



Original Article - Year 2013 - Volume 28 -
Profile ofplastic surgeons in the state of Paraná, Brazil
Perfil do cirurgião plástico paranaense
ABSTRACT
INTRODUCTION: In the present study, we aimed to outline the overall practice profile of plastic surgeons in the state of Paraná. It represents an initial project that aimed not to provide generalizations but to understand how plastic surgeons think and their professional aspirations, goals, and performance.
METHODS: A survey was conducted using a questionnaire consisting of 37 multiple-choice questions, mostly focusing on the current job market for plastic surgeons. The link to the online questionnaire was e-mailed to 263 members of the Brazilian Society of Plastic Surgery-Regional Paraná (SBCP-PR), which was also accessible via the SBCP-PR website, through a banner on its home page. The overall time to complete the questionnaire ranged from 3 to 5 minutes.
RESULTS: The response rate was 40.5%. Most interviewees operated only in one city, and more than half provided services only through health-care insurance plans and private practice. Half of the participants considered the market as extremely competitive and searched for several alternatives for self-maintenance, including increasing installment payment terms, lowering prices, and working at other locations. A significant proportion of the respondents believed that they lost more than 30 patients owing to pricing in the previous year and performed 10-20 surgeries per month on average. Most of the surgeons did not operate with an auxiliary plastic surgeon because this would increase their operational cost or because technologists could perform this function. Most participants believe that the number of trained residents in the state of Paraná is excessive.
CONCLUSIONS: In Paraná, plastic surgeons are concerned about the job market and therefore search for alternatives to remain competitive.
Keywords: Job market. Surgery, plastic. Professional practice. Marketing of Health Services.
RESUMO
INTRODUÇÃO: Esta pesquisa tem por objetivo traçar o perfil do cirurgião plástico do estado do Paraná. É um projeto inicial que não tem a pretensão de indicar respostas, mas sim de entender o que pensa, quais os anseios e objetivos na profissão e como atua o profissional dessa especialidade.
MÉTODO: Foi idealizada uma pesquisa com 37 perguntas de múltipla escolha, em sua maioria com foco no mercado de trabalho. Ela foi enviada por e-mail aos 263 membros da Sociedade Brasileira de Cirurgia Plástica - Regional Paraná (SBCP-PR), sob forma de um link que dava acesso ao questionário. O link também estava disponível no website da SBCP-PR, com um banner em sua página inicial. O tempo médio para preenchimento do questionário variou de 3 minutos a 5 minutos.
RESULTADOS: O índice de resposta foi de 40,5%. A maioria dos entrevistados atua apenas em uma cidade, e mais da metade atende apenas convênios e particulares. Metade dos participantes considera o mercado extremamente competitivo e procura várias alternativas para se manter, entre elas: aumentar parcelamento, baixar preços e atuar em outros locais. Uma parcela significativa acredita ter perdido mais de 30 pacientes por preço no último ano e faz, em média, 10 a 20 cirurgias mensais. A maioria dos participantes não opera com auxiliar cirurgião plástico, pois consideram que aumenta o custo ou que instrumentadoras podem fazer a mesma função. A maioria dos participantes acredita que o número de residentes formados no estado é excessivo.
CONCLUSÕES: O cirurgião plástico no Paraná está muito preocupado com o mercado de trabalho e procura alternativas para se manter competitivo.
Palavras-chave: Mercado de trabalho. Cirurgia plástica. Prática profissional. Marketing de Serviços de Saúde.
The use of plastic surgery has recently become widespread and has been significantly popularized globally, especially in Brazil1. What was once considered a luxury for a few people now represents a tangible dream for almost all social classes. Several factors have contributed to this scenario, such as global economic growth (indirectly boosting the Brazilian economy), increasing number of professionals in this line of work, ethical (or unethical) improvement of payment conditions (installment, consortium, and intermediating), and progressive decrease in values applied due to peer competition.
It is common to witness new surgeons mention complaints regarding the job market to experienced colleagues. Their opinions are almost unanimous: the market is becoming more challenging, the fees are lower, and patients are increasingly demanding. What should be done to improve this situation? This question requires a complicated answer considering that the factors that may affect this market are apparently multiple.
The present research was conducted with the purpose of outlining the overall practice profile of plastic surgeons in the state of Paraná. It represents an initial, almost embryonic, project. We did not intend to provide generalizations, which would require many other studies for validation. Instead, we aimed to simply understand how these professionals think and their professional aspirations, goals, and performance.
Nevertheless, the results of this study may provide insight on some observed data and possibilities for a more encouraging perspective regarding the future of our profession.
METHODS
A survey was designed using a questionnaire consisting of 37 multiple-choice questions, mostly focusing on the job market for plastic surgeons in the state of Paraná. The survey was developed based on the study of Krieger and Shaw2. Some modifications were made for the Brazilian scenario, especially in the state of Paraná. Thereafter, a specialized company created an online research system using the Google Docs platform.
The anonymity of the participants was ensured throughout the survey. The online link to the survey questionnaire was sent by e-mail to all the 263 members of the Brazilian Society of Plastic Surgery (SBCP) who work in Paraná and had updated cadastral records (4 of 267 had no e-mail information). The link was also available on the SBCP-Regional Paraná (SBCP-PR) website, through a banner on its home page.
The overall time to complete the questionnaire ranged from 3 to 5 minutes. Three reminders to respond to the survey were sent via e-mail, with an interval of 15 days. After a period of approximately 45 days, 106 responses were obtained. A spreadsheet containing all the responses was exported to the Excel platform, and statistical evaluation of crossed data was performed. To facilitate better understanding, graphs were constructed based on the most relevant data. A professional statistician performed the statistical evaluation of the data. The results were presented as mean, median, range, and standard deviations (quantitative variables) or as frequencies and percentages (qualitative variables).
RESULTS
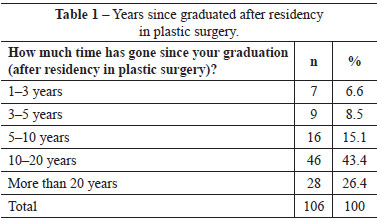
The response rate to the survey was 40.5% (106/263 respondents). Among the 106 respondents, 32.1% and 67.9% represented titular and specialist members, respectively. Table 1 shows the time of the participants' completion of their professional education.
Most participants (71.7%) practiced their profession only in one city, but responses to the survey came from all regions of the state (Table 2). Most of the plastic surgeons in this study owned an office (65.1%) and offered private practice services (48.1%). A little more than half of the volunteers only assist patients through health-care insurance plans and private service; however, a significant number of surgeons reported working within the Public Health System (SUS; 34.9%). In particular, a small percentage (18%) of the interviewees indicated that they performed cosmetic surgeries through health-care insurance plans (Table 3).


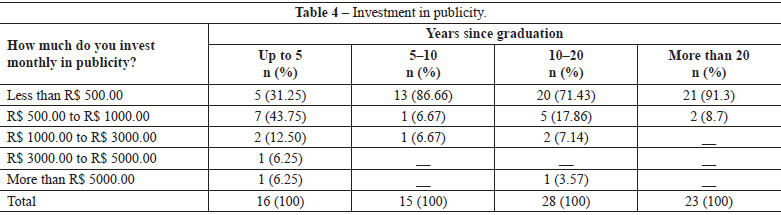
A significant number of the volunteers advertised their work (40.6%); of these, 36.8% reported the use of websites, 8.5% reported the use of magazines, and 8.5% reported the use of magazines and websites. Only 4.7% used other methods of publicity, such as advertising in television, press office, and radio, besides magazines and websites. Most (72%) of the surgeons who advertised their work claimed to have invested less than R$500.00 per month for this purpose (Table 4).
The monthly number of new consultations was described, as follows: of the participants, 35.8% had up to 20 new consultations, 31.3% had 30-50 new consultations, 18.9% had 20-30 new consultations, and 14.2% had more than 50 new consultations. Regarding payment methods, 56.6% of the surgeons reported accepting credit cards and 98.1% reported accepting installment payments ranging from 2 (2.9%) to 24 installments (1%). A smaller percentage of participants utilized companies to perform installment transactions on their behalf, including Saúde Service (15.4%), Online Doctor (1.1%), and Dr. Crédito (3.3%). Only one of the surgeons indicated performing free consultations, and 84.8% of the interviewees charged a consultation fee ranging from R$ 100.00 to R$ 200.00.
When asked about the number of clients that the participants believed they had lost to competitors in the last year owing to pricing, 41.9% responded that more than 30 clients were lost in this manner, whereas 22.9%, 21%, and 14.3% responded that 10-20, up to 10, and 20-30 clients were lost in this manner, respectively. In addition, 36.8% indicated that they perform 10-20 surgeries per month, 29.2% performed 20-30 surgeries, 23.6% performed up to 10 surgeries, and only 10.4% performed more than 30 surgeries per month. It is noteworthy that the types of procedures performed were not specified. When asked if they operate with the help of an auxiliary plastic surgeon, 52.8% of the interviewees denied the practice (Table 5); the justifications for this are presented in Figure 1. Of the procedures the surgeons performed in their daily practice, the frequency rates of plastic surgery procedures were as follows: 81-100% in 51.4%, 61-80% in 34.3%, 41-60% in 5.7%, 21-40% in 6.7%, and 0-20% in 1.9% participants.
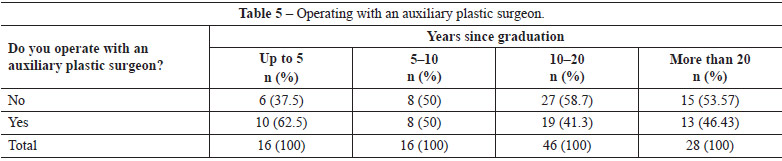
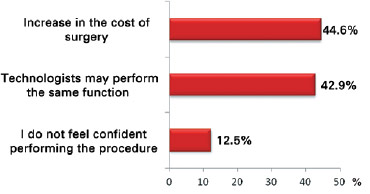
Figure 1 -Justification for not operating with an auxiliary plastic surgeon.
Regarding the plastic surgery market in Paraná, 49% of the surgeons reported it to be extremely competitive and only 1.9% reported it to be not so competitive (Table 6). We observed a balance between the interviewees who considered their patients to be moderately sensitive (51.5%) and those who considered their patients to be very sensitive (47.6%) to price changes. Only one surgeon classified patients as insensitive to price changes. The social classes of the standard patients are depicted in Figure 2. The initiatives adopted by the participants to maintain the number of plastic surgery procedures that they perform are presented in Table 7.
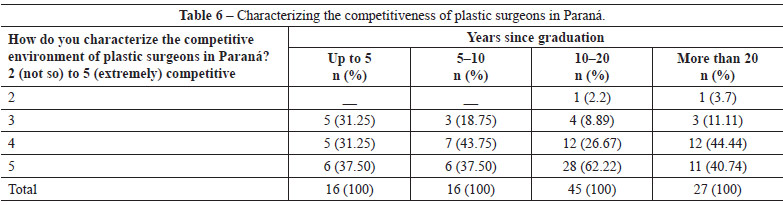
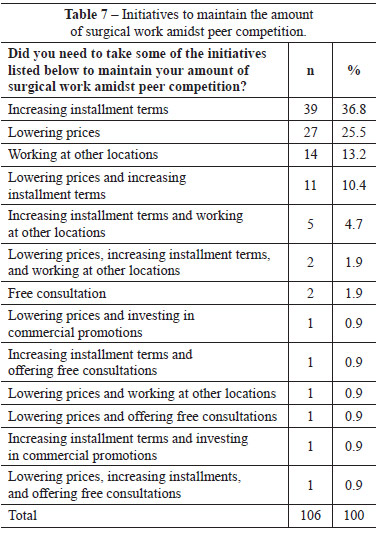
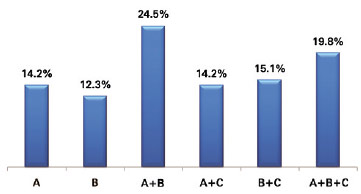
Figure 2 -Social classes to which the standard patients belonged. Observation: only classes A-C were included in the question.
The factors that significantly affect job market trends, as reported by the surgeons, are as follows: excessive number of active plastic surgeons, excessive number of recently graduated plastic surgeons entering the market, invasion of other specialties, and misdistribution of surgeons across cities. Of the respondents, 21.9% indicated all of the factors; 14.3% indicated all factors, except for misdistribution of surgeons; 13.3% indicated only excessive number of active plastic surgeons and invasion of other specialties; and 7.6% indicated only invasion of other specialties. When asked about the number of residents graduating in plastic surgery in Paraná, 62.4% of the participants considered it to be excessive; 36.6% considered it to be adequate; and only 1% considered it to be small.
In respect to the table of prices suggested by the SBCP-PR, most (62.3%) of the interviewees claimed to apply the prices, whereas 21.7% and 16% indicated that they considered the values to be too high and too low, respectively.
Furthermore, 82.1% of the surgeons reported performing nonsurgical procedures, the most cited being the use of botulinum toxin (78.3%), hyaluronic acid fillers (45.28%), chemical peeling (13.2%), and fractionated CO2 laser (13.2%). Other procedures were also performed (such as intense pulsed light treatment, radiofrequency, laser hair removal, and bioplasty), although at a much lower frequency (1-3%).
The total net values (surgeon's fee, staff salary, prosthesis cost, and clinic/hospital operational cost) and net values of the professional fees for major surgeries implemented by the interviewees are presented in Tables 8 and 9, respectively. The net values were stratified according to graduation time after residency in plastic surgery (Figures 3 to 6). Figure 7 presents the goals of the participants in terms of medical fees and number of surgeries performed.


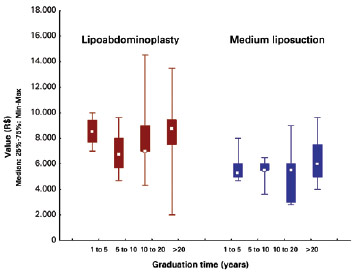
Figure 3 - Total values in R$ charged for lipoabdominoplasty and medium liposuction according to years since graduation after residency in plastic surgery. The total values include the surgeon's fee, staff salary, prosthesis cost, and clinic operational expense (anesthesiologist and materials).
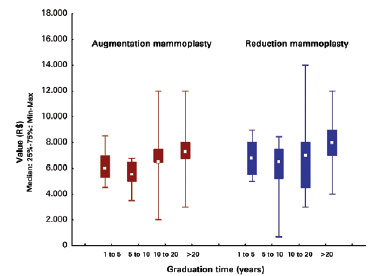
Figure 4 - Total values in R$ charged for augmentation mammoplasty and reduction mammoplasty according to years since graduation after residency in plastic surgery. The total values include the surgeon's fee, staff salary, prosthesis cost, and clinic operational cost (anesthesiologist and materials).
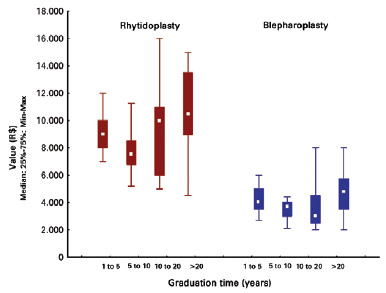
Figure 5 - Total values in R$ charged for rhytidoplasty and blepharoplasty according to years since graduation after residency in plastic surgery. The total values include the surgeon's fee, staff salary, prosthesis cost, and clinic operational cost (anesthesiologist and materials).
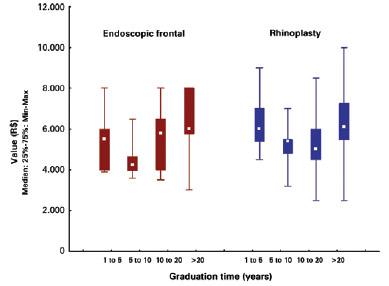
Figure 6 - Total values charged for endoscopic frontal and rhinoplasty according to years since graduation after residency in plastic surgery. The total values include the surgeon's fee, staff salary, prosthesis cost, and clinic operational cost (anesthesiologist and materials).
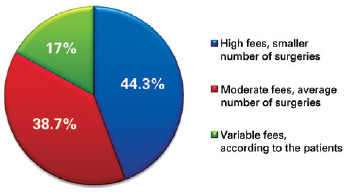
Figure 7 - Aim of the participants in terms of medical fees and number of surgeries performed.
DISCUSSION
For more than a decade, several authors have studied the relationship among plastic surgery, economics, and the job market3-8. However, this type of study is not common in Brazil. In 2009, SBCP conducted an extensive research survey using a sample of slightly more than 10% of its members at that time, obtaining 366 responses from a total of 3533 members. This study assessed the general situation of plastic surgery and plastic surgeon performance in the country, in addition to patient profiles and the major surgeries performed. However, the focus was not specifically on the job market, and the sample population from the state of Paraná was insufficient for statistical evaluation9. The present study may serve as a basis for other more detailed studies that aim to demonstrate the relationship between the number of surgeons and the job market trend in each Brazilian city or state.
The present online survey (via the link to the SBCP-PR website) achieved a response rate higher than the average (40.5%). Previous studies obtained a mean response rate of approximately 26%, and some factors may contribute to an increase in this value10,11, including prenotification and e-mailing from a trusted source or link to a reliable website. During a dinner held at the end of the year 2011, members of the SBCP-PR were informed that our research would be launched in early 2012; in addition, the e-mail from the SBCP-PR and the link to the website (www.sbcp-pr.org.br) that was made available through e-mail might have helped to increase the response rate to this survey.
Specialist members who had completed their residency 10-20 years previously represented most of our sample population (Table 1). This demonstrates that the most interested and collaborative surgeons were experienced members, who find themselves at a period of increased professional peer competition, as also shown in Table 6. Although more than 70% of the surgeons worked in only one city, the fact that approximately 30% worked in more than one city indicates the need to search for new markets; that is, the surgeons perceived increasing competition. Similarly, the percentage of surgeons (34.9%) that operated within the SUS was significant, as well as the percentage of those who performed cosmetic surgery through health insurance plans (17%). These values may be explained by the need to increase gains, as the values applied for the largest income source has plateaued over the recent years, with cosmetic surgery accounting for 81-100% of the operations of 51.4% of the surveyed surgeons.
In 2004, Krieger and Lee12 published an interesting paper on the changing performance of the plastic surgeon, from predominantly performing surgical repairs to cosmetic surgeries owing to the plateauing of the trend in the fees paid by health insurance plans. The authors pointed out that despite the increase in demand (number of surgeries per year) and the number of service providers (plastic surgeons), the amount of work increased by approximately 41% while the mean annual gain and cost per surgery remained stable.
It is interesting that a significant proportion of surgeons did not invest in any kind of publicity and that the most used publicity tool is the website, followed by magazines and other media (television, radio, and press office). Most of the participants who reported not investing in publicity had graduated more than 10 years earlier. The participants who reported spending on marketing were those who graduated within 5 years, spending more than R$5000.00 per month (Table 4). This demonstrates that the surgeons who were new in the market were more competitive and aggressive in this aspect. Rohrich13 claimed that career evolution in plastic surgery should be considered as the evolution of a surgeon's life. This evolution looks more like a marathon than a sprint. Surgeons must provide the correct rhythm to their professional growth. However, this does not appear to be the view of the newer colleagues, according to our data. In the past few years, it is difficult to imagine a surgeon who incurs high monthly marketing expenses. However, the current trends appear markedly different to those observed earlier.
Regarding market diversification and payment facilitation schemes, 98.1% of the surgeons received payment in installments and more than 50% accepted credit cards despite the high overhead costs. This demonstrates the need for the surgeon to remain competitive. In addition, the utilization of companies that serve as mediators in installment transactions (Saúde Service, Online Doctor, Dr. Crédito) and credit cards implies a decrease in the fear of competition, which is a chronic problem in many medical offices.
Only one surgeon indicated not charging for consultations. However, for those who took so long to complete their professional education, the values applied ranging from R$ 100.00 to R$200.00 might be too low. The costs associated with other professions involving lesser educational effort may be much higher than these values14.
Many surgeons performed between 10 and 20 surgeries per month, followed by those who conducted between 20 and 30 surgeries. Most of these surgeries were aesthetic, corroborating the findings of Krieger and Lee12. Generally, that number decreases to between 10 and 20 surgeries per month after 20 years of graduation, demonstrating that the surgeons did not maintain their initial number of surgeries at this stage, either by their own choice or by circumstances in their career.
The questions on the practice of operating with an auxiliary plastic surgeon and the reasons for not doing so demonstrate some important aspects about the job market in the state of Paraná, which probably reflects the situation in the rest of the country. More than half (52.8%) of the surveyed surgeons claimed to not operate with an auxiliary doctor. Among the reasons for this attitude is the high cost of surgery (44.6%); however, the fact that almost the same percentage of participants (42.9%) believed that technologists might exercise the same function is important. Only 12.5% of the interviewees indicated that they did not feel comfortable working with another plastic surgeon. The group concerned about the rising cost of operation due to the participation of an assistant surgeon obviously wanted to remain competitive in the market, reducing the total cost of the procedure, thus increasing the number of surgeries performed. The group that did not feel comfortable working with an assistant surgeon expressed difficulty in working in a team or delegating part of the procedure to an auxiliary plastic surgeon. Obviously, a well-trained and synchronized team only confers benefits to the patient and to the surgeon. The participation of an assistant surgeon results in less surgical and anesthesia time, along with a lower surgical risk. In addition, the procedure is less tiresome for the surgeon, and the surgeon can complete the surgery with the necessary zeal. The resolution of the Federal Council of Medicine 1490/98 deals with the composition of the surgical team, stating that the operation is the responsibility of the titular surgeon and that an assistant surgeon may be necessary if the titular is unable to continue the act. In the opinion of a counselor (1810/2007 CRM-PR), the issue can be addressed as follows: "It is good practice that the surgeon nominates an assistant surgeon to assist or replace him/her in his/her absence. A surgeon who gives up the presence of an assistant surgeon in elective surgery may be accused of unethical practice in case of failing to finish the procedure or if the procedure presents a complication leading to injury due to lack of assistance." Therefore, when surgeons choose to operate only with auxiliary technologists, they are exposed to an unnecessary risk. In addition, experienced surgeons may be of help to young surgeons in the start of their careers by employing them as assistants; however, they must take precaution against intermediating agents whose motive is the exploitation of the medical activity to increase their profits. Indirectly, surgeons put great value to their medical profession because of the long experience and intensive training required for them to obtain the title of expert, which is often devaluated by the statement, "Technologists may exercise the same function."
It is also important to emphasize that most of the younger surgeons operated with auxiliary plastic surgeons (Table 5) and that more than half of the surgeons who graduated 10-20 years and more than 20 years previously operated only with technologists. This might be explained by the following facts: (i) the young surgeon does not feel confident to perform a procedure alone, having the need to look for a partner to exchange opinions with, whereas (ii) most experienced surgeons feel confident to perform a procedure and thus dismiss any help from another plastic surgeon. Another fact to be considered is the lack of expert colleagues in smaller cities.
The professional competition increases on a daily basis, as evident in the fact that that almost half of the surveyed surgeons considered the job market to be extremely competitive and their patients to be very sensitive to price changes. The surgeons who had graduated 10-20 years previously felt the most intense competition (Table 6). Furthermore, the larger number of surgeons who perform cosmetic surgeries through health insurance plans fall under this postgraduation period (Table 3).
The present study confirms the popularity of plastic surgery, as 24.5% of the surgeons reported that their standard patients were from social classes A and B and 19.8% reported having patients from classes A-C (Figure 2).
The volunteers also described their main initiatives to maintain their number of performed surgeries. Increasing installment terms (36.8%), lowering prices (25.5%), and working at other locations (13.2%) were the most frequent initiatives, besides their combinations (Table 7). It is very common for patients to bargain, preferring the highest discounts for services among those offered by different surgeons. The surgeon is induced to accept this situation to maintain the number of surgeries that they perform in a certain period, which leads to the transformation of their services into commodities. The doctor-patient relationship depends more on trust than on bargaining, even at present. In fact, according to the study by Waltzman et al.15, pricing is only at the sixth place in terms of importance when a patient chooses a plastic surgeon, following academic title (first), recommendation (second), distance between home and clinic (third), decoration of the office (fourth), and surgeon experience (fifth). This study should be taken into account, although in our setting, the situation probably is different.
In an editorial published in the journal Plastic and Reconstructive Surgery, Rohrich16 asked in the title, "So you want to get paid for what you do?" In this article, Rohrich described the activity of plastic surgery as a union between physical activity and intellectually grounded knowledge and experience, and only comparable to a few activities such as playing an instrument or flying an airplane. Therefore, surgeons should not think of themselves only as "service providers" or "commodities," as their business requires much more than that. Similarly, without disparaging the role of the technologist, who plays a key role in the surgical team, surgeons should consider the technologist as having neither the ability nor the technical and intellectual knowledge of a trained plastic surgeon16.
On the question of what else affects job market trends, an important percentage of the volunteers (21. 9%) scored all the following alternatives: excessive number of active plastic surgeons, excessive number of recently graduated plastic surgeons joining the market, invasion of other specialties, and misdistribution of surgeons across cities. Only 7.6% indicated that the invasion of other specialties had the most impact, accounting for the fourth highest percentage of responses to this question. These indexes suggest that the plastic surgeon is much more concerned with other active plastic surgeons and members of the SBCP than with professionals from other specialties, or even from the so-called field of aesthetic medicine. The results for the item about the number of residents graduated in the state of Paraná confirms this. Most surgeons consider the number as excessive (62.4%), and most of the surgeons who provided this opinion had graduated 10-20 years previously (79.1%). Only 1% of the surveyed surgeons consider this number as small.
The controversy described herein has also occurred in other countries17. As stated at the beginning of this article, the problem of the job market is influenced by multiple factors, and no single main factor can be identified. Thus, several option should be considered.
Nonsurgical procedures have become important tools in the daily practice of plastic surgeons, which was confirmed by the index (82.1%) observed in this study. Over the years, the surgeons have added them to their arsenal of procedures to remain competitive and maintain their clientele18. The botulinum toxin injection is still the most cited procedure, followed by the use of hyaluronic acid fillers and peelings. These data confirm the findings from the Datafolha survey conducted by the SBCP9. These procedures, in most cases, complement other facial rejuvenation surgeries. Fortunately, the index of surgeons who perform polymethylmethacrylate injections or bioplasty was very low.
Finally, the item "medical fees" was analyzed. There was a balance between the surgeons who professionally targeted high fees in order to perform fewer surgeries (44.3%) and moderate fees in order to perform an average number of surgeries (38.7%). Even if these aims had not been achieved at the time of the survey, it represents the desired goals of the surgeons (Figure 7).
However, several aspects should be addressed in relation to the total net values and to the values considering only the surgeon's fees (Tables 8 and 9; Figures 3-6). First, a standard curve remained in almost all the graphs, which may be described as follows: the surgeons began charging a higher value after more than 5 years of graduation; between 5 and 10 years after graduation, this value was lowered significantly. However, it slightly increased between 10 and 20 years after graduation. The charged amounts were higher than average only after 20 years of training. This may be interpreted as struggling from competition. After years of graduation, medical practice, and further study, new surgeons attempt to charge the amount they believe is consistent with the sacrifice they have made. They then lower their prices after 5 years of graduation owing to the difficulty of self-maintenance and through observation of other colleagues that are doing the same. Between 10 and 20 years of graduation, even in the middle of a stiff competition, they slightly increase their fees to maintain the amount of work. After acquiring sufficient experience and recognition by the community for more than 20 years of practice, the surgeons finally increase their fees, and do not worry much about competitiveness. There is a second aspect to be addressed, that is, the younger surgeons only charged less than the experienced surgeons for liposuction surgery (equating to surgeons 10-20 years of graduation). This is probably because they have not yet encountered difficulties and complications in this surgery, even innocently believing that it is a simple procedure. The third aspect refers to surgeons who have graduated 10-20 years earlier who charge a mean value that is lower than those for all other categories, including blepharoplasty, rhinoplasty, and liposuction surgeries. The first 2 aspects may be explained by competition with other specialties (ophthalmology and otolaryngology), which utilizes health insurance plans to perform the same surgery. In contrast, the latter is probably justified only by the need of peer competition, as these surgeons probably already had experienced difficulties and complications inherent to liposuction. Other authors have also discussed this issue; it is not uniquely a local or national problem19.
Streu et al.20 evaluated the degree of satisfaction with plastic surgery outcomes in the United States. Despite finding a high degree of satisfaction (93%), the authors reported that surgeons with predominantly reconstructive practice and those who operated alone showed greater professional dissatisfaction. This kind of study would certainly be valid to complement the profile of our present specialists and provide a thorough discussion about the problems encountered in the field of plastic surgery in order to elucidate answers that will improve the future of the specialty.
CONCLUSIONS
The overall practice profile of the plastic surgeons in the state of Paraná reflects plastic surgeons who are concerned about the job market, by generally working in one city and seeking various alternatives to remain competitive, a situation that is most evident between 10 and 20 years after graduation.
REFERENCES
1. Rohrich RJ. The increasing popularity of cosmetic surgery procedures: a look at statistics in plastic surgery. Plast Reconstr Surg. 2000;106(6):1363-5.
2. Krieger LM, Shaw WW. The financial environment of aesthetic surgery: results of a survey of plastic surgeons. Plast Reconstr Surg. 1999;104(7):2305-11.
3. Krieger LM, Shaw WW. Aesthetic surgery economics: lessons from corporate boardrooms to plastic surgery practices. Plast Reconstr Surg. 2000;105(3):1205-10.
4. Krieger LM, Shaw WW. Pricing strategy for aesthetic surgery: economic analysis of a resident clinic's change in fees. Plast Reconstr Surg. 1999;103(2):695-700.
5. Constantian M. The media and plastic surgery: on being what you want to become. Plast Reconstr Surg. 2003;111(3):1348-9.
6. Rohrich RJ. The making of a plastic surgeon: present and future. Plast Reconstr Surg. 2003;111(3):1289-90.
7. Pearl RM, McAllister H, Pruzansky J. An economic analysis of health care reform and its implications for plastic surgery. Plast Reconstr Surg. 1997;99(1):1-9.
8. Pearl RM. An economic analysis of health care reform and its implications for plastic surgery: a five-year perspective. Plast Reconstr Surg. 2003;111(1):483-4.
9. Sociedade Brasileira de Cirurgia Plástica. Cirurgia Plástica no Brasil. Pesquisa Datafolha. Janeiro, 2009. Disponível em: http://www2.cirurgiaplastica.org.br/wp-content/uploads/2012/11/pesquisa2009.pdf Acesso: 5/8/2012
10. Hamilton MB. Online survey response rates and times background and guidance for industry. Disponível em: http://www.supersurvey.com/papers/supersurvey_white_paper_response_rates.pdf Acesso: 5/8/2012
11. Sheehan K. E-mail survey response rates: a review. JCMC. 2001;(6)2. Disponível em: http://jcmc.indiana.edu/vol6/issue2/sheehan.html
12. Krieger LM, Lee GK. The economics of plastic surgery practices: trends in income, procedure mix, and volume. Plast Reconstr Surg. 2004;114(1):192-9.
13. Rohrich RJ. The market of plastic surgery: cosmetic surgery for sale - at what price? Plast Reconstr Surg. 2001;107(7):1845-7.
14. Ribeiro R. Hora trabalhada de mecânico já custa o dobro da de médico. Folha de São Paulo, 01/07/2012. Disponível em: http://f5.folha.uol.com.br/humanos/1113560-hora-trabalhada-de-mecanico-ja-custa-o-dobro-da-de-medico.shtml Acesso: 5/8/2012
15. Waltzman JT, Scholz T, Evans GR. What patients look for when choosing a plastic surgeon: an assessment of patient preference by conjoint analysis? Ann Plast Surg. 2011;66(6):643-7.
16. Rohrich RJ. So you want to get paid for what you do? The saga continues. Plast Reconstr Surg. 2012;130(2):471-3.
17. Young RA. A plea for reducing the number of positions for residency training in plastic surgery. Plast Reconstr Surg. 1994;93(7):1523.
18. D'Amico RA, Saltz R, Rohrich RJ, Kinney B, Haeck P, Gold AH, et al. Risks and opportunities for plastic surgeons in a widening cosmetic medicine market: future demand, consumer preferences, and trends in practitioners' services. Plast Reconstr Surg. 2008;121(5):1787-92.
19. Prado AS, Parada F, Andrades P. Predatory pricing in plastic surgery. Plast Reconstr Surg. 2010;125(2):91e.
20. Streu R, Hawley S, Gay A, Salem B, Abrahamse P, Alderman AK. Satisfaction with career choice among U.S. plastic surgeons: results from a national survey. Plast Reconstr Surg. 2010;126(2):636-42.
1. Plastic surgeon, full member of Sociedade Brasileira de Cirurgia Plástica/Brazilian Society of Plastic Surgery (SBCP), Curitiba, PR, Brazil
2. Plastic surgeon, full member of SBCP, master in surgery at Evangelical Faculty of Paraná (FEPAR), president of SBCP-Regional Paraná, Curitiba, PR, Brazil
3. Plastic surgeon, full member of SBCP, member of the Scientific Committee of the Center for Integral Assistance to the Cleft Lip and Palate (CAIF), secretary of SBCP-Regional Paraná, Curitiba, PR, Brazil
4. Plastic surgeon, full member of SBCP, associate professor at the Federal University of Paraná (UFPR), head of the discipline and the Department of Plastic Surgery at UFPR, postdoctoral fellow at Yale University, full professor at the University of São Paulo (USP), treasurer of SBCP-Regional Paraná, Curitiba, PR, Brazil
Correspondence to: Luiz Roberto Reis de Araújo
Alameda Presidente Taunay, 1820 - Mercês
Curitiba, PR, Brazil - CEP 80430-042
E-mail: drluiz@drluizaraujo.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: October 7, 2012
Article accepted: February 1, 2013
This study was performed at the Brazilian Society of Plastic Surgery (SBCP) - Regional Paraná, Curitiba, PR, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket