



Original Article - Year 2013 - Volume 28 -
Morphometric analysis of the upper lip and the action of ageing
Análise morfométrica do lábio superior e da ação do envelhecimento
ABSTRACT
BACKGROUND: A pleasant smile depends on harmonious relationships between the teeth, gums, and lips. The present study measured upper lip changes related to ageing using a morphometric analysis.
METHODS: Forty-six Caucasian women at least 15 years of age were selected and divided into four groups: 15 - 30 years old, 31 - 45 years old, 46 - 60 years old, and > 60 years old. Frontal photographs with closed lips and parted lips were taken. The following measurements were performed: upper lip height, upper vermilion height in parted and closed lips positions, and exposure of the central upper incisors in the relaxed position.
RESULTS: Upper lip height increased with age. The average upper lip height in the closed lips position was 13.75 mm in the youngest age-range (15 - 30 years old). The upper lip height gradually increased with age until reaching an average of 19.24 mm was observed in the > 60 years old group. The opposite result was observed in upper vermilion height, which decreased with increasing age. The average vermilion height in the parted lips position was 7.09 mm in the youngest age-range (15-30 years old) and decreased to 4.58 mm in the oldest group (> 60 years old). Teeth exposure decreased with age. The average upper teeth exposure was 3.55 mm in the youngest group and decreased to 0.40 mm in the oldest group.
CONCLUSION: The upper lip height increases, while the upper vermilion height and exposure of the upper teeth decrease with age.
Keywords: Lip. Aging. Age Groups.
RESUMO
INTRODUÇÃO: Um sorriso considerado agradável envolve relações harmônicas entre os dentes, gengivas e lábios. O presente estudo mediu as alterações no lábio superior, relacionadas ao envelhecimento, utilizando análise morfométrica.
MÉTODO: Foram selecionadas 46 mulheres caucasianas com idade mínima de 15 anos e divididas em quatro grupos: 15-30 anos, 31-45 anos, 46-60 anos e > 60 anos. Foram tiradas fotografias frontais com a boca fechada e na posição de repouso. As seguintes medidas foram realizadas: altura do lábio superior, altura do vermelhão do lábio superior nas posições repouso e fechada, e exposição dos dentes incisivos superiores centrais na posição repouso.
RESULTADOS: A altura do lábio superior aumentou com a idade. A média da altura do lábio superior com a boca fechada foi 13,75 mm na faixa etária mais nova (15-30 anos). A altura do lábio superior gradualmente aumenta com a idade até atingir uma média de 19,24 mm, observada no grupo > 60 anos. O resultado oposto foi observado na altura do vermelhão superior, que diminuiu com o aumento da idade. A altura média do vermelhão com a boca em repouso foi 7,09 mm na faixa etária mais nova (15-30 anos) e diminuiu para 4,58 mm no grupo mais velho (> 60 anos). A exposição dos dentes diminuiu com a idade. A exposição média dos dentes superiores foi de 3,55 mm no grupo mais jovem e diminuiu para 0,40 mm no grupo mais velho.
CONCLUSÃO: A altura do lábio superior aumenta, enquanto a altura do vermelhão superior e a exposição dos dentes superiores diminuem com a idade.
Palavras-chave: Lábio. Envelhecimento. Grupos Etários.
The importance of a pleasant smile is undeniable. The influence of facial attractiveness and smile has been demonstrated at professional and social levels1. A pleasant smile depends on harmonious relationships between the teeth, gums, and lips2. The upper lip and its dynamics are essential components of a beautiful smile and facial balance3,4.
The upper lip and face are affected by ageing, which produces several anatomical, functional, and morphometric alterations5. In this study, we aimed to measure upper lip changes related to ageing using a morphometric analysis.
METHODS
Forty-six Caucasian women at least 15 years of age were selected and divided into four groups: 15 - 30 years old, 31 - 45 years old, 46 - 60 years old, and > 60 years old. Women with severe craniofacial changes or who received any surgical procedures on the upper lip were excluded.
The participants underwent photographic assessment using the open-access software, Image J6. Frontal photographs with closed lips and parted lips were taken (Figure 1). The following measurements were performed: upper lip height, upper vermilion height in parted and closed lips positions, and exposure of the central upper incisors in the relaxed position (Figure 2). The results were analyzed using one-factor analysis of variance (ANOVA). Significant differences between pairs were compared using the Bonferroni test.

Figure 1 - "Closed lips" position (A) and "Parted lips" position (B) with the measured parameters.
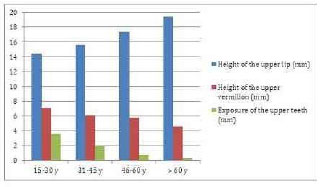
Figure 2 - Graph comparing the height of upper lip (blue), height of the upper vermilion Figure 2 - Graph comparing the height of upper lip (blue), height of the upper vermilion (red) and exposure of the upper teeth (green) in each group.
RESULTS
Upper lip height increased with age (Table 1). The average upper lip height in the closed lips position was 13.75 mm in the youngest age-range (15 - 30 years old). The upper lip height gradually increased with age until reaching an average of 19.24 mm was observed in the > 60 years old group.
The opposite result was observed in upper vermilion height, which decreased with increasing age (Table 2). The average vermilion height in the parted lips position was 7.09 mm in the youngest age-range (15-30 years old) and decreased to 4.58 mm in the oldest group (> 60 years old).
The exposure of the upper teeth exhibited the same tendency as the lip vermilion. Teeth exposure decreased with age (Table 3). The average upper teeth exposure was 3.55 mm in the youngest group and decreased to 0.40 mm in the oldest group.
Significant differences (P<0.002) were observed between all groups and all investigated parameters (Tables 1, 2, and 3).
DISCUSSION
The upper lip undergoes a proliferative stage that begins at birth and ends at puberty. This stage is characterized by muscle and gland hypertrophy, which produces full, everted, and well-defined lips. A gradual process of atrophy and sagging of structures begins after puberty due to the thinning and stretching of the skin, hypotrophy of the bones and teeth, and hypotonia and hypotrophy of muscles and glands7,8.
The ageing process involves intrinsic and extrinsic factors. Several factors in intrinsic ageing produce important alterations in the dermis. Reductions in glycosaminoglycans and proteoglycans result in the loss of dermal volume and turgor. The proportion and absolute amount of type I and type III collagen decreases, and the elastic fibers become thinner and fragmented. These changes reduce the quantity and quality of dermal collagen9.
Extrinsic factors, such as actinic damage and smoking, accelerate the ageing process, which may be visibly observed as an elongation of the upper lip with a consequent reduction in the exposure of the upper teeth. Concomitantly, the lip vermilion becomes less exposed due to its internal rotation, which is due to the elongation of the upper lip that is associated with the hypotrophy of the vermilion itself10.
These anatomical-morphometric changes are depicted in Figure 1. The upper lip height increases with age, but teeth exposure and upper lip length decrease.
The reduction in teeth exposure in the older age groups tends to be more important than indicated by the values that were obtained in the present study. The reason for this difference is that the participants in the present study who exhibited no teeth exposure were recorded as 0 mm, but these participants actually exhibited negative values of teeth exposure. The present study adopted this criterion because it was not possible to measure negative exposures of the upper teeth in photographic assessments.
The importance of changes in the upper lip caused by aging is demonstrated in this study. These anatomical-morphometric alterations must be considered by surgeons in the treatment of facial ageing and the smile8,11,12.
CONCLUSIONS
The upper lip height increases, while the upper vermilion height and exposure of the upper teeth decrease with age.
REFERENCES
1. Stevenage SV, McKay Y. Model applicants: the effect of facial appearance on recruitment decisions. Br J Psychol. 1999;90(2):221-34.
2. Desai S, Upadhyay M, Nanda R. Dynamic smile analysis: changes with age. Am J Orthod Dentofacial Orthop. 2009;136(3):310.e1-10.
3. Dong JK, Jin TH, Cho HW, Oh SC. The esthetics of the smile: a review of some recent studies. Int J Prosthodont. 1999;12(1):9-19.
4. Ishida LH, Ishida LC, Ishida J, Grynglas J, Alonso N, Ferreira MC. Myotomy of the levator labii superioris muscle and lip repositioning: a combined approach for the correction of gummy smile. Plast Reconstr Surg. 2010;126(3):1014-9.
5. Van der Geld P, Oosterveld P, Kuijpers-Jagtman AM. Age-related changes of the dental aesthetic zone at rest and during spontaneous smiling and speech. Eur J Orthod. 2008;30(4):366-73.
6. Abramoff MD, Magalhães PJ, Ram SJ. Image processing with ImageJ. Biophotonics Int. 2004;11(7):36-42.
7. Rubin LR, Mishriki Y, Lee G. Anatomy of the nasolabial fold: the keystone of the smiling mechanism. Plast Reconstr Surg. 1989;83(1):1-10.
Rev. Bras. Cir. Plást.2013; Vol. 28 (No.4 ) 592 www.rbcp.org.br 8. Austin HW, Weston GW. Rejuvenation of the aging mouth. Clin Plast Surg. 1992;19(2):511-24.
9. Maloney BP. Aesthetic surgery of the lip. In: Papel ID, ed. Facial plastic and reconstructive surgery. 2nd ed. New York: Thieme Medical Publishers; 2002. p.344-52.
10. Gonzalez-Ulloa M. The aging of the upper lip. In: Marshac D, Hueston JT, eds. Transactions of the Sixth International Congress of Plastic and Reconstructive Surgery. Paris: Masson; 1975.
11. Hinderer UT. Aging of the upper lip: a new treatment technique. Aesthetic Plast Surg. 1995;19(6):519-26.
12. Guerrissi JO. Surgical treatment of the senile upper lip. Plast Reconstr Surg. 2000;106(4):938-40.
1. Plastic Surgeon. Member of the Sociedade Brasileira de Cirurgia Plástica/Brazilian Society of Plastic Surgery (SBCP), São Paulo, SP, Brazil
2. Doctorate in Plastic Sugery. Assistant physician, Department of Plastic Surgery, Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (HCFMUSP), São Paulo, SP, Brazil
3. Aspirant member of the SBCP. Aspirant member of the SBCP, Resident physician, Department of Plastic Surgery, HCFMUSP, São Paulo, SP, Brazil
4. Full professor. Associate professor at the Division of Plastic Surgery of the Department of Surgery of HCFMUSP
5. Full professor - Associate professor at the Division of Plastic Surgery of the Department of Surgery of HCFMUSP
6. Titular professor of Plastic Surgery Discipline at Medicine College of Universidade de São Paulo, Chief of Plastic Surgery Division of HCFMUSP, São Paulo, SP, Brazil
Marco Vinicius Losso Longo
Avenida Dr. Arnaldo, number 455 - 1363
CEP: 01246-903. São Paulo, SP, Brazil
Article recceived:20/10/2013
Article accepted:30/11/2013
Work performed at Hospital das Clinicas, Faculty of Medicine, USP, São Paulo, SP, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket