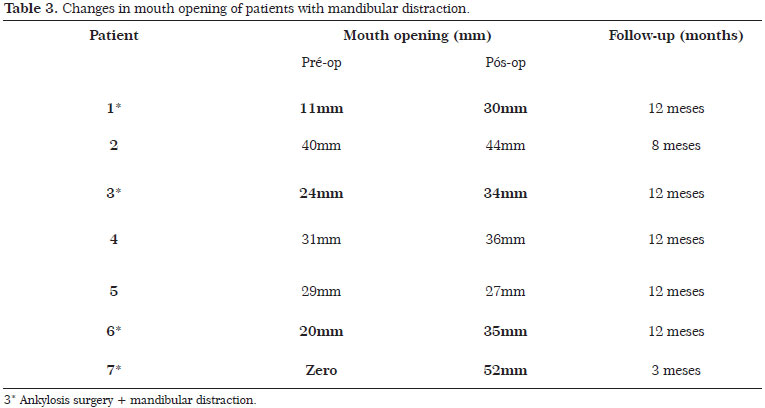
From the dental-skeletal and aesthetic point of view, all patients presented with a convex face profile (class II of angle and negative overjet) and with some degree of laterognathism and cross bite. Patients with craniofacial microsomia had Pruzansky IIB mandibular hypoplasia and normal mouth opening. All patients with unilateral or bilateral TMJ ankylosis had decreased mouth opening, ranging from 0 to 31 mm. The mean mouth opening of this group of patients was 19 mm; this measurement considered the inter-incisor distance, except for patient 7 whose teeth hardly had exposed crowns. That is, the negative overjet of these patients contributed to the calculation of the final preoperative opening.
There was improvement in all patients from the dental-skeletal and aesthetic point of view: facial profiles were improved and even hypercorrected, the laterognathism was eased, and the mouth opening increased in most (86%) of them (Figure 3). The mouth opening increased more significantly in those patients who received ankylosis surgery in conjunction with mandibular distraction (Table 3) (Figure 4). Three patients remained with cross bite, and three developed an anterior open bite.

Figure 3. Patient 3: bearer of right TMJ ankylosis submitted to ankylosis surgery + bilateral internal distraction. There was improvement of facial symmetry, elimination of snoring during sleep, and only a small scar where the activation pin exited.

Figure 4. Patient 7: carrier of bilateral temporomandibular joint (TMJ) ankylosis submitted to ankylosis surgery + bilateral external distraction. There was a considerable improvement in stomatognathic function and in the mouth opening, in addition to the aesthetic improvement. The mouth opening improved from 0 to 52mm.
Radiologically, the bone gain obtained in the mandibular ramus became apparent, together with mandibular advancement and increased retromandibular column of air in the airways of these patients. Clinically, the soft tissue followed this bone gain (Figure 5).

Figure 5. Patient 4: carrier of bilateral temporomandibular joint (TMJ) ankylosis submitted to external bilateral distraction. There was a considerable elongation of the jaw and soft parts, providing a complete change of aesthetic profile and decannulation of the tracheostomy. Profile cephalometry reveals a very clear increase of the retromandibular air column.
The most common complication was pain upon distraction, which was reported by five patients (71%), one of them was treated with opiates at one moment. Two of the four (50%) patients with external distractors reported social problems due to the appearance of the system, and one of them missed school throughout the treatment period and almost lost the entire academic year. Only one of three patients (33%) with internal distractors reported social problems. Two of the four patients (50%) with external distractors showed hypertrophic scars; one of them was indicated for surgical revision (Figure 6). Three patients (43%) progressed with neuropraxia of the inferior alveolar nerve; two progressed with loss of tonicity of the upper lip (29%); and two (29%) progressed with paresis of mandibular and/or buccal branches of the facial nerve. All these changes in sensitivity and motricity were transient and successfully treated by a speech therapist. In one patient (14%), the length of the distractor appeared to be inadequate; that is, we could have lengthened the jaw a little more if we had placed a larger distractor (Figure 7).

Figure 6. Patient 6: carrier of bilateral temporomandibular joint (TMJ) ankylosis submitted to ankylosis surgery + external bilateral distraction. Despite the result, hypertrophic scars remained on the face.

Figure 7. Patient 2: carrier of hemifacial microsomia submitted to bilateral internal distraction. The distraction was performed up to the limit of the appliance; however, perhaps a larger distractor would have improved the inclination of the oral commissure.
All of the patients and their tutors found that the treatment with mandibular distraction was satisfactory. All of them recognized the functional improvement and the considerable change in facial aesthetics after the procedure. We also noticed that the self-esteem of these patients clearly increased.
DISCUSSION
Although mandibular distraction was presented as a therapeutic alternative for mandibular hypoplasia in 1992 with the publication of McCarthy et al.1, and of Molina et al. in 19953, this surgery is not currently routinely performed in many major centers in Brazil. It is common to encounter patients with congenital deformities (e.g., craniofacial microsomia) in preadolescence and adolescence who have never received surgical treatment. These patients have lost time for distraction, may have already experienced problems in social adaptation, and are now faced with the decision to either undergo distraction or wait for complete development before undergoing an orthognathic surgery. Besides the lack of bone development, many of these patients present with associated considerable soft tissue hypoplasia, which can be a determining factor for the failure of a possible surgical bone movement (orthognathic surgery).
As a rule, an indication for distraction takes into account primarily the issue of impaired airways and facial dysmorphy. In the case of airway impairment, distraction must commence as early as possible, in order to avoid a tracheostomy or enable decannulation5. In cases of facial dysmorphy, distraction is recommended before the patient reaches school age6. McCarthy et al.1 stipulated some criteria for these indications in accordance with the age of the patient and the severity of the condition (Table 4).

Our still limited sample in the INTO impedes us from presenting a characteristic profile of our patients who underwent distraction (Tables 1 and 2). Ow et al.5, in a large meta-analysis with 1185 patients, selected in 2012, presented the profiles shown in (Tables 5-7).



With regard to the type of distractor used on the patients, there are some aspects that should be taken into account. The external distractor is preferable in the case of very hypoplastic mandibles, previously grafted jaws, and mandibles with little bone for fixation of internal distractor plates. This has the advantage of allowing distraction in multiple vectors, which is desirable for the correction of an anterior open bite and to guide a neocondyle to the glenoid fossa16. The disadvantages are the scar formation, higher social impact of an external equipment, and greater vulnerability to accidents, especially distractor movement in small traumas involving children5.
The internal distractor, on the other hand, has the great advantage of causing lesser scars. Mechanically, it also seems to be more advantageous because the appliance is fixed to the bone, unlike the external distractor that is 30-40 mm away. The distraction in these cases is only performed in one vector and is particularly suitable for vertical vectors (from 45° to 90º from the maxillary occlusal plane). Fortunately, this distraction vector is very frequent and is the best option for the elongation of the mandibular ramus, the most affected segment in mandibular hypoplasia. The disadvantages are the requirement for a jaw with at least 12 mm width and the need for a second surgery for the removal of the distractor6. Despite the different characteristics of each distractor, as ours is a public hospital, often the major criterion for the selection of the distractor is availability.
Most of the patients operated at the INTO had TMJ ankylosis. In this metric, the mandibular distraction exerts an interesting effect on the TMJ and can be used in the treatment of ankylosis of this joint. McCormick et al.14,15 showed that compressive forces of distraction benefit the structure and position of the TMJ, with the condyles exhibiting an increased size, improvement in geometry, and increase in vertical height after the mandibular distraction. In the case of an established TMJ ankylosis, the resection of the ankylotic block can be associated with mandibular distraction in the same surgical moment. This technique is called transport distraction16 and is a sum of transport techniques with bone distraction. An L or a vertical osteotomy is made in the ramus by creating a bone disk that will be transported by distraction. During the activation phase, this neocondyle, pressed to the glenoid fossa, will be refurbished, creating a rounded and smooth articular surface. The distraction continues until the ramus reaches a suitable height and the neocondyle moves into the glenoid fossa. In these cases, the consolidation phase is kept; however, active motion exercises of the TMJ should be started 1 week after the end of the activation phase.
The decision of when to stop the distraction can be confusing and is usually clinical17. We observed hypo- and hypercorrection in the antero-posterior plane of the mandible, as well as extreme difficulty in positioning the equipment in the midline in patients with laterognathism. In cases of antero-posterior deficiency in still developing patients, hypercorrection is preferable. Yet, even after reaching the desired hypercorrection, possibly almost all of these patients will have an indication for a new distraction or orthognathic surgery when they attain maturity of skeletal development18.
The improvement of the dental-skeletal characteristics was evident in patients operated at the INTO. However, although the gain in function and facial aesthetics was considerable, the orthodontic issue was not covered due to the lack of this specialty in our multidisciplinary team. Ideally, a pre- and postoperative follow-up of these patients should be done, similar to what is advocated in orthognathic surgery 19. Currently, all of our patients are receiving orthodontic treatment owing to a partnership with another hospital.
The most common complication was pain upon activation. This may be related to the distraction rate used (2 mm/day). The typical complications of external distractors were valued by our patients. The social problems and the scars, fortunately, were compensated with a general improvement, also highly valued by them. The support of speech therapy was very important for the treatment of all complications, especially nerve paresis, paresthesias, and transitory muscle hypotonia. We compared our observed complications with those reported by another service18 in Table 8.

Finally, we believe that the presence of a qualified multidisciplinary team has a large contribution in the treatment of these patients. A good result largely depends on the commitment of the patient in this long-term follow-up, in which the surgery is only one of several steps involved.
CONCLUSION
We believe that mandibular distraction osteogenesis is a good alternative for the treatment of mandibular hypoplasia, often being the first indication in some clinical situations. This procedure apparently has less morbidity than the classic reconstructions of the jaw and has the added benefit of also lengthening the soft tissues. In addition, there is a likely benefit to the airways. A qualified and complete multidisciplinary team greatly increases the chances of success in this type of treatment.
REFERENCES
1. McCarthy JG, Stelnicki EJ, Mehrara BJ, Longaker MT. Distraction osteogenesis of the craniofacial skeleton. Plast Reconstr Surg. 2001;107(7):1812-27.
2. Pereira MA, Luiz Freitas PH, Rosa TF, Xavier CB. Understanding distraction osteogenesis on the maxillofacial complex: a literature review. J. Oral Maxillofac Surg. 2007;18(1):29-38.
3. Molina F, Monasterio FO. Mandibular elongation and remodeling by distraction: the farewell to major osteotomies. Plast Reconstr Surg. 1995;96(4):825-40.
4. McCarthy JG, Katzen JT, Hooper R, Grayson BH. The first decade of mandibular distraction: lessons we have learned. Plast Reconstr Surg. 2002;110:1704-13.
5. Ow TA, Cheung LK. Meta-analysis of mandibular distraction osteogenesis: clinical applications and functional outcomes. Plast Reconstr Surg. 2008;121(3):54e-69e.
6. Davidson EH, Brown D, Shetye PR, Greig AV, Grayson BH, Warren SM, et al. The evolution of mandibular distraction: device selection. Plast Reconstr Surg. 2010;126(6):2061-70.
7. Williams JK, Rowe NM, MacKool RJ, Levine JP, Hollier LH, Longaker MT, et al. Controlled multiplanar distraction of the mandible. Part II: laboratory studies of page (anteroposterior) and vertical (superoinferior) movements. J Craniofac Surg. 1998;9:504-13.
8. Diner PA, Kollar EM, Martinez H, Vazquez MP. Intraoral distraction is mandibular lengthening: the technical innovation. J Craniomaxillofac Surg. 1996;24:92-5.
9. Diner PA, Kollar, Martinez H, Vazquez MP. Sub-merged intraoral device for mandibular lengthening. J Craniomaxillofac Surg. 1997;25:116-23.
10. Klein C, Howaldt HP. Correction of mandibular hypoplasia by means of bidirectional callus distraction. J Craniofac Surg. 1996;7:258.
11. Roth DA, Gosain AK, McCarthy JG, Stracher MA, Lefton DR, Grayson BH. A CT scan technique for quantitative volumetric assessment of the mandible after distraction osteogenesis. Plast Reconstr Surg. 1997;99:1237-47.
12. Pensler JM, Goldberg DP, Lindell B, Carroll NC. Skeletal distraction of the hypoplastic mandible. Ann Plast Surg. 1995;34:130-6.
13. Marcus JR, Erdmann D, Rodriguez ED. Essentials of craniomaxillofacial trauma. St. Louis, Missouri: Quality Medical Publishing; 2012.
14. McCormick SU, McCarthy JG, Grayson BH, Staffenberg D, McCormick SA. Effect of mandibular distraction on the temporomandibular joint. Part 1: canine study. J Craniofac Surg. 1995;6:358-63.
15. McCormick SU, Grayson BH, McCarthy JG, Staffenberg D. Effect of mandibular distraction on the temporomandibular joint. Part 2: clinical study. J Craniofac Surg. 1995;6:364-7.
16. McCormick S. Distraction osteogenesis. Dent Today 1996;15:58.
17. Freitas RS, Busato L, D'Oro U, Ferreira MC. Mandible distraction using internal device: mathematical intelligence analysis of the result. J Craniofac Surg. 2007;18:29-38.
18. Shetye PR, Warren SM, Brown D, Garfinkle JS, Grayson BH, McCarthy JG. Documentation of incidents associated with mandibular distraction: introduction of the new stratifications system. Plast Reconstr Surg. 2009;123(2):627-34.
19. Da Silva Freitas R, Tolazzi AR, Alonso N, Cross GA, Busato L. Evaluation of molar teeth and buds in patients submitted to mandible distraction: long-term results. Plast Reconstr Surg. 2008;121(4):1335-42.
1. Effective Member of the SBCP - Effective Member of ABCCMF
2. Full Member of the SBCP - Head of the Center for Specialized Care in Craniomaxillofacial Surgery of the INTO-RJ
3. Professor in Plastic Surgery at the FMUSP - Head of the Department of Craniomaxillofacial Surgery, Division of Plastic Surgery and Burns of the HC-FMUSP
4. Professor at the University of Sao Paulo - Head of the Plastic Surgery department and Service at the UFPR
5. Full Member of the SBCP - Effective Member of ABCCMF
6. Full Member of the SBCP - Plastic and Craniomaxillofacial Surgeon of the INTO-RJ
7. Full Member of the SBCP - Effective Member of ABCCMF
8. Effective Member of the SBCP - Effective Member of ABCCMF
9. Effective Member of the SBCP - Ex-trainee in Craniomaxillofacial Surgery of the INTO-RJ
Institution: National Institute of Traumatology and Orthopaedics (INTO-RJ).
Corresponding Author:
Pablo Maricevich
Av. Antônio de Góes 275, sala 407, Pina
Recife - PE, Brazil. CEP: 51110-000
Article submitted: January 15, 2014.
Article accepted: December 13, 2014.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket