



Original Article - Year 2013 - Volume 28 -
Neoomphaloplasty using an X-shaped incision in 401 consecutive abdominoplasties
Neo-onfaloplastia com incisão em X em 401 abdominoplastias consecutivas
ABSTRACT
BACKGROUND: The search for a natural-looking umbilicus that does not compromise the aesthetic results of abdominoplasty began in the 1950s. Since then, the umbilical transposition technique has remained the preferred method among most surgeons. The objective of this study was to describe a new technique for umbilical reconstruction using small X-shaped incisions in the abdominal skin to create 4 small V-shaped flaps. These flaps are then sutured to the aponeurosis using absorbable sutures.
METHODS: This technique was used in 401 consecutive abdominoplasties and a survey was conducted to determine the level of patient satisfaction with the aesthetic results of their umbilicus.
RESULTS: Remarkably natural-looking umbilici were obtained using the described technique, which was also easily reproducible, did not cause any apparent scars, had a low incidence of complications (9.7%), and resulted in high patient satisfaction with the aesthetic results of the surgery.
CONCLUSIONS: The described technique represented a simple, safe, and fast approach to create new, natural-looking umbilici with a low rate of complications.
Keywords: Umbilicus. Scar. Abdomen/surgery. Abdominoplasty.
RESUMO
INTRODUÇÃO: A procura por um umbigo de aspecto natural, que não comprometa o resultado estético das abdominoplastias, começou na década de 1950 e, desde então, a técnica de transposição umbilical é a preferida pela maioria dos cirurgiões. O objetivo deste artigo é descrever nova técnica de reconstrução umbilical, utilizando pequenas incisões em forma de X na pele abdominal, que criam 4 pequenos retalhos em forma de V, os quais são suturados à aponeurose com suturas absorvíveis.
MÉTODO: Essa técnica foi utilizada em 401 abdominoplastias consecutivas e foi realizada uma pesquisa para determinar o nível de satisfação dos pacientes com o resultado estético dos umbigos.
RESULTADOS: Foram criados umbigos extremamente naturais, de maneira facilmente reprodutível e sem cicatrizes aparentes, com baixa incidência de complicações (9,7%) e alto índice de satisfação dos pacientes.
CONCLUSÕES: A técnica utilizada permitiu a criação de um novo umbigo com aparência natural, de maneira simples, segura e rápida, com baixo índice de complicações.
Palavras-chave: Umbigo. Cicatriz. Abdome/cirurgia. Abdominoplastia.
Abdominoplasty has been performed for over a century and was initially described by Kelly.1
During the 1950s, Andrew and Vernon developed a technique for reconstruction of the umbilical scar, while highlighting the importance of this procedure because of the emotional discomfort associated with the removal of the umbilicus.1-3 Since then, the umbilical transposition technique has become a fundamental step of abdominoplasty.
However, frequent complications associated with periumbilical incisions, such as hypertrophy and stenosis, have led surgeons to attempt new techniques utilizing different types of incisions around the umbilicus and surrounding abdominal flaps.
During the 1970s, Regnault1 and Baroudi4 described the use of horizontal incisions in the flap, whereas Avelar5 proposed the use of a star-shaped incision in 1978. These approaches resulted in a lower risk of stenosis.
Several incision techniques have been proposed, including a V-shaped incision as suggested by Juri et al.,6 a circular incision in the umbilicus and a triangular incision in the abdominal flap, as proposed by Massiha et al.,7 an inverted U-shaped incision in the flap, as proposed by Malic et al.,8 and Y-shaped de-epithelialized skin flaps, as suggested by Castilho et al.9
Several techniques have been described for specific cases of umbilical reconstruction, such as congenital absence or loss due to trauma.13-17 According to Illouz,18 umbilical reconstruction should be a part of all abdominoplasties, as the umbilicus, although aesthetically important, has no other function and can be replaced.
The purpose of this study was to present a new, simple, and fast technique for umbilical reconstruction with consistent, natural-looking results, no apparent scars, and which can be routinely performed as a part of abdominoplasty, replacing the technique of umbilical transposition.
METHODS
Umbilical reconstruction using an X-shaped incision was performed in 401 consecutive patients who underwent abdominoplasty.
The age of the patients ranged from 23 to 67 years (392 women and 9 men).
The surgeries were performed between July 2003 and December 2011 and the postoperative follow-up period ranged from 5 to 36 months.
Surgical Technique
A suprapubic incision with a superior concavity was made between the anterior and superior iliac crests. The dermoadipose flap was lifted to expose the aponeurosis and the detached flap was stretched up to the xiphoid appendix.
The umbilicus pedicle was dissected and separated from its base at the aponeurosis. If the abdominal cavity had been inadvertently opened, its closure was performed with a simple suture using 3-0 nylon. Following hemostasis, the rectus diastasis was corrected with 2-0 non-absorbable prolene sutures. As a result of this surgical procedure, the umbilical stump was invaginated and methylene blue was used to mark its position in the abdominal wall.
Traction was applied to the upper portion of the flap as it was progressively fixed to the aponeurosis, beginning at the xiphoid appendix area and extending up to the umbilicus. This was performed with pairs of 2-0 absorbable sutures that were placed 4-cm apart following the midline of the abdominal wall. Excess tissue was then resected (Figure 1).

Figure 1 - Before resection of the abdominal flap
Figure 1 shows the depressions in the upper portion of the flap indicating the locations where it was sutured to the aponeurosis (Baroudi).
The border of the remaining abdominal flap was then temporarily sutured to the border of the pubic incision to define the position with the neo-umbilicus using an "umbilicus marker," which projects the original position of the umbilicus in the surface of the tractioned flap (Figure 2).

Figure 2 - Use of an umbilicus marker to define its original position
At this location, an X-shaped mark was made, with each of its 4 segments measuring 4 mm in length (Figure 3).
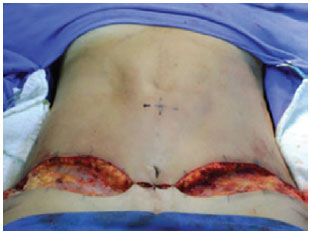
Figure 3 - The flap is temporarily fixed to the pubic region and location of the "X" in the abdominal flap
An X-shaped incision was performed, creating 4 small V-shaped flaps (Figure 4).
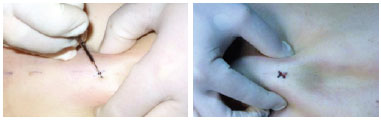
Figure 4 - An X-shaped incision forming 4 small V-shaped flaps.
Subsequently, a scissor was used to perform conical resection of the adipose tissue located under the X-shaped incision, creating a depression in this area (Figure 5A).
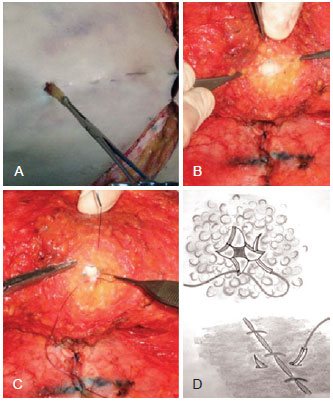
Figure 5 - A, Removal of a small portion of the cone-shaped adipose tissue to create a central depression. B, Small V-shaped flaps as observed during eversion. C, Photograph of the first suture. D, Diagram showing placement of the first suture in the aponeurosis and V-flaps. The suture is passed through the upper V-shaped flap and then through the left flap.
The temporary suture used to fix the flap was removed and the abdominal flap was everted for hemostasis (Figure 5B).
The neo-umbilicus was fixed to the aponeurosis in the location previously marked using two 2-0 absorbable monofilament sutures. The first suture was passed through the aponeurosis, the upper V-shaped flap, and the left V-shaped flap. The second suture, placed immediately under the first, was passed through the aponeurosis, the right V-shaped flap, and the lower V-shaped flap (Figure 5C and 5D).
Figure 6A shows the immediate postoperative results. The X-shaped incision was hidden within the new umbilicus. Once the neo-umbilicus was created, the lower portion of the abdominal flap was fixed to the aponeurosis with several sutures in the same manner as the upper portion. The final closure consisted of 3 layers of 4-0 absorbable sutures.
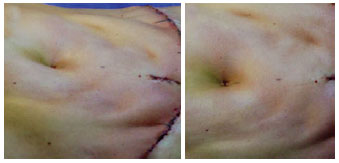
Figure 6 - Postoperative appearance
The neo-umbilicus was dressed with gauze and silver sulfadiazine cream. Dressings were changed daily for 12 days while keeping the area protected without compression.
Fifty patients were randomly selected to participate in a survey to examine their level of satisfaction with the procedure and its results.
A 5-point Likert scale was used to assess the level of patient satisfaction, ranging from 1 to 5, where: 1 = bad; 2 = reasonable; 3 = good; 4 = very good; and 5 = excellent. The results were also assessed by the surgeon.
RESULTS
Of the 43 (86%) patients who answered the survey, 90.3% rated their neo-umbilicus as good or excellent (excellent, 67.4%; very good, 23.2%; good, 9.3%).
Figure 7 presents the results of the surgeon's aesthetic evaluation of the umbilical reconstruction, which was considered good or excellent in 95% of cases.
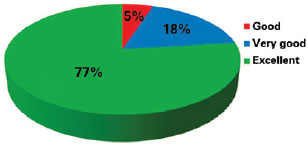
Figure 7 - Surgeon's evaluation of the surgical outcome of umbilical reconstruction
Figure 8 shows examples of the results obtained after umbilical reconstruction using an X-shaped incision.

Figure 8 - A and C, preoperative appearance of a neoomphaloplasty using an X-shaped incision: frontal and oblique left views, respectively. B and D, postoperative appearance 6 months after surgery: frontal and oblique left views, respectively.
Thirty-nine (9.7%) patients experienced immediate complications, including infection (3.99%), seroma (2.74%), necrosis (1.5%), hematoma (0.99%), and wound dehiscence (0.5%). Patients with infections responded quickly to oral antibiotics. None of the patients required reintervention.
Based on the satisfactory results obtained after the use of X-shaped incisions in umbilicoplasty, it is possible to routinely discard the original umbilicus, which is usually deformed, widened, or darkened because of previous pregnancies, and create a neo-umbilicus with a younger appearance (Figures 8 to 12).

Figure 9 - A, preoperative appearance of a neoomphaloplasty using an X-shaped incision, frontal view. B, postoperative appearance 6 months after surgery.
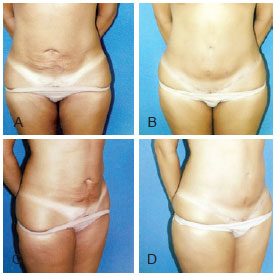
Figure 10 - A and C, preoperative appearance of a neoomphaloplasty using an X-shaped incision, frontal and oblique right views, respectively. B and D, postoperative appearance 8 months after surgery, frontal and oblique right views, respectively.
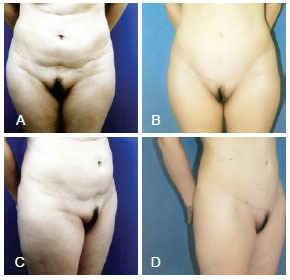
Figure 11 - A and C, preoperative appearance of a neoomphaloplasty using an X-shaped incision, frontal and oblique right views, respectively. B and D, postoperative appearance 1 year after surgery, frontal and oblique right views, respectively.
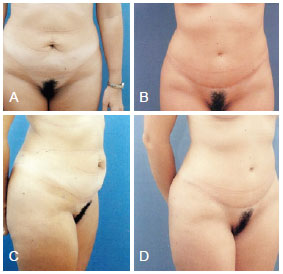
Figure 12 - A and C, preoperative appearance of a neoomphaloplasty using an X-shaped incision, frontal and oblique right views, respectively. B and D, postoperative appearance 7 months after surgery, frontal and oblique right views, respectively.
DISCUSSION
Umbilicus reconstruction is one of the most important steps of abdominoplasty because the umbilicus will be more visible than the lower abdominal scar.
Currently, the umbilical transposition technique is used more often than umbilical reconstruction. The objective of these 2 techniques is to avoid visible and hypertrophic scars, stenosis, and suture marks. Well-positioned umbilici with natural features such as adequate depth and small folding of the upper skin, can be achieved with umbilical reconstruction.19
Most of the techniques used for umbilical reconstruction were developed for cases in which transposition was either not indicated or not possible.
Kirianoff20 proposed the use of 3 skin flaps sutured to the aponeurosis during reconstruction, whereas Sabatier et al.17 used U-shaped flaps. In 1975, Baroudi4 described a procedure in which the borders of a small, linear incision were sutured to the aponeurosis. Franco and Franco13 reported the use of 3 skin flaps anchored to the aponeurosis, leaving a small central area opened, which would then heal by secondary intention. Franco et al.15 used 2 flaps and 2 grafts that were alternately fixed to the aponeurosis.
Marconi16 described a simple umbilical reconstruction technique that uses a degreased island skin flap and purse-string sutures. Pardo-Mateu and Chamorro-Hernandez21 also reported the use of purse-string sutures in an ellipsis separated into 3 flaps for umbilical reconstruction.
Other techniques have also been described; however, they frequently lead to the formation of large and highly visible scars, or are too complex and lengthy, thus increasing the duration of surgery and consequently the risk of complications.22-24
The described technique using an X-shaped incision was initially used only in cases in which the original umbilicus could not be preserved. However, its good results encouraged the use of this technique in all abdominoplasties, always discarding the original umbilici.
With the use of the described technique, reconstruction can be performed in < 10 min, and the internal sides of the 4 small flaps are fixed to the aponeurosis with absorbable sutures, thus avoiding external suture marks and the need for suture removal. In contrast, the technique of 3 flaps described by Franco and Franco13 relies on the use of external nylon sutures, which need to be removed subsequently.
The suture of the flaps to the aponeurosis results in umbilici showing adequate depth and a small skin fold on the upper pole. These are the 2 most important anatomic features of the first scar that is acquired after birth.
The cicatrization is fast, lasting approximately 15 days, and grafts are not required. The absence of circular scars and, therefore, of stenosis also contributes to the high level of satisfaction with the appearance of the neo-umbilicus.
The umbilical transposition technique often leaves apparent scars around the umbilicus, and discromy in the umbilical wall is frequently observed (Figure 13). Moreover, when necrosis or wound dehiscence occurs unaesthetic scars and stenosis tend to develop, which does not occur when umbilical reconstruction techniques such as those using the X-shaped incision or 3 flaps,13,20,21 are used.

Figure 13 - Unsatisfactory results, apparent scars, and discromy of the umbilical wall.
If necrosis or wound dehiscence occurs, the scar forms inside the umbilicus and not on its periphery. Its retraction could even contribute to the aesthetic result of a deeper umbilicus. The reduced size of the flaps represents an advantage of the proposed technique over other reconstruction techniques.
The technique using an X-shaped incision produces smaller flaps than those obtained with other techniques, such as the one using 3 flaps.13,20,21 This minimizes the risk of necrosis in the distal extremity of the flaps, and if necrosis does occur, it will result in fewer deformities. In this study, only 6 (1.5%) patients presented with necrosis and none of these required reintervention.
The small scars remain hidden within the new umbilicus, in its center, and are not noticeable. If the umbilicus is shallower, the scar will simulate natural pleats. A small vertical scar in the hypogastrium resulting from the closing of the original umbilical orifice, in a much lower location than the new umbilicus, may be necessary when traction of the abdominal flap is insufficient to allow resection of this area.
It is important to note that this vertical scar is not related to the X-shaped incision. Moreover, it is required in any abdominoplasty, regardless of the technique used for reconstruction or umbilical transposition. However, the technique described herein does not lead to any visible periumbilical scars, which contributes to greater patient acceptance of the vertical scar, if it does form.
As proposed by Baroudi and Ferreira,14 fixation of the entire abdominal flap to the aponeurosis using as many sutures as needed, reduces tension in the area surrounding the umbilicus and improves the quality of the final scar. It also allows better control of the shape of the neo-umbilicus, varying the position of the surrounding fixation sutures.
If the traction applied to the flap fixation points below the umbilicus is increased, it will be more elongated. Several typical examples of abdominoplasty results with umbilical reconstruction in the form of an "X" are shown in Figure 4.
Although it is difficult to define objective criteria for the postoperative analysis as it relates to the umbilical shape and dimensions, the subjective evaluation of the aesthetic results by the surgeon and patients, along with the high level of satisfaction with the appearance of the neo-umbilicus, are sufficient to suggest the routine use of the present technique using an X-shaped incision in abdominoplasties.
CONCLUSIONS
Neoomphaloplasty using an X-shaped incision is a simple, fast procedure that leads to the formation of pleasant- and natural-looking umbilical scars, without increasing the duration of surgery or leaving visible scars.
The rate of complications seems to be lower than that of umbilical transposition techniques. The neo-umbilicus often cannot be distinguished from a natural one. The scars are also much less noticeable than those formed from transposition techniques.
The neo-umbilicus often looks better than the original umbilicus, which is often deformed owing to obesity or previous gestations.
The procedure has long-lasting aesthetic results that will not disappear over time. Moreover, its routine use offers uniform and predictable results, with a low rate of complications and a high level of patient satisfaction.
REFERENCES
1. Regnault P. The history of abdominal dermolipectomy. Aesthetic Plast Surg. 1978;2(1):113-23.
2. Hakme F. Abdominoplasty: peri- and supra-umbilical lipectomy. Aesthetic Plast Surg. 1983;7(4):213-20.
3. Vernon S. Umbilical transplantation upward and abdominal contouring in lipectomy. Am J Surg. 1957;94(3):490-2.
4. Baroudi R. Umbilicoplasty. Clin Plast Surg. 1975;2(3):431-48.
5. Avelar J. Abdominoplasty: systematization of a technique without external umbilical scar. Aesthetic Plast Surg. 1978;2(1):141-51.
6. Juri J, Juri C, Raiden G. Reconstruction of the umbilicus in abdominoplasty. Plast Reconstr Surg. 1979;63(4):580-2.
7. Massiha H, Montegut W, Phillips R. A method of reconstructing a natural-looking umbilicus in abdominoplasty. Ann Plast Surg. 1997;38(3):228-31.
8. Malic CC, Spyrou GE, Hough M, Fourie L. Patient satisfaction with two different methods of umbilicoplasty. Plast Reconstr Surg. 2007;119(1):357-61.
9. Castillo PF, Sepúlveda CA, Prado AC, Troncoso AL, Villamán JJ. Umbilical reinsertion in abdominoplasty: technique using deepithelialized skin flaps. Aesthetic Plast Surg. 2007;31(5):519-20.
10. Akbaş H, Guneren E, Eroğlu L, Uysal OA. Natural-looking umbilicus as an important part of abdominoplasty. Aesthetic Plast Surg. 2003;27(2):139-42.
11. Lee MJ, Mustoe TA. Simplified technique for creating a youthful umbilicus in abdominoplasty. Plast Reconstr Surg. 2002;109(6):2136-40.
12. Ribeiro L, Muzy S, Accorsi A. Omphaloplasty. Ann Plast Surg. 1991;27(5):457-75.
13. Franco T, Franco D. Neoomphaloplasty: an old and new technique. Aesthetic Plast Surg. 1999;23(2):151-4.
14. Baroudi R, Ferreira CA. Seroma: how to avoid it and how to treat it. Aesthet Surg J. 1998;18(6):439-41.
15. Franco T, Boghossian LC, Silva ALB. Neo-onfaloplastia. Rev Bras Cir. 1985;75(4):257-60.
16. Marconi F. Reconstruction of the umbilicus: a simple technique. Plast Reconstr Surg. 1995;95(6):1115-7.
17. Sabatier PH, Barraya L, Picaud AJ. A peculiar technic for the umbilicus reconstruction. Ann Chir Plast. 1978;23(4):245-8.
18. Illouz YG. A new safe and aesthetic approach to suction abdominoplasty. Aesthetic Plast Surg. 1992;16(3):237-45.
19. Craig SB, Faller MS, Puckett CL. In search of the ideal female umbilicus. Plast Reconstr Surg. 2000;105(1):389-92.
20. Kirianoff TG. Making a new umbilicus when none exists. Case report. Plast Reconstr Surg. 1978;61(4):603-4.
21. Pardo-Mateu L, Chamorro-Hernandez JJ. Neoumbilicoplasty through a purse-string suture of three defatted flaps. Aesthetic Plast Surg. 1997;21(5):349-51.
22. Matsuo K, Kondoh S, Hirose T. A simple technique for reconstruction of the umbilicus, using a conchal cartilage composite graft. Plast Reconstr Surg. 1990;86(1):149-51.
23. Schoeller T, Wechselberger G, Otto A, Rainer C, Schwabegger A, Lille S, et al. New technique for scarless umbilical reinsertion in abdominoplasty procedures. Plast Reconstr Surg. 1998;102(5):1720-3.
24. Uraloğlu M, Tekin F, Orbay H, Unlu RE, Sensöz O. Simultaneous abdominoplasty and umbilical reconstruction using a modified C-V flap technique. Plast Reconstr Surg. 2006;117(7):2525-6.
Plastic Surgeon, full member of the Brazilian Society of Plastic Surgery, Belo Horizonte, MG, Brazil
Correspondence to:
Ticiano César Teixeira Cló
Rua República Argentina, 507 - Sion
Belo Horizonte, MG, Brazil - CEP 30315-490
E-mail: ticianoclo@terra.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: June 3, 2012
Article accepted: October 8, 2012
Work performed at the private clinic of the author, Belo Horizonte, MG, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket