



Ideas and Innovation - Year 2013 - Volume 28 -
Sundfeld-Reis suture for the correction of auricular axis and ear upper pole using otoplasty: preliminary note
Descrição do ponto de Sundfeld-Reis para correção do eixo auricular e polo superior da orelha em otoplastia: nota prévia
ABSTRACT
Prominent ears are among the most frequent anomalies that affect the head and neck regions and present with conchal disproportionality and/or the lack of an antihelix curvature. A wide spectrum of techniques for the correction of these deformities has been published; the most commonly cited are the techniques from Pitanguy, Converse, Stenvers, Stenstroem, Mustardé, Furnas, and Horlock. All of these techniques seek to restore facial harmony with proportional scaling of the pinna, a suitable cephaloauricular angle, and natural curvature of the antihelix. After reviewing the literature, the present study aims to describe a new technique for correcting the auricular axis and ear upper pole with a suture in the portion of the helical crus known as the Sundfeld-Reis technique. According to Adamson et al., this technique provides better positioning of the ear's upper pole in relation to the temporal pole without the need for suturing the triangular fossa region in the periosteum of the temporal bone. Therefore, using the Sundfeld-Reis technique, the pinna is placed parallel to the nasal dorsum, providing a natural result after otoplasty. The proposed technique is the latest possibility in the world of otoplasty that attains more natural results with fewer surgical interventions.
Keywords: External ear/surgery. Plastic surgery/methods. Otologic surgical procedures.
RESUMO
Dentre as diferentes anomalias que acometem as regiões de cabeça e pescoço, as orelhas em abano se encontram entre as mais frequentes, apresentando desproporcionalidade conchal e/ou falta de curvatura da antélice. Existe na literatura um grande espectro de técnicas para a correção dessas deformidades, citando-se como as mais consagradas as técnicas de Pitanguy, Converse, Stenvers, Stenstroem, Mustardé, Furnas e Horlock. Todas essas técnicas buscam restaurar a harmonia da face com proporcional dimensionamento do pavilhão auricular, ângulo aurículo-cefálico adequado e curvatura de antélice natural. Após revisão da literatura, o presente estudo pretende descrever uma nova técnica para correção do eixo auricular e o polo superior da orelha com uma sutura na porção do ramo da hélice, descrita como técnica de Sundfeld-Reis. Tal técnica proporciona melhor posicionamento do polo superior da orelha em relação ao temporal, sem a necessidade da sutura realizada na região da fossa triangular no periósteo do osso temporal, como orientado por Adamson et al. Outrossim, com o ponto de Sundfeld-Reis há posicionamento do pavilhão auricular paralelo ao dorso nasal, proporcionando um resultado natural da otoplastia. A proposta técnica se fulgura como mais uma possibilidade arregimentada no universo da otoplastia, vislumbrando resultados mais naturais, com menores intervenções cirúrgicas.
Palavras-chave: Orelha externa/cirurgia. Cirurgia plástica/métodos. Procedimentos cirúrgicos otológicos.
Historically, the face has represented one of the main means of communication and features the backdrop of expressions for feelings and emotions. This can be observed in known works such as "La Gioconda" by Leonardo da Vinci during the Italian Renaissance movement and "The Scream (Skrik)" by Edvard Munch during the expressionist movement.
The external ear is a highly important structure in the harmony of the face. Prominent ear, affecting approximately 5% of the general population, is the most common congenital deformity of the outer ear1. This deformity is transmitted in an autosomal dominant mode, and regardless of its benign physiological consequences, several studies have demonstrated associated psychological distress, emotional trauma, and behavioral changes, especially in children2.
A wide spectrum of techniques has been described for correcting prominent ears and can be grouped into the following categories: with incision and suture3, suture only4, cartilage removal techniques5-7, and others combining some of those previously mentioned8. Despite the large amount of corrective techniques, new proposals can be developed because there is no ideal method for correcting prominent ears.
Knowledge of the embryology and anatomy of the external ear is essential to achieving good surgical results in otoplasty. The pinna develops from six mesenchymal proliferations around the fifth gestational week, known as the hillocks of His, which are located in the dorsal region of the first and second branchial arches. Subsequently, the hillocks fuse around the dorsal region of the first pharyngeal cleft forming the pinna. Each hillock contributes to the formation of a specific structure in the external ear. The outer ear migration from the cervical region to the side of the skull occurs during fetal development9.
The sensory and motor innervation of the external ear is represented by the following nerves innervating the muscles of the external ear: auricular branch of the vagus nerve (X); greater auricular nerve with its anterior and posterior branches (C2/C3); mandibular nerve (V); auriculotemporal nerve; nerve of the external acoustic meatus; auricular branch of the facial nerve (VII); and posterior auricular nerve10.
The external ear is a complex structure composed primarily of skin and cartilage that consists of five main elements, including the concha, helix, antihelix, tragus, and lobule. Other portions of lesser importance include the antitragus, incisura intertragica, and Darwin's tubercle (Figure 1). The partition of the ear can be embryologically understood through the branchial arches. The second branchial arch is the main collaborator in the formation of the ear, contributing to the formation of the helix, scapha, antihelix, concha, antitragus, and lobule, whereas the first branchial arch contributes only to the formation of the tragus and helical crus.
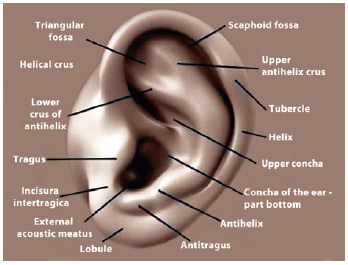
Figure 1 - Auricular anatomy showing the helical crus between the superior and inferior portion of the concha where the Sundfeld-Reis suture is performed.
The innervation of the external ear, as pictured above, follows the distribution of the branchial arches and consists of the anterior and posterior branches of the greater auricular nerve, which innervates the structures that arise from the first branchial arch (tragus and helical crus), and the auriculotemporal nerve, which innervates structures arising from the second branchial arch (helix, scapha, antihelix, concha, antitragus, external acoustic meatus, and lobule). The external acoustic meatus is also innervated by branches of the vagus and glossopharyngeal nerves11.
Blood is supplied to the external ear through the posterior auricular and occipital branches of the external carotid artery and the anterior auricular branch of the superficial temporal artery. The pinna has several ligaments and muscles, namely the helicis major, helicis minor, tragicus muscle, and antitragicus muscle on the anterior side and the superior auricular ligament, oblique muscle of the ear, transverse muscle of the ear, and posterior auricular ligament on its posterior surface10.
The ideal positioning of the external ear in relation to the other components of the face contributes to a harmonious and ideal aesthetic appearance. In an anteroposterior view, the desired cephaloauricular angle should be 15-30º and is considered optimal at 25-30º. The distance from the edge of the helix to the mastoid should be 15-20 mm. The pinna's vertical orientation should be strictly parallel to the nasal dorsum. A horizontal line extending from the inferior orbital margin should be level with the top edge of the tragus12.
Other parameters used to characterize prominent ears are the distances from the lateral border of the helix to the temporal and mastoid region in a perpendicular line in the range of 10-12 mm in the upper pole, 15-25 mm in the midportion, and 20-22 mm in the lower pole. These measures vary widely according to body type, age, and racial group13.
Some of the main causes of prominent ears are: excessive or hypertrophic concha (upper pole, lower pole, or both); inadequate formation of the antihelix projection (antihelix base, superior crus, lower crus, or all); scaphoconchal angle > 90º; and a combination of concha hypertrophy with incomplete antihelix development. Other causes may include cranial abnormalities (which may influence the evaluation of the base where the ear sits), protruding lobule, and anterolateral dislocation of the helix tail14.
Despite the existence of several techniques in the literature for the correction of prominent ears, there is no consensus on the ideal one for otoplasty; many techniques show numerous variations and have persisted over time. A technique consisting of a suture at the helical crus - the Sundfeld-Reis technique - seeks to offer a new surgical method for improved composition and harmony after otoplasty; it is a simple technique but has recognized complications.
The aim of this study is to describe the Sundfeld-Reis technique performed on the helical crus to correct the upper auricular pole and auricular axis.
METHOD
Patients with unilateral or bilateral prominent ears, without craniofacial and auricular malformations (microtia), who were >15 years were selected for this study. All patients were informed about the surgical procedures, risks, and possible complications. Terms of consent for surgery, participation in the study, and use of collected images were signed. All procedures were performed according to the protocols and determinations of the Research Ethics Committee from the Paulista School of Medicine - Federal University of São Paulo.
After medical consultations, patients were taken to the operating room. Markings on the front and back of the external ear were performed to indicate the locations for Sundfeld-Reis sutures. Patients were positioned supine after aqueous chlorhexidine antisepsis and underwent local anesthesia with an anesthetic solution (lidocaine 2% 40 mL without epinephrine, 60 mL of isotonic saline, 0.5 mL of adrenaline; 1:200,000 solution). Anesthetic infiltration was performed subcutaneously along the posterior and anterior portions and anterior portion of the external acoustic meatus for a total anesthetic block. Approximately 10 minutes were allowed to elapse for vasoconstriction peaking resulting from the local effect of the injected adrenaline. No sedation or general anesthesia was employed in the patients included in this study. Sterile fields positioned on the head were used to allow lateral rotation with ear exposure for comparison and symmetry of results. First-generation cephalosporin was used as the antibiotic prophylaxis, maintained for 7 days postoperatively.
After excision of the posterior portion of the ear skin dissected down to the posterior perichondrium, a dissection was carried out to the edge of the helix along the pinna's length. Dissection of the mastoid and rigorous hemostasis was subsequently performed. The proposed technique, called a Sunfeld-Reis structure, which recommends the passage of a suture with black 3.0 nylon monofilament in the helical crus, was performed between the concha at its upper and lower portion (Figure 2).

Figure 2 - Creation of the Sundfeld-Reis suture.
After this suture was created, the resulting effects (Figure 3) were observed. If the pinna was already in a harmonious position in its upper pole with its vertical axis parallel to the nasal dorsum, we proceeded with passing Mustardé sutures with colorless 4.0 nylon monofilament to form the antihelix and Furnas sutures with black 3.0 nylon monofilament. The procedures described here were repeated in the contralateral ear and the sides were compared to ensure symmetry. Subsequent incisions were sutured with black 4.0 monofilament nylon in a continuous suture after further review of hemostasis.
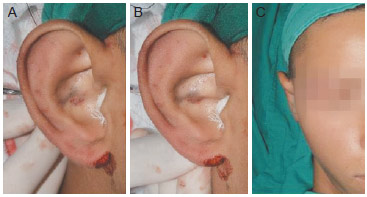
Figure 3 - Final appearance after creation of the Sundfeld-Reis suture. A, external ear without tension in the Sundfeld-Reis suture. B, external ear showing the effect of the Sundfeld-Reis suture. C, part of the external ear after the Sundfeld-Reis and modified Furnas sutures are placed.
A containment dressing was applied with bandaging molding of the external ear with sterile cotton. The dressing was removed on the first postoperative day and replaced by an otoplasty elastic band.
Follow-up visits were conducted on the 1st, 7th, and 14th days postoperatively and at 1, 3, 6, and 12 months after surgery. All patients were photographed at every visit for later comparison of the outcomes. The occurrence of complications such as infection, hematoma, tissue necrosis, pressure ulcers, feeling of paresthesia, wound dehiscence, recurrence of prominence, and extruding sutures were evaluated at every patient's follow-up visit.
RESULTS
Recurrence, dehiscence, infection, hematoma, and necrosis of cartilage and/or tissue were not observed in the first 6 postoperative months (Figure 4). Complaints of slight numbness in the auricular region were reported by 33% of patients at 3 months postoperatively. Figures 5-10 illustrate some cases in this series.
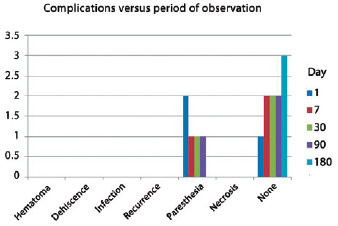
Figure 4 - Complications observed throughout the follow-up visits.

Figure 5 - Preoperative view of patient 1 on the 7th and 180th postoperative days.

Figure 6 - Preoperative view of patient 2 on the 1st and 180th postoperative days.

Figure 7 - Preoperative view of patient 3 on the 7th and 180th postoperative days.
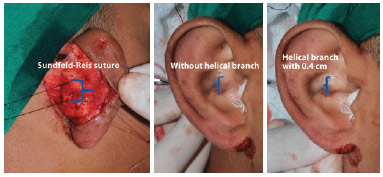
Figure 8 - Effect of the Sundfeld-Reis suture placed at the helical crus to create its curvature.
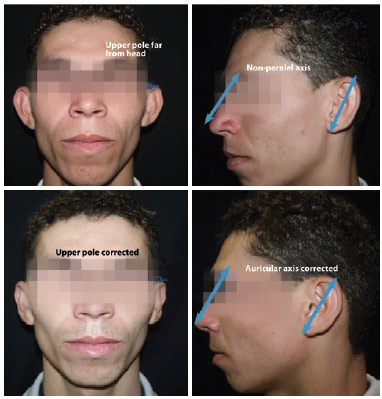
Figure 9 - Final appearance after the Sundfeld-Reis suture application. Note the correction of the upper pole and auricular axis to a position parallel to the nasal dorsum.

Figure 10 - Correction of the upper pole and auricular axis. Final appearance after the Sundfeld-Reis suture is applied in different patients that corrected the upper pole and auricular axis.
DISCUSSION
Forged over time, the different otoplasty techniques used to date are increasingly current. In 1845, Dieffenbach15 described the first case of otoplasty performed on a patient with posttraumatic sequelae for which he performed resection of the post-auricular skin and concha mastoid fixation as the form of treatment.
In 1881, Ely16 described his technique in elective otoplasties in which he performed an excision in the post-auricular skin, conchamastoide suture, and excision of a conchal cartilage strip. This procedure is performed in two surgical moments. Luckett17 analyzed the literature reviews by Keen, Cocheril, and Gersuny and stressed the importance of the creation and restoration of the antihelix shape in otoplasty procedures. Luckett also introduced the revolutionary concept of manipulating the auricular cartilage to obtain a natural shape. In creating the antihelix, he used a posterior access and performed cartilage resection with subsequent union of edges. In 1952, Becker18 introduced a concept using incisions associated with cartilage sutures to obtain a smoother antihelix shape.
The approach used by Mustardé4 in 1963 intended to create a new antihelix based on permanent sutures via posterior access with sutures encompassing the anterior perichondrium without transfixing the skin. In 1963, Stenstroem5 developed a technique of scraping the anterior surface to achieve a smoother contour in the antihelix. Deformities of the concha can be corrected through several corrective methods including excision, abrasion, and fixing of the cartilage. Techniques using sutures were initially described by Owens and Delgado19 in 1955.
In 1968, Furnas20 modified the technique from Owens and Delgado of creating sutures with non-absorbable threads placed in the conchal cartilage, transfixed up to the anterior perichondrium, and sutured to the mastoid fascia. The technique from Furnas gained great popularity for its simplicity and easy reproducibility; however, as with several other techniques, it was modified by Spira et al.21 in 1969.
The Sundfeld-Reis technique presents a simple solution for correcting the upper auricular pole and auricular axis with complication rates comparable to previously published results. It also boasts harmonious aesthetic results without increased relapse rates. As such, we emphasize that the Sundfeld-Reis approach does not resemble any technique described in the literature, is simple and easily reproducible, and shows satisfactory long-term results and better facial harmony. The technique proposed herein provides harmonious and reproducible results and correction of the upper ear pole and axis that increase patient satisfaction.
We highlight that one of the limitations of this study is the lack of result comparison with other techniques for the correction of the upper pole. Nevertheless, there is a prospect for conducting a clinical trial that compares the Sundfeld-Reis technique with that of Adamson et al.22.
CONCLUSIONS
The Sundfeld-Reis technique described herein with a suture performed on the helical crus represents a simple and reproducible procedure for the correction of the ear upper pole and auricular axis to make it parallel to the nasal dorsum without the need for suturing on the triangular fossa or temporal fascia as projected by Adamson et al.22 for correcting the upper pole. Additionally, the technique does not result in increased complication rates.
REFERENCES
1. Janis JE, Rohrich RJ, Gutowski KA. Otoplasty. Plast Reconstr Surg. 2005;115(4):60e-72e.
2. Macgregor FC. Ear deformities: social and psychological implications. Clin Plast Surg. 1978;5(3):347-50.
3. Converse JM, Nigro A, Wilson FA, Johnson N. A technique for surgical correction of lop ears. Plast Reconstr Surg. 1955;15(5):411-8.
4. Mustardé JC. The correction of prominent ears using simple mattress sutures. Br J Plast Surg. 1963;16:170-8.
5. Stenstroem SJ. A "natural" technique for correction of congenitally prominent ears. Plast Reconstr Surg. 1963;32:509-18.
6. Ju DM, Li C, Crikelair GF. The surgical correction of protruding ears. Plast Reconstr Surg. 1963;32:283-93.
7. Chongchet V. A method of antihelix reconstruction. Br J Plast Surg. 1963;16:268-72.
8. Schlegel-Wagner C, Pabst G, Müller W, Linder T. Otoplasty using a modified anterior scoring technique: standardized measurements of long-term results. Arch Facial Plast Surg. 2010;12(3):143-8.
9. Sadler TW. Ear. In: Sadler TW, ed. Langman's medical embryology. 6th ed. Baltimore: Williams & Wilkins; 1990.
10. Putz R, Pabst R. Sobotta Atlas de anatomia humana. Vol. 1. 21ª ed. Rio de Janeiro: Guanabara Koogan; 2000. p. 382-3.
11. Tolleth H. Artistic anatomy, dimensions, and proportions of the external ear. Clin Plast Surg. 1978;5(3):337-45.
12. Spira M. Otoplasty: what I do now. A 30-year perspective. Plast Reconstr Surg. 1999;104(3):834-41.
13. Stucker FJ, Vora NM, Lian TS. Otoplasty: an analysis of technique over a 33-year period. Laryngoscope. 2003;113(6):952-6.
14. Webster GV. The tail of the helix as a key to otoplasty. Plast Reconstr Surg.1969;44(5):455-61.
15. Dieffenbach JE. Die operative chirurgie. Leipzig: F. A. Brockhause; 1845.
16. Ely ET. An operation for prominent auricles. Arch Otolaryngol. 1881;10:97 (reprinted in Plast Reconstr Surg. 1968;42:582).
17. Rogers BO. The classic reprint. A new operation for prominent ears based on the anatomy of the deformity by William H. Luckett, M.D. (reprinted from Surg. Gynec. & Obst., 10:635-7, 1910). Plast Reconstr Surg. 1969;43(1):83-6.
18. Becker OJ. Correction of the protruding deformed ear. Br J Plast Surg. 1952;5(3):187-96.
19. Owens N, Delgado DD. The management of outstanding ears. South Med J. 1955;58:32-3.
20. Furnas DW. Correction of prominent ears by conchamastoid sutures. Plast Reconstr Surg. 1968;42(3):189-93.
21. Spira M, McCrea R, Gerow FJ, Hardy SB. Correction of the principal deformities causing protruding ears. Plast Reconstr Surg. 1969;44(2):150-4. 22. Adamson PA, McGraw BL, Tropper GJ. Otoplasty: critical review of clinical results. Laryngoscope. 1991;101(8):883-8.
1. Resident Physician in Plastic Surgery, Escola Paulista de Medicina/Universidade Federal de São Paulo (EPM/UNIFESP), Aspiring Training Member of the Brazilian Society of Plastic Surgery (BSPS), São Paulo, SP, Brazil
2. Plastic Surgeon, Associate Member of the BSPS, Maringa, PR, Brazil
3. Plastic Surgeon, Associate Member of the BSPS, Coordinator of AME Maria Zelia - Plastic Surgery EPM/UNIFESP, São Paulo, SP, Brazil
4. Plastic Surgeon, Full Professor in the Department of Plastic Surgery, EPM/UNIFESP, Full Member of the BSPS, São Paulo, SP, Brazil
Correspondence to:
Daniel Sundfeld Spiga Real
Rua Pedro de Toledo, 544 - ap. 600 - Vila Clementino
São Paulo, SP, Brazil - CEP 04039-001
E-mail: daniel.ssr@hotmail.com
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: 9/10/2012
Article accepted: 1/6/2013
Work performed at the Escola Paulista de Medicina/Universidade Federal de São Paulo, São Paulo, SP, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket