



Original Article - Year 2014 - Volume 29 -
Quality of life in patients undergoing transverse rectus abdominis myocutaneous flap breast reconstruction
Qualidade de vida em pacientes submetidas à reconstrução de mama com retalho miocutâneo transverso do reto abdominal
ABSTRACT
INTRODUCTION: Breast reconstruction is intended to improve the quality of life of patients who underwent mastectomy, and the use of the Transverse Rectus Abdominis Myocutaneous (TRAM) flap is a valuable option.
OBJECTIVE: To assess the influence of delayed TRAM flap breast reconstruction on patient's quality of life.
METHODS: 30 breast cancer patients who had undergone mastectomy were enrolled in this cross-sectional study. Fifty of them (Study Group - SG) had undergone delayed TRAM flap breast reconstruction six months before, and the other 15 (Control Group) were scheduled for the operation. To assess quality of life, the Brazilian version of the Medical Outcomes Study 36-item Short-form Health Survey (SF-36) was used. Data were statistically compared.
RESULTS: Compared to CG, patients in SG had better quality of life scores for the SF-36 domains social aspect (p<0.001), mental health (p=0.002) and general health (p=0.008). No statistical significances were reached for the other SF-36 domains.
CONCLUSION: The delayed TRAM flap breast reconstruction had a positive influence on patient's quality of life.
Keywords: Quality of Life; Surgical Flap; Mastectomy.
RESUMO
INTRODUÇÃO: A reconstrução de mama visa melhorar a qualidade de vida das pacientes que se submeteram à mastectomia, e o uso do retalho miocutâneo transverso do abdome (TRAM) é uma opção valiosa.
OBJETIVO: Avaliar a influência da reconstrução mamária tardia com o retalho TRAM na qualidade de vida das pacientes.
MÉTODO: 30 pacientes com câncer de mama, mastectomizadas foram incluídas neste estudo transversal. 15 delas (Grupo Estudo - GE) foram submetidas à reconstrução mamária com retalho TRAM seis meses antes, e as outras 15 (Grupo Controle - GC) foram programadas para a operação. Para avaliar a qualidade de vida, foi utilizado a versão brasileira do Medical Outcomes Study 36-item Short-form Health SurveyQuestionnaire (SF-36). Os dados foram comparados estatisticamente.
RESULTADOS: Em comparação com o GC, as pacientes do GE apresentaram melhores escores do SF-36 nos domínios: aspecto social (p<0.001), saúde mental (p=0.002) e estado geral de saúde (p=0.008). Nenhuma significância estatística foi alcançada para os outros domínios do SF-36.
CONCLUSÃO: A reconstrução mamária tardia com retalho TRAM tem influência positiva na qualidade de vida das pacientes.
Palavras-chave: Qualidade de Vida; Retalhos Cirúrgicos; Mastectomia.
Breast reconstruction is an important aspect of plastic surgery. Increased disease-free survival has meant that quality of life and respect for bodily integrity are increasingly considered in breast cancer treatment1.
Breast reconstruction was previously considered detrimental to cancer treatment. However, evidence that reconstruction does not increase recurrence risks or retard diagnosis of local recurrence has resulted in its extensive use worldwide 2.
Transverse rectus abdominis myocutaneous (TRAM) flap surgery, a reconstruction option first described by Hartrampf et al. 3 and Gandolfo 4 in 1982, has gained immense popularity, and it has been used worldwide for numerous reconstructions, especially post-mastectomy breast reconstructions. The advantages of TRAM flap include the ability to use large amounts of autologous tissue without prostheses; a natural appearance and consistency similar to breast tissue, with improved symmetry; good results in overweight women and moderate to large breasts and bilateral reconstruction; possibility of repairing thoracic wall defects caused by mastectomy such as scars and other deformities; and the ability to replace irradiated skin during delayed reconstruction 5.
The literature generally describes breast reconstruction as a procedure that improves patient quality of life. The procedure may alleviate the emotional and physical effects of radical surgery. The immediate purpose of breast reconstruction is to repair a mutilation and restore the shape and volume of the amputated breast, thus preserving patient self-image and contributing to faster psychosocial recovery 6. The objective of this study was to evaluate the quality of life of patients who underwent TRAM flap breast reconstruction.
METHODS
This study was conducted at the Department of Plastic Surgery in the Women's Health Reference Center at Pérola Byington Hospital between May 2009 and March 2010. This clinical, primary, non-randomized, cross-sectional study was approved by the Institutional Research Ethics Committee, and all patients provided written informed consent.
In all, 30 patients with breast cancer treated at Unified Health System (SUS) who had undergone unilateral modified radical mastectomy were included in the study. Fifteen patients in the study group (SG) had undergone delayed TRAM flap mammary reconstruction 6 months previously; the remaining 15 patients in the control group (CG) were scheduled for the same procedure. Inclusion and allocation of patients to these groups were determined using eligibility criteria, including the following: patients who had previously undergone modified unilateral radical mastectomy and radiotherapy, who were between 30 and 65 years of age, and who had undergone late TRAM flap breast reconstruction surgery (SG) or were scheduled for this procedure (CG). Patients who underwent immediate breast reconstruction, breast reconstruction with another technique, or who had undergone reconstruction less than or more than 6 months previously were excluded from the SG. Obese patients (body mass index [BMI]> 30 kg/m2), smokers, patients with acute or chronic uncontrolled diseases or autoimmune diseases, those who had previously undergone abdominoplasty, or those who had other abdominal scars that could preclude TRAM were excluded from the CG.
Prior to inclusion in the study, all patients (SG and CG) were evaluated by the mastology team, and patients diagnosed with or under evaluation for local recurrence or metastatic disease were excluded.
To assess the quality of life, we used the Brazilian version of the Medical Outcomes Study: 36-Item Short-Form Health Survey (SF-36). 7 This generic instrument for assessing quality of life is widely used globally. It consists of 11 questions divided into 36 items covering many areas of quality of life: functional status, physical role, bodily pain, general health, vitality, social functioning, emotional role, and mental health. A score is assigned for each question, and total score values are transformed on a scale of 0 to 100, where zero corresponds to the worst health status and 100 the best. Each domain is analyzed separately 8.
Questionnaires were conducted by interviews performed by the same researcher in a secluded and peaceful environment.
Data were tabulated and analyzed statistically.
Statistical analysis
Given the nature of the variables, non-parametric tests were used. The Mann-Whitney9 U test was used to compare age and SF-36 scores between groups (SG and CG). The null hypothesis was rejected at 5%, corresponding to statistical significance for p values < 0.05.
RESULTS
The age of CG and SG patients ranged from 37 to 61 years (median: 48.0; mean ± SD: 48.3 ± 9.0) and from 35 to 62 years (median: 43.0; average ± SD: 43.5 ± 6.6), respectively.
Comparisons of SF-36 scores between groups are shown in Table 1 and Figure 1.
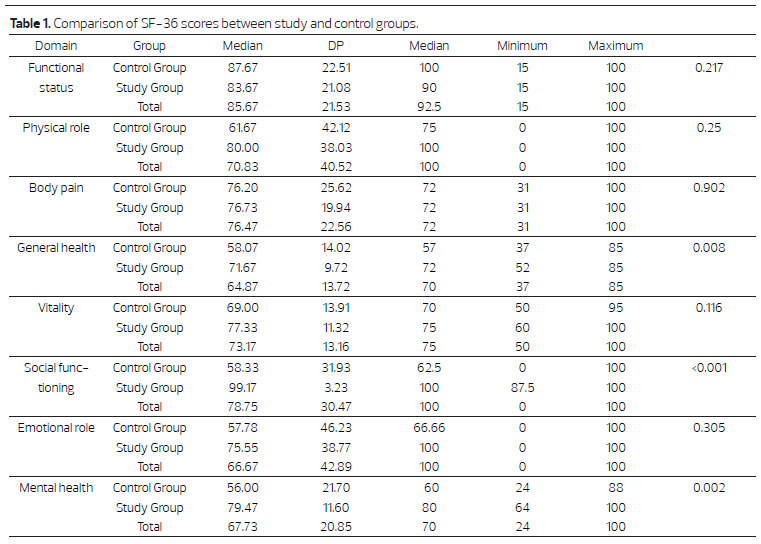

Figure 1. Median SF-36 scores for study and control groups compared to transverse myocutaneous groups (Mann-Whitney U Test).
Six months post reconstruction, SG patients had statistically significant higher scores in the general health, mental health, and social functioning domains. Despite increased scores, no statistically significant differences were found in the physical role, body pain, vitality, or emotional role domains.
DISCUSSION
Breast reconstruction should be considered an option to improve quality of life of women undergoing mastectomies. It may also contribute to their acceptance of their breast cancer diagnosis and treatment 6.
After its initial description by Hartrampf et al., TRAM flap surgery has become a widely used reconstruction technique worldwide 3. It was introduced as a proposal for allowing autologous breast reconstruction without use of prostheses while also leaving a lower abdominal scar very similar to an abdominoplasty 10.
In 2004, Veiga et al.11 published the results of a prospective study about the quality of life in patients undergoing delayed TRAM flap breast reconstruction, reporting that reconstruction had a positive effect in all SF-36 domains except in vitality 1 year after surgery. In this study, patients who had undergone mastectomies but had not yet received reconstruction comprised the control group. Based on this definition, the CG in the present study consisted of mastectomy patients who had not yet undergone reconstructive surgery.
We did not include patients older than 65 years of age because, although there is no formal contraindication for TRAM flap surgery in these patients, the Brazilian Society of Plastic Surgery recommends conducting individual assessment to guarantee risk/benefit ratios in favor of the patient 12. Because patients in the CG would receive delayed TRAM breast reconstruction, additional exclusion criteria were also applied. Obese patients (body weight >20% of ideal weight or BMI > 30kg/m2) are considered unfavorable candidates for TRAM reconstruction 12. Obesity is associated with a significant number of complications (40%), due to poor vascularization of the flap (neobreast) and complications of the donor area, either by changes resulting from circulatory failure or mechanical changes of the abdominal wall, ranging from bulging to true hernias13.
According to Hartrampf3, the presence of two risk factors is considered sufficient contraindication for TRAM flap surgery. However, the procedure may also be contraindicated when comorbidities are also considered. Therefore, patients in this study with severe and uncontrolled comorbidities (hypertension, diabetes mellitus, hypercholesterolemia, and autoimmune disease) were excluded from the CG. Smoking was another important factor considered in preoperative selection and assignment of patients in this study, as it increases the incidence of complications such as abdominal flap necrosis, hernias, and retail losses 10. These complications occur in up to 25% and 40% of nonsmokers and smokers, respectively 14.
Quality of life was measured using the Brazilian version of the SF-36 survey, which was adapted and validated for use in Brazil by Ciconelli et al. 7 in 1999.
Besides Brazil, 20 other countries have also validated the survey. The SF-36 results reflect patient views about their treatment independent of the opinions of their surgical team 14.
The SG showed better, but not statistically significant, SF-36 results in almost all domains except functional status. There was a highly significant difference in three of the eight domains (general health, mental health, and social functioning), suggesting that patients who underwent TRAM flap surgery had better quality of life compared to patients in the CG.
Pusic et al.15 compared mastectomy patients and patients undergoing breast reconstruction in a retrospective study that observed lower quality of life scores in all areas except physical health and vitality among patients who had received mastectomies. Higher scores were also observed in these areas between the SG and CG in the present study.
Brandberg et al.16 compared the effects of three methods of delayed breast reconstruction (latissimus dorsi, TRAM, and prosthesis), and observed significant improvement in social aspects and mental health domains after 12 months. The present study found no statistically significant differences between the groups within the first 6 months; however, better results were observed in the group undergoing breast reconstruction.
Ysuf et al.17 reported that ethnicity affects the quality of life values among women with breast cancer. This study compared Chinese and Malaysian women within a society and showed that quality of life scores were better among Chinese women, reinforcing the importance of ethnicity when measuring quality of life in women with breast cancer. Better understanding of ethnic differences in quality of life assessments will allow health professionals to determine how best to support and improve the quality of life for these women during the difficult moments of their illnesses and the course of their treatments.
In addition to ethnicity, clinical factors and socio-economic status must also be taken into account when assessing quality of life17.
McClellan reported the importance of exercise in survivors of breast cancer because it improves physical function and quality of life. More research on the type and intensity of exercise will help physicians prepare highly specific recommendations18.
According to Geiger19, quality of life can be improved and psychiatric disorders reduced up to 2 years after breast reconstruction in mastectomy patients as well as asymptomatic patients in the risk group who opted for prophylactic mastectomies. Technical advances in breast reconstruction are sometimes not enough to mitigate the negative psychological effects of mastectomy. Post-operative reports often note that women feel relieved not to have immediate contact with their mutilated bodies.
The results of this study are consistent with the statement by Brandberg et al.16, that all mastectomy patients should have the opportunity to receive breast reconstruction because of the positive effects on quality of life. However, the study results should be considered in light of several limitations, such as its cross-sectional design: the questionnaire would ideally be applied to pre- and postoperative patients.
One should also consider that the patients in this study were enrolled from the national health system, and may therefore have different expectations compared to patients in the private health sector who might more easily accept the results achieved by the reconstructive surgery.
More studies are needed on options and advancements that improve the quality of life of cancer patients.
The main sense won or regained by patients undergoing this reconstructive surgery is rehabilitation of social environments and life itself, both in women who have already undergone and in those who have not yet received breast reconstruction. The desire for personal and social reintegration is the most obvious explanation for the effect of this procedure 20.
It is not the responsibility of reconstructive plastic surgery to make a person more or less happy; however, this surgical procedure appears to constitute an important physical and emotional tool for mastectomy patients.
CONCLUSIONS
Quality of life scores were higher in the group of patients who underwent breast reconstruction.
REFERENCES
1. Garbay JR, Rietjens M, Petit JY. Résultats esthétiques de La reconstruction mammaire après amputation pour cancer: a propos de 323 cas. J Gynecol Obstet Biol Reprod. 1992;21(4):405-12.
2. Petit JY, Lehmann A, Mouriesse H, Rietjens M. Résultats à long terme après reconstruction mammaire. Helv Chir Acta. 1989;55(6):869-77.
3. Hartrampf CR, Scheflan M, Black PW. Breast reconstruction with a transverse abdominal island flap. Plast Reconstr Surg. 1982;69(2):216-25.
4. Gandolfo EA. Breast reconstruction with a lower abdominal myocutaneous flap. Br J Plast Surg. 1982;35(4):452-76.
5. Moscona RA, Holander L, Or D, Fodor L. Patient satisfaction and aesthetic results after pedicled transverse rectus abdominis muscle flap for breast reconstruction. Ann Surg Oncol. 2006;13(12):1739-46.
6. Harcourt D, Rumsey N. Psychological aspects of breast reconstruction: a review of the literature. J Adv Nurs. 2001;35(4):477-87.
7. Ciconelli RM, Ferraz MB, Santos W, Meinão I, Quaresma MR. Tradução para a língua portuguesa e validação do questionário genérico de avaliação de qualidade de vida SF-36 (Brasil SF-36). R Bras Reumatol. 1999;39(3):143-50.
8. de Brito MJ, Nahas FX, Barbosa MV, Dini GM, Kimura AK, Farah AB, Ferreira LM. Abdominoplasty and its effect on body image, self-esteem, and mental health. Ann Plast Surg. 2010;65(1):5-10.
9. Kirkwood BR, STERNE JAC. Essential Medical Statistics. 2nd ed. Massachusetts (USA): Blackwekk science; 2006.
10. Mélega JM. Cirurgia Plástica - Fundamentos e Arte IV - Cirurgia Reparadora de Tronco e e Membros. 1ª.ed. Rio de Janeiro: Guanabara Koogan; 2004.
11. Veiga DF, Sabino NetoM, Ferreira LM, Garcia EB, Veiga filho J, Novo NF, Rocha JL. Quality of life outcomes after pedicled TRAM flapdelayed breast reconstruction, BR J Plast Surg. 2004;57(3):252-7.
12. Carreirão S, Cardim V, Goldenberg D. Cirurgia Plástica Sociedade Brasileira de Cirurgia Plástica. 1ª.ed. São Paulo: Atheneu; 2005.
13. Kroll SS, Marchi M. Comparison of strategies for preventing abdominal-wall weakness after TRAM flap breast reconstruction. Plast Reconstr Surg. 1992;89(6):1045-51.
14. Chang DW, Reece GP, Wang B, Robb GL, Miller MJ, Evans GR, et al. Effect of smoking on complications in patients undergoing free TRAM flap breast reconstruction. Plast Reconstr Surg. 2000;105(7):2374-80.
15. Pusic A, Thompson TA, Kerrigan CL, Sargeant R, Slezak S, Chang BW, Kelzlsouer KJ, Manson PN. Surgical options for the early-stage breast cancer: factors associated with patient choice and postoperative quality of life. Plast Reconstr Surg. 1999; Oct;104(5):1325-33.
16. Brandberg Y, Malm M, Blomqvist L. A prospective and randomized study, "SVEA," comparing effects of three methods for delayed breast reconstruction on quality of life, patient-defined problem areas of life, and cosmetic result. Plast Reconstr Surg. 2000;105(1):66-74.
17. Yusuf A, Ahmad Z, Keng SL. Quality of life in Malay and Chinese women newly diagnosed with breast cancer in Kelatan, Malaysia. Asian Pac J Cancer Prev. 2013;14(1):435-440.
18. McClellan R. Exercise programs for patients with cancer improve physical functioning and quality of life. J Physiother. 2013;59(1):57.
19. Geiger AM, West CN, Nekhlyudov L et al. Contentment with quality of life among breast cancer survivors with and without contralateral prophylactic mastectomy. J Clin Oncol. 2006;24:1350-56.
20. Souza AMF. Informacões, sentimentos e sentidos relacionados à reconstrucao mamária [Dissertação]. Rio de Janeiro: fundação Oswaldo Cruz, 2008.
1 - Full Member of the Brazilian Society of Plastic Surgery - Assistant Physician, Department of Plastic Surgery, Women's Health Reference Center - Pérola Byington Hospital
2 - MSc in Plastic and Reconstructive Surgery, Federal University of Sao Paulo (UNIFESP) - Assistant Physician, Department of Plastic Surgery, Women's Health Reference Center - Pérola Byington Hospital
3 - MSc in Plastic and Reconstructive Surgery, Federal University of Sao Paulo (UNIFESP) - Assistant Physician, Department of Plastic Surgery, Women's Health Reference Center - Pérola Byington Hospital
4 - PhD in Plastic Surgery from the Federal University of São Paulo (UNIFESP) - Pro-Rector for Graduate Studies and Research at the University of Vale do Sapucai, Supervisor of the Graduate Program in Plastic Surgery, UNIFESP
5 - PhD in Plastic Surgery from the Federal University of São Paulo (UNIFESP) - Professor and Supervisor of the Post-Graduate Program in Plastic Surgery, UNIFESP, and Technical Director Department of Plastic Surgery, Women's Health Reference Center - Pérola Byington Hospital
6 - Lecturer in Mastology at the Federal University of São Paulo - UNIFESP - Head Director, Women's Health Reference Center - Pérola Byington Hospital
7 - Lecturer at the Federal University of São Paulo (UNIFESP) - Full Professor of Plastic Surgery, UNIFESP; Coordinator Med III CAPES (2011-2014) and Coordinator, Post-Graduate Program in Plastic Surgery, UNIFESP
Institution: Women's Health Reference Center - Pérola Byington Hospital
Corresponding author:
João Carlos Rondelo
Rua: Água Rasa, 83, apto 44, Vila Regente Feijó
CEP: 03343-010. São Paulo - SP, Brasil
E-mail: jcrondelo@uol.com.br
Article received: August 2, 2013
Article accepted: October 30, 2014
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket