



Original Article - Year 2012 - Volume 27 -
Evaluation of the main criteria of facial profile aesthetics and attractiveness
Avaliação dos principais padrões de perfil facial quanto a estética e atratividade
ABSTRACT
BACKGROUND: The parameters of beauty and facial attractiveness have a significant impact on the population because aesthetic standards are important factors of social acceptance. The aim of this study was to assess the major determinants of facial profile aesthetics and attractiveness according to laypeople and correlate the obtained results with ethnicity.
METHODS: A cohort of 125 patients (or their guardians) receiving treatment in municipal or private health care services in Caruaru, PE, Brazil, was analyzed. A defined sequence of 6 photos was shown to each individual, who then assigned a score of 0-10 for evaluation of aesthetics and beauty. The images were previously treated and manipulated using Adobe Photoshop CS3 and corresponded to the main criteria of facial profile (classes I, II, and III) and ethnicity.
RESULTS: Average values of 8.02 ± 1.63 were obtained for Caucasian class I, 6.60 ± 2.35 for African class I, 4.72 ± 2.71 for Caucasian class II, 4.23 ± 2.29 for African class II, 4.54 ± 2.33 for Caucasian class III, and 3.49 ± 2.10 for African class III. African facial profiles were considered statistically less attractive than Caucasian facial profiles.
CONCLUSIONS: The facial criteria of both Caucasian class I and African class I were the most attractive, whereas to the facial criteria of class III were less attractive. However, in this study, the African class received lower scores for aesthetics and attractiveness in all criteria.
Keywords: Esthetics. Perception. Facial asymmetry.
RESUMO
INTRODUÇÃO: Os parâmetros de beleza e atratividade facial exercem influência considerável na população, pois os padrões estéticos são vistos como importante fator para aceitação social. O objetivo deste estudo foi avaliar os principais padrões do perfil facial em relação aos parâmetros de atratividade estética na opinião de uma população leiga e relacionar os resultados com a raça.
MÉTODO: A amostra foi composta de 125 pacientes e/ou responsáveis sob os cuidados do serviço de saúde municipal e serviços privados, na cidade de Caruaru, PE, Brasil. A sequência específica de seis fotos foi mostrada para cada indivíduo, que atribuiu pontuação de 0 a 10 para a classificação de estética e beleza. As imagens tinham sido previamente tratadas e manipuladas usando o programa Adobe Photoshop CS3 e representavam os principais padrões do perfil facial (classes I, II e III) e tipos raciais.
RESULTADOS: Valores médios de 8,02 ± 1,63 foram obtidos para a classe I branca, 6,60 ± 2,35 para a classe I negra, 4,72 ± 2,71 para a classe II branca, 4,23 ± 2,29 para a classe II negra, 4,54 ± 2,33 para a classe III branca e 3,49 ± 2,10 para a classe III negra. Perfis faciais da raça negra foram estatisticamente considerados menos atraentes que os da raça branca.
CONCLUSÕES: O padrão facial de classe I foi considerado o mais atraente e o padrão de classe III o menos atraente, para as raças branca e negra. No entanto, neste estudo a raça negra recebeu notas mais baixas na avaliação de todos os padrões de perfil em relação a estética e atratividade.
Palavras-chave: Estética. Percepção. Assimetria facial.
Facial aesthetics is a major social concern. As reported by Kiekens et al.1, more than 70% of parents believe that their children will become more attractive, socially accepted, and successful in their professional life after orthodontic treatment. Many children, teenagers, adults, and parents think that pleasant facial aesthetics is a major factor of psychosocial wellbeing.
Most of the general population has significant malocclusions and/or abnormal growth of the facial skeleton that mainly affect the maxilla and/or mandible and influence facial proportions, thereby affecting aesthetics and attractiveness2. Orthodontics and maxillofacial surgery are dental specialties that enable the correction of tooth positioning as well as functional and dentofacial deformities, thus improving facial aesthetics and attractiveness. Patients with dentofacial deformities require careful examination by surgeons and orthodontists to improve their aesthetics and function. This examination consists of a detailed evaluation of the soft tissues, maxillofacial skeleton, and dentoalveolar relationship2.
However, the reasons for requesting orthodontic or orthosurgical treatments are not necessarily related to functional need, such as correction of chewing, talking, breathing, and psychological problems. Instead, people usually seek this treatment to improve their aesthetic appearance because other people's opinions directly or indirectly affect their self-esteem and how they perceive their own appearance2,3.
Several classifications such as that suggested by Reis et al.4 have been proposed to establish and guide the treatment of malpositioned teeth and facial asymmetry after facial evaluation according to frontal and lateral profiles. Based on this classification, facial patterns are divided in classes I, II, and III as well as long and short faces. Class I includes patients with an occlusion within the parameters of normality and facial symmetry. Classes II and III are characterized by a positive and negative sagittal relationship, respectively, between the maxilla and the mandible. The criteria for long and short faces were used to identify vertical discrepancies4.
Consistent with the findings of Todd et al.5, the clinical perception of facial aesthetics by dental professionals does not always correspond to that of the general population. This is due to the existence of significant differences among the opinions of dentists, orthodontists, and laypeople on the subjective morphological evaluation of dentofacial characteristics. Dental professionals normally prefer to work with patients in class I. Assessment of differences among classes is presumably based on changes in experience and knowledge. Therefore, more attention should be given to the requests, expectations, and self-evaluations of patients because aesthetic criteria may vary.
The aim of this study was to assess the main criteria of facial profile aesthetics and attractiveness (classes I, II, and III) from the perspective of laypeople and provide dental professionals with better suggestions about the actual expectations of patients and their families from the recommended treatment.
METHODS
This prospective, observational, descriptive, and cross-sectional study was performed in the form of a survey. The methodology proposed here satisfied bioethical requirements, and the study was approved by the Human Research Ethic Committee (CEP/ASCES 256/09).
Individuals or guardians that were considered eligible to participate in the study had undergone orthopedic or orthodontic preventive or corrective treatment. The non-probabilistic sample comprised 125 males and females of different ages, ethnicity, and cultural and socioeconomic origins. Each individual received clarification about the aims of the study and signed a consent form.
The participants were interviewed in the waiting room while waiting for treatment. To extensively diversify our cohort, patients were selected from both public and private orthodontic clinics in Caruaru, PE, Brazil.
Data acquisition was performed using a standard case report form that included questions about personal and demographic information as well as a visual analogue scale (VAS) from 0 to 10 (0-10) to score aesthetics and attractiveness. A specific sequence of 6 photos was shown to each individual and represented the main patterns of facial profile (classes I, II, and III) and ethnicity (Caucasian and African). Participants were instructed to evaluate each picture for up to 1 minute and give their opinion about aesthetics and attractiveness. To avoid a negative tendency in interpreting and evaluating the images, the pictures were distributed in 3 different sequences chosen randomly for each participant.
The participants were informed that the VAS score should correspond to an increased level of attractiveness (0, less attractive; 10, more attractive), as reported in earlier studies1,4,5. After the patient provided a score or after expiration of the time allotted to evaluate a photo, the next photo was immediately shown.
Pre-selected images were obtained of the right side profile of a female patient. Based on earlier studies6, the image was digitally treated and manipulated using Adobe Photoshop® CS3 (EUA) to obtain the criteria of classes I, II, and III. Moreover, the skin color was altered to establish ethnicity (Caucasian or African). Image processing was performed using the same original photo of a Caucasian female profile belonging to class I. After the digital manipulation, the images were printed on matte photo paper (15 cm × 21 cm) and laminated separately without a written or numerical identifier.
The scores assigned to each image are shown in Tables 1-3. Average values were calculated and classified into 4 categories:
category 1 (0-2.99 points) - unattractive facial aesthetics; category 2 (3-5.99 points) - reasonable aesthetics and attractiveness; category 3 (6-8.99 points) - pleasant aesthetics and attractiveness; category 4 (9-10 points) - very attractive facial aesthetics.
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 13.0, and an analysis of variance test was used to assess statistical significance (P < 0.05).
RESULTS
The average age of the 125 participants was 28.8 ± 10.9 years, and most were females (68.8%). The level of education was heterogeneous, and the largest class completed high school (33.1%) (Table 1).

Table 2 shows the mean values and standard deviations of the VAS scores for the attractiveness of each facial profile and ethnicity. Caucasian class I, which was considered the more attractive profile, received an average score of 8.02 ± 1.63. African class III, which was considered the least attractive profile, received an average score of 3.49 ± 2.10.
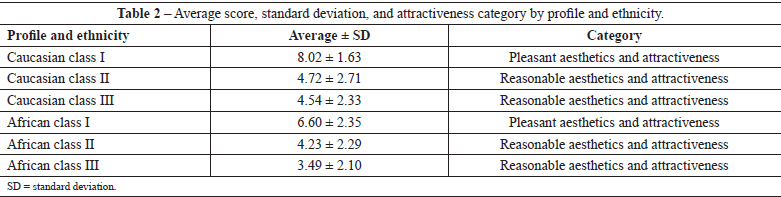
Table 3 shows the statistical correlations of VAS score between the different facial profiles and ethnicities. An F value was used to determine the differences within and among classes. Statistically significant differences were observed in the following comparisons: Caucasian class III vs. Caucasian class II; Caucasian class I vs. African class I; Caucasian class I vs. Caucasian class III; and African class II vs. African class III. Moreover, African classes II and III differed significantly from all of the other ethnic facial profiles (Caucasian classes I, II, and III and African class I). In contrast, no statistically significant differences were observed in the following comparisons: Caucasian class I vs. Caucasian class II; African class I vs. Caucasian class II; and African class I vs. Caucasian class III (P > 0.05) (Table 3).

DISCUSSION
Aesthetics can be defined as appreciation of the beauty or combination of qualities that please the senses. This concept continuously changes in different populations and historicalperiods6,7. Aesthetics is alsoinfluenced bygender, ethnicity, education, social, and environmental criteria6. In keeping with this notion, a heterogeneous cohort was evaluated in this study to minimize potential bias arising from the opinions of the individuals based on their social, cultural, racial, and economic origins as well as to illustrate the opinion of the racially mixed people that are present in Brazil.
Several studies have tried to determine the facial criteria responsible for pleasant or unpleasant aesthetic appearance1,3-12. These parameters rely on the harmonious balance between different parts of the face, which are considered one of the most important determinants of a "first impression" among an individual's physical traits6. Therefore, opinions concerning facial aesthetics are associated with harmony, balance, and proportionality of hard and soft tissues, as demonstrated by the highest scores being awarded to class I in the present study (Tables 2 and 3). Studies have also found that dental professionals and laypeople show an increased acceptance of the profile observed in class I 8,10.
The innovation of this study was the use of photos of both Caucasian andAfrican individuals to determine whether ethnicity affects the opinions of laypeople about aesthetics and attractiveness. This method also allowed an expectation overview of laypeople classified according to aesthetics and facial attractiveness.
The facial profiles in classes I, II, and III indicate a decreasing order of attractiveness. The facial profile in class I was found to be more attractive and aesthetically pleasant in studies involving dental professionals and laypeople7,11 in different countries, geographical regions, and cultures, with values that differ from the typical Western standards13. The results of the present study demonstrate that the profile in class I was the most attractive to Caucasians and Africans. This was an expected finding since the profile in class I displayed a clear proportion and harmony even among laypeople. However, it was interesting to find that the profile in class II received the second highest score, although it was significantly lower than that of class I. The profile of class II was classified as very attractive.
The dentofacial deformities observed in classes II and III lead to significant functional and aesthetic repercussions. Individuals with these facial profiles undergo orthosurgical correction to establish harmony and balance between the dental arches and the other thirds of the face. These procedures lead to a facial pattern that is similar to the dental and skeletal standards of class I. Therefore, it is essential to prove that this facial profile is the most requested by the overall population and corresponds to the most pleasant aesthetical criteria.
Regarding ethnicity, while African class I received the second highest score, the remaining African profiles were scored as the least aesthetic and attractive. Moreover, the African scores were significantly lower in all profiles compared to the corresponding Caucasian scores (Tables 2 and 3). This finding suggests that lay perceptions vary according to ethnicity, which leads us to believe that facial attractiveness is more closely related to ethnicity than facial pattern.
However, these statements are not conclusive because of the presence of several potential prejudices, e.g., the manipulated images used in the evaluation were derived from the same picture of a Caucasian woman and may have led to inadequate representations that impaired the average scores assigned by the interviewees. Moreover, with the exception of the skin color, other African anthropological traits such as the lip thickness, noses, and eyebrows were not efficiently recreated. This notion is supported by the finding that Caucasians were classified more homogenously than Africans, suggesting that the facial pattern was more evident in Caucasians. However, even with this limitation, African class I received the second highest score on the scale of attractiveness, meaning that it was aesthetically "pleasing." Further studies with greater emphasis on racial issues may further clarify the results obtained in the present investigation.
Regarding dentofacial discrepancies, it is estimated that approximately 10% of the general population has class II malocclusion, 2.5% has class III malocclusion, and 3% requires surgical correction for different dentofacial deformities. Therefore, opinions regarding the main determinants of facial profile aesthetics and attractiveness reveal an individual's expectations and serve as parameters for dental treatments that alter the orofacial morphology. Facial profiles considered less attractive (classes II and III) are subjected to different orthosurgical and/or odontologic treatments and undergo major morphological changes affecting function and aesthetics. As demonstrated by Edler et al.9, patients with less attractive facial profiles show major morphological changes in facial profiles after treatment.
When orthosurgical procedures are used for achieving an ideal facial profile, the initially aim should be to create functional improvement. Moreover, the need to correct dentofacial deformities by surgery should be discussed among the clinical team, patient, and the patient's family because aesthetic expectations may vary among individuals and may be influenced by the sociocultural context. It is essential to identify the facial criteria requested by the patients using scientific standards. Moreover, ethnic characteristics and the opinions of the patients and their families should be taken into consideration. Ethnic differences may explain the diversity of aesthetic preferences. However, other factors such as gender, age, education, social status, geographical location, and personal profile may also affect the preferences of different evaluators7.
CONCLUSIONS
The facial pattern in class I was more attractive than that in class III, which was considered less attractive for both Caucasians and Africans. However, in this study, Africans received the lowest scores in all the facial pattern profiles of aesthetics and attractiveness.
REFERENCES
1. Kiekens RM, Maltha JC, van't Hof MA, Kuijpers-Jagtman AM. Objective measures as indicators for facial esthetics in white adolescents. Angle Orthod. 2006;76(4):551-6.
2. To EWH, King WWK, Au O. Reshaping the face with orthognathic surgery: an overview. Disponível em: http://www.fmshk.org/article/862.pdf Acesso em: 20/7/2012
3. Vargo JK, Gladwin M, Ngan P. Association between ratings of facial attractivess and patients' motivation for orthognathic surgery. Orthod Craniofac Res. 2003;6(1):63-71.
4. Reis SAB, Abrão J, Capelozza Filho L, Claro CAA. Estudo comparativo do perfil facial de indivíduos padrões I, II e III portadores de selamento labial passivo. Rev Dent Press Ortodon Ortop Facial. 2006;11(4):36-45.
5. Macías Gago AB, Romero Maroto M, Crego A. The perception of facial aesthetics in a young Spanish population. Eur J Orthod. 2012;34(3):335-9.
6. Silva LM, Fukusima SS. Faces simétricas por reflexão das hemifaces não são mais atraentes que as faces naturais. Psicol Reflex Crít. 2010;23(3):466-75.
7. Little AC, Jones BC, DeBruine LM. Facial attractiveness: evolutionary based research. Phil Trans R Soc B Biol Sci. 2011;366(1571):1638-59.
8. Todd SA, Hammond P, Hutton T, Cochrane S, Cunningham S. Perceptions of facial aesthetics in two and three dimensions. Eur J Orthod. 2005;27(4):363-9.
9. Edler R, Agarwal P, Wertheim D, Greenhill D. The use of anthropometric proportion indices in the measurement of facial attractiveness. Eur J Orthod. 2006;28(3):274-81.
10. Johnston DJ, Hunt O, Johnston CD, Burden DJ, Stevenson M, Hepper P. The influence of lower face vertical proportion on facial attractiveness. Eur J Orthod. 2005;27(4):349-54.
11. Knight H, Keith O. Ranking facial attractiveness. Eur J Orthod. 2005;27(4):340-8.
12. Abu Arqoub SH, Al-Khateeb SN. Perception of facial profile attractiveness of different antero-posterior and vertical proportions. Eur J Orthod. 2011;33(1):103-11.
13. Lee LH, Jun JH, Danganan M, Pogrel MA, Kushner H, Lee JS. Orthognathic surgery for the Asian patient and the influence of the surgeon's background on treatment. Int J Oral Maxilofac Surg. 2011;40(5):458-63.
1. Dental Surgeon, Specialist in Morphological Sciences and Masters in Dentistry - Universidade Federal do Rio Grande do Norte, Natal, RN, Brazil.
2. Dental Surgeon by the Associação Caruaruense de Ensino Superior (Caruaruense Association of Higher Education - ASCES), Caruaru, PE, Brazil.
3. Adjunct Professor at ASCES. Specialist, Master, PhD and Post-doctoral student in Oral and Maxillofacial Surgery, Caruaru, PE, Brazil.
4. Graduated in Physical Education, Master in Adolescent Medicine, Doctoral Candidate in Nutrition, Adjunct Professor at Universidade Federal de Pernambuco (Federal University of Pernambuco), Recife, PE, Brazil.
5. Dental Surgeon, Master and Doctor in the Dental Clinic, Adjunct Professor of the Surgery and Maxillofacial Traumatology Course at the Faculdade de Odontologia de Pernambuco, Universidade de Pernambuco (Faculty of Dentistry of Pernambuco, University of Pernambuco), Camaragibe, PE, Brazil.
Correspondence to:
Marconi Eduardo Sousa Maciel Santos
Department of Dentistry, Faculty of Dentistry, Caruaruense Association of Higher Education
Av. Portugal, 584 - Universitario
Caruaru, PE, Brazil - CEP 55016-090
E-mail: marconimaciel@gmail.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: August 23, 2012
Article accepted: November 15, 2012
This work was performed at the Faculdade de Odontologia da Associação Caruaruense de Ensino Superior (Faculty of Dentistry of the Caruaruense Association of Higher Education), Caruaru, PE, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket