



Reviw Article - Year 2014 - Volume 29 -
Nerve alterations in rhytidoplasty: a systematic literature review
Alterações nervosas na ritidoplastia: uma revisão sistemática
ABSTRACT
INTRODUCTION: Rhytidoplasty has become one of the most common aesthetic surgeries performed by plastic surgeons worldwide. Along with the increase in the number of surgeries performed, the number of procedure-related complications has also increased. In particular, nerve injuries are the major concern. By conducting a systematic review, the present study aimed to identify the main nerve structures injured during rhytidoplasty, by either the conventional or endoscopic technique.
METHODS: A systematic literature review was performed in the main databases currently used. Articles that met the inclusion criteria were analyzed in their entirety, and their references were checked. Finally, 20 studies were included.
RESULTS: In these 20 articles, 3,347 patients were evaluated and 142 nerve injuries found, of which 79 were of the facial nerve, 55 were of the trigeminal nerve, and eight were of the great auricular nerve. Of these, only two were definitive. The lesions were more prevalent (81%) with the video-assisted techniques than with the conventional techniques (19%).
CONCLUSION: We found that the injuries of the temporal and buccal branches were more frequent during facelifts; and those of the great auricular nerve, during cervical rhytidoplasty. Although nerve injuries are infrequent in the literature, well-designed studies that aim to better understand these complications are lacking.
Keywords: Rhytidoplasty; Facial nerve; Trigeminal nerve; Cervical plexus.
RESUMO
INTRODUÇÃO: A ritidoplastia se tornou uma das cirurgias estéticas mais realizadas por cirurgiões plásticos ao redor do mundo. Junto com o aumento do número de cirurgias, a quantidade de complicações associadas ao procedimento também aumentou, sendo que as alterações nervosas são uma das que despertam maiores preocupações. O presente estudo visa a identificar, por meio de uma revisão sistemática, as principais estruturas nervosas lesadas durante uma ritidoplastia, tanto por técnicas convencionais como endoscópicas.
MÉTODOS: Uma revisão sistemática da literatura foi realizada nas principais bases de dados utilizadas atualmente. Artigos que preencheram os critérios de inclusão foram analisados na íntegra e suas referências, verificadas. Ao final, 20 estudos foram incluídos.
RESULTADOS: Nestes 20 artigos, no total, foram avaliados 3.347 pacientes, sendo encontradas 142 lesões nervosas: 79 do nervo facial; 55 do nervo trigêmeo, e oito do nervo auricular magno. Destas, apenas duas foram definitivas. As lesões, proporcionalmente, foram mais comuns nas técnicas videoassistidas (81%), quando comparadas com as convencionais (19%).
CONCLUSÃO: Encontramos que as lesões dos ramos temporal e bucal são mais frequentes no facelift e as do nervo auricular magno, na ritidoplastia cervical. Apesar de as lesões nervosas serem pouco frequentes na literatura, faltam estudos bem desenhados que busquem conhecer melhor estas complicações.
Palavras-chave: Ritidoplastia; Nervo facial; Nervo trigêmeo; Plexo cervical.
Rhytidoplasty is currently one of the most common aesthetic surgeries performed by plastic surgeons worldwide. Many techniques for facial rejuvenation have been described in the literature, the oldest of which was reported in 1919 by Passot1, who described in detail a browlift. Since then, facial rejuvenation has gone through a constant evolution of surgical techniques, beginning with the simple classic procedures to composite techniques, involving various procedures. Currently, the number of minimally invasive and endoscopic surgeries has increased since the 1990s2,3. Along with this increase, the number of procedure-related complications has grown, with nerve injuries being the major concern.
The present study aimed to identify by conducting a systematic review of the literature the main nerve structures injured during a rhytidoplasty, by either the conventional or endoscopic technique, regardless of the approach used, in order to direct plastic surgeons toward reducing the risk of complications from facial or cervical nerve injuries.
METHODS
The study began with a search of the topic in the following main electronic databases currently used: PUBMED, SCOPUS, and EMBASE. The following keywords were used in the following order:
1) FaceliftThe initial research strategy was to search articles pertaining to the relationship of the abovementioned words, in the abovementioned main databases. The titles and abstracts were read, and all the articles that were included in the study were analyzed in their entirety. The references were also rigorously researched in order to include articles of interest. All of the articles were accessed by two independent researchers (MAS and EP) by using the following inclusion criteria: texts in English and Portuguese, published over the past 15 years, patients of both sexes and older than 18 years, and no age limit. Duplicate articles were removed. Studies that used animals, corpses, or adolescents were excluded. All of the survey data were tabulated in a spreadsheet for statistical analysis of the data. The organogram that exemplifies the search is described in Figure 1.
2) Paresthesia or paresis
3) ( # 1) and ( # 2)

Figure 1. In total, 113 studies were initially found, but only 18 met the inclusion criteria. After the analysis of the references of these articles, two more were added, for a total of 20 studies.
RESULTS
The search revealed 20 articles. The following items were analyzed: country of origin; the number, sex, and age of the patients; the surgical technique used; the nerve injury found; and the time of postoperative control (Table 1). The country that produced the most number of articles of interest was the United States with nine, followed by Brazil and France with two articles each. South Korea, Lithuania, Argentina, United Kingdom, Singapore, Spain, and Turkey contributed one article each. The total number of patients involved was 3,347. The study of Tanna and Lindsey (2008)4 from the University of Washington had the largest number of individuals assessed (1000 patients). The articles by Malata and Abood (2009)5 and Newman (2006)6 from the United Kingdom and United States assessed the smallest number of patients (30 and 10 patients, respectively).
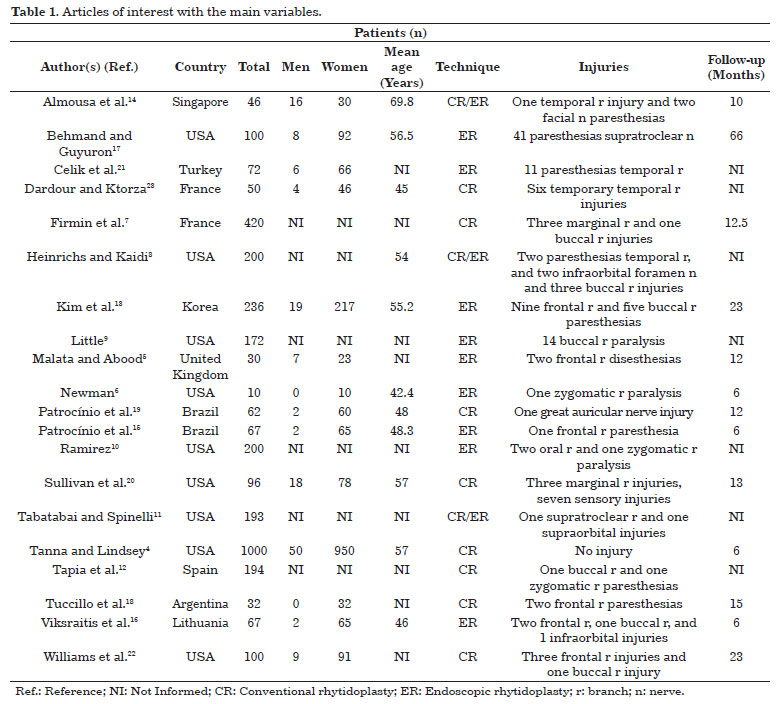
Some articles did not detail sex7-12. In those that reported sex, 143 were men and 1,825 were women; therefore, only 7.2% patients were male. In our comparative analysis of mean age, we found that this ranged from 42.4 years for women to 69.8 years for men, the youngest and oldest being 29 years13 and 84 years, respectively14. The mean patient follow-up period also varied greatly according to study type. The smallest and most common study type had 6 months' follow-up4,6,15,16, and the largest had 5.5 years17. Regardless of the specific surgical technique used, the rhytidoplasties were allocated into two groups as follows: those that used conventional or classic techniques, and those that were endoscopy or video assisted. In seven articles, the conventional technique was used, while 10 articles reported video-assisted techniques. In three articles8,11,14, both techniques were used.
When we analyzed the anatomical regions addressed during facelifts, we observed that most authors opted toward the temporal fascia 4-6,12,14,18 or in combination with dissection of the frontal fascia13,19. The superficial musculoaponeurotic system (SMS) was only approached in six studies7,8,11,15,20,21.
Regarding the nerve injuries involved in rhytidoplasty, the number of sensory injuries observed, which were mostly of the facial nerve compared with the trigeminal nerve, was much larger than that of motor injuries. In total, of 79 facial nerve injuries, 18 were caused by conventional rhytidoplasty and 61 were caused by the endoscopic rhytidoplasty (Figure 2). Of 55 trigeminal nerve injuries, 1 was caused by conventional rhytidoplasty and 54 were caused by endoscopic rhytidoplasty. Eight great auricular nerve injuries were incurred during cervical rhytidoplasty (Table 2). All of the injuries found were transitory, with the exception of those in the study by Sullivan et al. (1999)20, who identified a permanent injury on the frontal branch of the facial nerve, which was caused during the training of residents in otolaryngology, and those in the study by Williams et al (2003)22, who found a permanent change in the maxillary branch of the trigeminal nerve.

Figure 2. Of the 142 nerve injuries identified, 79 were of the facial nerve branches, of which 77% were caused by video-assisted techniques.

Regarding the type of technique used, conventional rhytidoplasty was performed in 2,046 patients, whereas endoscopic rhytidoplasty was performed in 1,301 patients (61% versus 39%). When we separated the nerve injuries according to either conventional or endoscopic rhytidoplasty, we observed that the video-assisted technique presented a much higher prevalence of injuries than the classical techniques (81% versus 19%).
DISCUSSION
Rhytidoplasty is becoming increasingly common. The number of techniques published and their results vary greatly. The ability to restore the harmony of facial features requires rigor in applying the techniques, exquisite knowledge of the anatomy, and artistic sensibility to individualize the surgical objective for each patient11. Failure to observe these basic laws can lead to extremely undesirable changes, some permanent.
The complications of rhytidoplasty are well known, including hematoma, alopecia, hypertrophic scar, infection, facial contour deformity, and sensory and motor lesions. Hematoma is still the most common complication; however, if controlled early, it has little effect on the final surgical result24.
Great auricular nerve injury is the most common nerve injury related to cervical rhytidoplasty16. In a residency program, Sullivan et al.20, during the assessment of sensory injuries in rhytidoplasty, found six cases of temporary paresthesia in the ear and one case that evolved permanent sensory loss of the auricular region due to great auricular nerve injury.
Transient paresthesia and hyperesthesia of the lower two-thirds of the middle ear, the preauricular region, and neck usually last from 2 to 6 weeks and are the result of inevitable injury to a small amount of nervous tissue in the surgical area of rhytidoplasty. The permanent sensory injury in the lower portion of the ear, in turn, is generally due to deep dissection of the middle portion of the sternocleidomastoideus muscle25.
The mechanism of sensory injury more commonly involved anesthesia infiltration, nerve perforation by the anesthesia needle, and deep and extensive dissection, in addition to swelling or injury of the nerve during electrocautery. In the articles included in this review, no reference was made on the use of the latter methodology. However, in the study of Firmin et al.7, a device similar to a cautery, the harmonic blade, was used. In this study, only four cases of temporary paralysis of the facial nerve were observed, all of which were completely resolved in 3 postoperative months.
In general, paresthesia caused by anesthesia infiltration spontaneously resolve in a few hours, when the anesthetic effect ceases. However, the temporary injury can last from 24 hours up to weeks and is usually caused by direct injury to the nerve20. In our review, we observed a large variation in the recovery of temporary nerve lesions. The minimum recovery period was 41 days for an injury to the temporal branch of the facial nerve in the study by Heinrichs and Kaidi in 19988. The maximum recovery period was 2 years in a patient with an injury of the supratroclear branch of the ophthalmic nerve incurred during a facelift, in the study by Behmand and Guyuron in 200617. However, we observed that in most of the articles analyzed, the most common recovery interval was between 6 weeks and 6 months5-7,9,13,14,19.
Permanent facial nerve injury is a rare complication, whereas temporary injuries are much more common. In a review of the literature conducted by Rubin and Simpson26 in 1996, in 7,000 cases of superficial rhytidoplasty, only 55 cases were motor injuries, the most common being of the temporal branch, followed by the marginal mandibular nerve. Of the 55 cases, only seven were definitive. In our review of 3,347 patients, 139 had some degree of temporary injury, only two of which were permanent. One of the permanent injuries was of the maxillary branch of the trigeminal nerve incurred during a browlift22. The patient progressed with permanent loss of sensitivity of the region supplied by this nerve. The second case was of the great auricular nerve, incurred during a cervical rhytidoplasty in a residency program, as described before20.
Although the prevalence of injuries varies greatly depending on the study, all studies agree that the frontal and marginal mandibular branches of the facial nerve have the highest risk of injury and permanent dysfunction during a facelift25. The mechanisms of injury to the marginal branch include transection during deep dissection of the subplatysmal flap, plication sutures, tissue traction, and cervical liposuction in the subplatysmal plane. Ellenbogen28 described two cases of transient pseudoparalysis of the marginal mandibular branch due to an injury in the cervical branch. These injuries can be distinguished from injuries of the marginal mandibular branch because these patients can still evert the lower lip because of preservation of the function of the mentalis muscle. The vulnerable point to injury of the marginal mandibular nerve is after leaving the deep cervical fascia, when it runs on the anterior face of the jaw, in the region of the facial artery27.
Regardless of the article analyzed, in all of the studies, we opted for a conservative assessment of nerve injuries. In none of these studies was any directed clinical treatment proposed.
In our systematic review, we observed that the video-assisted techniques presented a higher prevalence of nerve injuries than the classical techniques (81% versus 19%). Although only few studies have addressed this topic in the literature, it is true that in the United States, the endoscopic technique has been progressively abandoned because of the high cost of the equipment, the long learning curve, or the long operative time required for this procedure. In fact, in that country, more attention has been given to approaches that require reduced access but by using the conventional techniques29.
CONCLUSION
The actual incidence of nerve injuries in rhytidoplasty has not yet been determined. Prospective studies are required that more accurately objectively and critically assess the sensitivity, and facial and cervical movements of patients. This systematic review reaffirms the statements of other authors on the main facial changes and still managed to observe that these lesions are more prevalent when endoscopic procedures are performed.
REFERENCES
1. Passot R. La chirurgie esthétique des rides du visage. Presse Med. 1919;27:258-60.
2. Isse NG. Endoscopic forehead lift. Evolution and update. Clin Plast Surg. 1995;22(4):661-73. PMid:8846634.
3. Ozerdem OR, Vasconez LO, de la Torre J. Upper face-lifting. Facial Plast Surg Clin North Am. 2006;14(3):159-65. http://dx.doi.org/10.1016/j.fsc.2006.04.001. PMid:16908382
4. Tanna N, Lindsey WH. Review of 1,000 consecutive short-scar rhytidectomies. Dermatol Surg. 2008;34(2):196-202, discussion 202-3. http://dx.doi.org/10.1097/00042728-200802000-00008. PMid:18093201
5. Malata CM, Abood A. Experience with cortical tunnel fixation in endoscopic brow lift: the "bevel and slide" modification. Int J Surg. 2009;7(6):510-5. http://dx.doi.org/10.1016/j.ijsu.2009.08.013. PMid:19800433
6. Newman J. Safety and efficacy of midface-lifts with an absorbable soft tissue suspension device. Arch Facial Plast Surg. 2006;8(4):245-51. http://dx.doi.org/10.1001/archfaci.8.4.245. PMid:16847170
7. Firmin FO, Marchac AC, Lotz NC. Use of the harmonic blade in face lifting: a report based on 420 operations. Plast Reconstr Surg. 2009;124(1):245-55. http://dx.doi.org/10.1097/PRS.0b013e3181ab130f. PMid:19568088
8. Heinrichs HL, Kaidi AA. Subperiosteal face lift: a 200-case, 4-year review. Plast Reconstr Surg. 1998;102(3):843-55. http://dx.doi.org/10.1097/00006534-199809010-00036. PMid:9727455
9. Little JW. Three-dimensional rejuvenation of the midface: volumetric resculpture by malar imbrication. Plast Reconstr Surg. 2000;105(1):267-85, discussion 286-9. http://dx.doi.org/10.1097/00006534-200001000-00044. PMid:10626999
10. Ramirez OM. Three-dimensional endoscopic midface enhancement: a personal quest for the ideal cheek rejuvenation. Plast Reconstr Surg. 2002;109(1):329-40, discussion 341-9. http://dx.doi.org/10.1097/00006534-200201000-00052. PMid:11786834
11. Tabatabai N, Spinelli HM. Limited incision nonendoscopic brow lift. Plast Reconstr Surg. 2007;119(5):1563-70. http://dx.doi.org/10.1097/01.prs.0000256073.49355.fc. PMid:17415251
12. Tapia A, Ruiz-de-Erenchun R, Rengifo M. Combined approach for facial contour restoration: treatment of malar and cheek areas during rhytidectomy. Plast Reconstr Surg. 2006;118(2):491-7, discussion 498-501. http://dx.doi.org/10.1097/01.prs.0000235265.26138.66. PMid:16874222
13. Kim IG, Oh JK, Baek DH. Personal experiences and algorithm of endoscopically assisted subperiosteal face lift in Orientals for 5 years. Plast Reconstr Surg. 2001;108(6):1768-79, discussion 1780-1. http://dx.doi.org/10.1097/00006534-200111000-00053. PMid:11711962
14. Almousa R, Amrith S, Sundar G. Browlift-a South East Asian experience. Orbit. 2009;28(6):347-53. http://dx.doi.org/10.3109/01676830903104652. PMid:19929658
15. Patrocínio LG, Reinhart RJY, Patrocínio TG, Patrocínio JA. Frontoplastia endoscópica: três anos de experiência. Rev Bras Otorrinol. 2006;72(5):624-30. http://dx.doi.org/10.1590/S0034-72992006000500008.
16. Viksraitis S, Astrauskas T, Karbonskiene A, Budnikas G. Endoscopic aesthetic facial surgery: technique and results. Medicina (Kaunas). 2004;40(2):149-55. PMid:15007274.
17. Behmand RA, Guyuron B. Endoscopic forehead rejuvenation: II. Long-term results. Plast Reconstr Surg. 2006;117(4):1137-43, discussion 1144. http://dx.doi.org/10.1097/01.prs.0000215331.89085.a6. PMid:16582776
18. Tuccillo F, Jacovella P, Zimman O, Repetti G. An alternative approach to brow lift fixation: temporoparietalis fascia, galeal, and periosteal imbrication. Plast Reconstr Surg. 2007;119(2):692- 702. http://dx.doi.org/10.1097/01.prs.0000246526.59290.57. PMid:17230109
19. Patrocínio JA, Patrocínio LG, Aguiar ASF. Complicações de ritidoplastia em um service de residência médica em otorrinolaringologia. Rev Bras Otorrinolaringol (Engl Ed). 2002;68(3):338-42. http://dx.doi.org/10.1590/S0034-72992002000300008.
20. Sullivan CA, Masin J, Maniglia AJ, Stepnick DW. Complications of rhytidectomy in an otolaryngology training program. Laryngoscope. 1999;109(2 Pt 1):198-203. http://dx.doi.org/10.1097/00005537-199902000-00005. PMid:10890765
21. Celik M, Tuncer S, Buyukcayir I. Modifications in endoscopic facelifts. Ann Plast Surg. 1999;42(6):638-43. http://dx.doi.org/10.1097/00000637-199906000-00010. PMid:10382801
22. Williams EF III, Vargas H, Dahiya R, Hove CR, Rodgers BJ, Lam SM. Midfacial rejuvenation via a minimal-incision brow-lift approach: critical evaluation of a 5-year experience. Arch Facial Plast Surg. 2003;5(6):470-8. http://dx.doi.org/10.1001/archfaci.5.6.470. PMid:14623683
23. Dardour JC, Ktorza T. Endoscopic deep periorbital lifting: study and results based on 50 consecutive cases. Aesthetic Plast Surg. 2000;24(4):292-8. http://dx.doi.org/10.1007/s002660010049. PMid:10954794
24. Daane SP, Owsley JQ. Incidence of cervical branch injury with "marginal mandibular nerve pseudo-paralysis" in patients undergoing face lift. Plast Reconstr Surg. 2003;111(7):2414-8. http://dx.doi.org/10.1097/01.PRS.0000061004.74788.33. PMid:12794490
25. McCollough EG, Perkins SW, Langsdon PR. SASMAS suspension rhytidectomy: rationale and long-term experience. Rationale and long-term experience. Arch Otolaryngol Head Neck Surg. 1989;115(2):228-34. http://dx.doi.org/10.1001/archotol.1989.01860260102023. PMid:2643976
26. Rubin LR, Simpson RL. The new deep plane face lift dissections versus the old superficial techniques: a comparison of neurologic complications. Plast Reconstr Surg. 1996;97(7):1461-5. http://dx.doi.org/10.1097/00006534-199606000-00024. PMid:8643732
27. Biggs TM. Endoscopic brow lift: a retrospective review of 628 consecutive cases over 5 years. Plast Reconstr Surg. 2004;113(7):2219, author reply 2219-20. http://dx.doi.org/10.1097/01.PRS.0000123600.67295.57. PMid:15253222
28. Ellenbogen R. Pseudo-paralysis of the mandibular branch of the facial nerve after platysmal face-lift operation. Plast Reconstr Surg. 1979;63(3):364-8. http://dx.doi.org/10.1097/00006534-197903000-00012. PMid:419214
29. Chiu ES, Baker DC. Endoscopic brow lift: a retrospective review of 628 consecutive cases over 5 years. Plast Reconstr Surg. 2003;112(2):628-33, discussion 634-5. http://dx.doi.org/10.1097/01.PRS.0000071042.11435.2E. PMid:12900626
1. MD, Resident in General Surgery at the Hospital de Clínicas, Universidade Estadual de Campinas (UNICAMP), Campinas, SP, Brazil
2. Undergraduate Student in Medicine, Faculdade de Ciências Médicas, Universidade Estadual de Campinas (UNICAMP), Campinas, SP, Brazil
3. MSc, Assistant Professor of Plastic Surgery, Department of Surgery, Faculdade de Ciências Médicas da Universidade Estadual de Campinas (UNICAMP), Campinas, SP, Brazil
4. Professor of Maxillo-Facial Surgery, Section of Plastic Surgery, Department of Surgery, Faculdade de Ciências Médicas da Universidade Estadual de Campinas (UNICAMP), Campinas, SP, Brazil
Institution: Work conducted at the Faculty of Medical Sciences of the Universidade Estadual de Campinas (UNICAMP), Campinas, SP, Brazil.
Corresponding author:
Luis Augusto Passeri
Faculty of Medical Sciences - Unicamp
Rua Tessália Vieira de Camargo, 126 Cidade Universitária "Zeferino Vaz,"
Campinas, SP, Brazil CEP 13983-887
E-mail: passeri@fcm.unicamp.br
Article received: November 11, 2012.
Article accepted: March 3, 2013.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket