



Ideas and Innovation - Year 2013 - Volume 28 -
Aesthetic otoplasty using a crochet needle
Otoplastia estética com emprego de agulha de crochê
ABSTRACT
In aesthetic otoplasty, it is widely known that only techniques that disassemble the resilient cartilaginous architecture in cases of protruding ears coupled with anchoring sutures can achieve good and stable results. All surgical otoplasty procedures aim to achieve a new, shapely, and aesthetic antihelix fold that shapes and beautifies the outer ear. In this article, we describe our 10-year experience with the use of a new instrument for auricular cartilage striation - the traditional crochet needle. Moreover, we describe the manner in which the new instrument can be prepared in order to have a lower bevel cutting edge as well as the technical management of this instrument in small buttonholes in the auricular helix. After molding the antihelix complex, the new form is fixed with absorbable and non-absorbable sutures. With this technique, there is a low complication rate due to narrow cutaneous detachment tunnels in the anterior surface of the ear. In the article, we also describe the successful clinical use of the new instrument.
Keywords: External ear/surgery. Needles. Plastic surgery/methods.
RESUMO
Um consenso atual em otoplastia estética apregoa que somente as técnicas que desmontem a resiliente arquitetura cartilaginosa das orelhas protrusas, aliadas à fixação da nova forma com suturas, podem alcançar resultados bons e estáveis. O alvo cirúrgico de toda otoplastia é a nova dobra da antélice torneada e estética: uma roliça dobra afunilada que dá forma e beleza à orelha externa. Neste artigo é descrita a experiência de 10 anos com o uso de um novo instrumental no estriamento da cartilagem auricular: as tradicionais agulhas de crochê. Além disso, são demonstrados o modo de aparelhar o novo dispositivo, para ter uma borda inferior em bisel cortante, e a técnica de manejo desse dispositivo por pequenas botoeiras sob a hélice auricular. Após a moldagem do complexo antelical, é assegurada a nova forma com suturas, absorvível e não-absorvível. Com essa técnica, é observado baixo índice de complicações, em decorrência de estreitos túneis de descolamento cutâneo da face anterior do pavilhão auricular. No artigo, é também apresentado um caso clínico bem-sucedido com o uso do novo instrumental.
Palavras-chave: Orelha externa/cirurgia. Agulhas. Cirurgia plástica/métodos.
In aesthetic otoplasty, a new antihelix fold can be constructed in 4 ways: via cartilage plication through a cartilaginous incision/excision, outer perichondrial scarification, and a combination of both.
The technique that yields a definitive natural aspect of the ear ensures appropriate external perichondrium striation in the antihelix axis and achieves a new form of the antihelix complex via special sutures at the base as well as in the body and the superior antihelix crus1.
Many techniques employ exclusive rasps, toothed forceps, hypodermic needles, or sharpened Kirschner wires to excoriate this thin cartilage through subcutaneous tunnels2-6. Other techniques, after lifting of the outer perichondrial skin, employ scalpels or scalpel blades, diamond burs, or even thin rasps for perichondrial scoring7-10. The instruments used to create the tunnels should be especially delicate. All of these techniques are based on the Gibson & Davis11 and Stenstrom7 principle, which consists of external perichondrial rupture by scorers and enables higher tension at the opposite perichondrial interface, while arching the cartilage on that side.
AESTHETIC OTOPLASTY USING A CROCHET NEEDLE
Ten years earlier, based on the experience gained with the Stenstrom7 method and their abraders, our team introduced a versatile instrument that is widely used in vascular surgery - the crochet needle.
To obtain the desired effect, the delicate blunt hook end of this needle was modified to resemble a cutting bevel. The beveled part was obtained by polishing the bottom edge with the aid of a delicate emery grinder, used in rhinoplasty in the alar cartilages, leaving the blunt tip to protect the skin of the anterior surface.
Modified number 00, 01, and 02 steel crochet needles have a cutting edge of approximately 2 mm and are able to pass through the narrow tunnels (Figure 1).
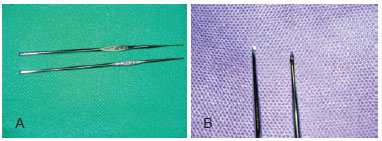
Figure 1 - In A, standard crochet needles. In B, a normal crochet needle and the modified active portion.
Preoperative drawings were made on the anterior ear to create an enlarged superior crus, followed by a mean furcula right to the acute antihelix body, as part of the corrective plan of the antihelix complex. A vasoconstrictor anesthetic was then injected for skin hydrodissection on the anterior and posterior surface of the ear, which was initiated with the Moldenhauer hook detacher (used in tonsillectomies) and completed with the Stenstrom abrader (Figure 2). Three parallel tunnels are created via a 4 mm micro-incision on the anterior fold of the helix or by excision of a spindle italic "S" of the retroauricular skin. These tunnels are positioned on top of the body, the upper furcula and the superior crus of the antihelix, and at the lower and upper limits. With the finger of the opposite hand placed on the back of the ear as a sensitive base, the crochet needle traverses the path of tunnels to the highest point with the bevel maintained parallel to the skin. To score, three to seven insertions of the needle are performed beneath the thin perichondrium, the depth of which is controlled by the other hand on an anteriorly and posteriorly "dry" ear (Figure 3). The presence of perichondrial fibers can halt the insertion of the crochet needle, which is reversed by retreating and turning.

Figure 2 - Creation of tunnels in the anterior surface of the ear using thin retractors.

Figure 3 - Passage of the crochet needle through the narrow subcutaneous tunnels of the external ear surface.
Four soft passes of the crochet needle in strategic points are typically sufficient to undermine the resilient cartilage, except in patients > 10 years of age or adults, where additional passes may be required. Since there are no extensive detachments but rather threaded tunnels as in liposuction, the swelling is reduced, and the likelihood of hematoma or postoperative skin necrosis is very low. The antihelix fold does is not detached or striated, but is reconstructed with non-absorbable sutures. In the body and superior antihelix crus, a special stitch is made using a PDS II slow absorption suture. The skin excision at the antihelix groove is closed using 4-0 catgut thread in a continuous subcuticular suture.
The dressing consists of a thin layer of gauze with antibiotic ointment on the retroauricular suture line and wet cottony gauze monocle on the front surface that is covered with dry gauze for fixation with sterile strips in the malar and mastoid regions. Both sides are wrapped with crepe elastic bandage in the form of a turban for patient comfort. The dressing is maintained for 48-72 hours; when it is removed, a single longitudinal strip remains on the internal wound. A frontal night band is applied on the superior helix for 1 month. Figure 4 illustrates the case of a patient on whom the new instrument was used to perform the otoplasty, and good aesthetic results were obtained.
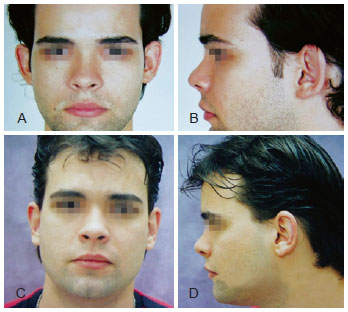
Figure 4 - Case report. In A and B, preoperative aspect, respectively, frontal and left profile. In C and D, 1-year postoperative aspect, respectively, frontal and left profile.
ACKNOWLEDGEMENTS
To Mr. Valerio Parizotto, Sulivan Ruwer, and Richard Fiorino (in memoriam).
REFERENCES
1. Furnas DW. Otoplasty for prominent ears. Clin Plast Surg. 2002;29(2):273-88.
2. Kaye BL. A simplified method for correcting the prominent ear. Plast Reconstr Surg. 1967;40(1):44-8.
3. Vecchione TR. Needle scoring of the anterior surface of the cartilage in otoplasty. Plast Reconstr Surg. 1979;64(4):568.
4. Mahler D. The correction of the prominent ear. Aesthetic Plast Surg. 1986;10(1):29-33.
5. Thomas SS, Fatah F. Closed anterior scoring for prominent-ear correction revisited. Br J Plast Surg. 2001;54(7):581-7.
6. Bulstrode NW, Huang S, Martin DL. Otoplasty by percutaneous anterior scoring. Another twist to the story: a long-term study of 114 patients. Br J Plast Surg. 2003;56(2):145-9.
7. Stenstroem SJ. A "natural" technique for correction of congenitally prominent ears. Plast Reconstr Surg. 1963;32:509-18.
8. Chongchet V. A method of antihelix reconstruction. Br J Plast Surg. 1963;16:268-72.
9. Neumer O. A simple method for the correction of prominent ears. Plast Reconstr Surg. 1971;47(2):111-6.
10. Nordzell B. Open otoplasty. Plast Reconstr Surg. 2000;106(7):1466-72.
11. Gibson T, Davis W. The distortion of autogenous cartilage grafts: its cause and prevention. Br J Plast Surg. 1958;10:257-74.
1. Plastic surgeon, full memberof the Sociedade Brasileira de Cirurgia Plástica (Brazilian Society of Plastic Surgery), Director, Interclínicas Interplástica, plastic surgeon, Santa Casa de Campo Grande, Campo Grande, MS, Brazil
2. Resident physician, Hospital Universitário da Universidade Federal de Mato Grosso do Sul (University Hospital of the Federal University of Mato Grosso do Sul), assistant surgeon, Interclínicas Interplástica, Campo Grande, MS, Brazil
Correspondence to:
Miguel Marques Oliveira
Av. Afonso Pena, 3504 - Gr. 126 - Jardim dos Estados
Campo Grande, MS, Brazil - CEP 79002-075
E-mail: corpusclinica1@gmail.com
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: July 17, 2012
Article accepted: July 23, 2012
This study was performed at Interclínica-Interplástica, Campo Grande, MS, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket