



Original Article - Year 2012 - Volume 27 -
A method to evaluate the SMAS suspension in facelift
Método de avaliação da suspensão do SMAS no rejuvenescimento facial
ABSTRACT
BACKGROUND: The superficial musculo-aponeurotic system (SMAS) suspension is a globally accepted procedure in rhytidoplasties. In order to evaluate the efficacy of suspension performed with the round block SMAS treatment, the authors planned a method in which the wound area reduction is measured to assure its functionality, based in clear evidence.
METHODS: Twenty consecutive rhytidoplasties were evaluated, all of them done by the same surgeon, using the same standards. Twelve measures were taken in each side of the face, 7 before suspension and 5 after, allowing for the elaboration of 40 diagrams comprising the areas evaluated before and after suspension. The software ImageJ (NIH Image) was used to evaluate the surfaces.
RESULTS: The undermined area in the 40 measures had a mean of 52.6 cm2, which changed to a mean of 32.6 cm2 after suspension, with a mean reduction of 38%. The diagrams also showed the exact handled points of the face.
CONCLUSIONS: The described methodology confirms that the round block SMAS treatment technique is efficient regarding the suspension of the superficial muscular aponeurotic system, with significant reduction of the undermined area, consequently reducing the dead space, and may be a parameter to comparison of different techniques.
Keywords: Face/surgery. Rhytidoplasty. Evaluation of results of therapeutic interventions.
RESUMO
INTRODUÇÃO: A suspensão do sistema musculoaponeurótico superficial (SMAS) é um procedimento amplamente aceito nas ritidoplastias. Com o objetivo de avaliar a eficácia de tal suspensão na técnica de tratamento do SMAS em round block com cicatrizes curtas, foi proposto método em que a redução da área descolada é avaliada ao final da cirurgia, assegurando sua eficácia, baseada em clara evidência.
MÉTODO: Foram analisadas 20 cirurgias consecutivas de ritidoplastia, todas realizadas pelo mesmo cirurgião, com os mesmos padrões. Foram tomadas 12 medidas em cada lado da face, 7 antes e 5 após a realização da suspensão, permitindo a elaboração de 40 diagramas compreendendo as áreas avaliadas antes e após o procedimento. Foi utilizado o software ImageJ (NIH Image) para cálculo das áreas.
RESULTADOS: A área descolada nas 40 medidas apresentou média de 52,6 cm2, mudando para 32,6 cm2 após a suspensão, com redução média de 38%. Os diagramas obtidos refletiram a exata atuação nos diversos pontos da face.
CONCLUSÕES: O método descrito confirma que a técnica é eficiente quanto à suspensão do SMAS, com redução significativa da área descolada e consequente diminuição do espaço morto pós-operatório, e pode servir como parâmetro para comparação de diferentes técnicas.
Palavras-chave: Face/cirurgia. Ritidoplastia. Avaliação de resultado de intervenções terapêuticas.
Rhytidoplasty is a cosmetic surgery usually done in a phase of life when patients know what they want and look for a plastic surgeon whose profile will offer the naturalness they are intending to obtain. Although non-surgical options, as botulinum toxin and fillers, have been widely used, the space for this surgery will be preserved. Increase in life expectancy together with the fact that tissue laxity will be unavoidable at least for a long time, and the current desire of having a young aspect that meets the constantly improved physical condition shown by aging people, all make rhytidoplasty a highly sought-after procedure nowadays. Safer anesthetic procedures, restrained cases postponed by noninvasive techniques, and the contingent of patients who underwent bariatric surgery require well-defined parameters based on reliable evidence.
Although the authors sought to find an established method to quantify wound area reductions after a rhytidoplasty, they have not come upon any papers published about this topic. This routine was conceived to supply this omission.
It is globally accepted that the superficial muscular aponeurotic system (SMAS)1 needs some kind of treatment during a facelift. In the present study, the authors propose an objective, methodized evaluation of a very well-determined parameter: the reduction of the undermined surface during rhytidoplasty procedures, performed according to the technique named short scar facelift with the roundblock SMAS treatment2,3.
All steps are clearly explained, so any surgeon will be able to create the diagrams and evaluate the areas as shown in the article, and compare the results used in his technique with this new parameter.
METHODS
A prospective clinical study was performed in 2012. Patients included in this study comprised those who consulted the senior author in his private clinic for facial rejuvenation surgery, and opted for a short-scar facelift (the details of which having been published before)3.
Twenty women, with ages ranging from 39 to 74 years (mean of 57.6 years) underwent rhytidoplasty. There were 11 primary facelifts, 6 secondary, 1 tertiary, 1 quaternary and 1 quinary (Table 1). The only exclusion criterion was contraindication to the short scar facelift with round block SMAS treatment.

Surgical Technique
All patients underwent general anesthesia, and all procedures were performed by the same surgeon.
After the areas to be treated were infiltrated with a 1:500,000 epinephrine solution in normal saline, the cervical area was treated according to necessity, which is not the scope of this study. Subsequently, an incision was made, always starting at the base of the left sideburn, then running inside the sideburn hair up to the superior site of auricle implantation. Then the incision continues downward before the auricle (upper tragal region), contouring the earlobe and extending through the retroauricular region up to the approximate projection of the first incision.
Subcutaneous undermining is performed according to the described technique.
Twelve measures were taken in each side of the face, 7 before suspension and 5 after, allowing for the elaboration of 40 diagrams comprising the areas evaluated before and after suspension. The undermined areas are measured according to the following patterns (Figures 1 to 7).

Figure 1 - Measure nº. 1, preauricular

Figure 2 - Measure nº. 2, postauricular.

Figure 3 - Measure nº. 3, parallel to sideburn.

Figure 4 - Measure nº. 4, from the upper tragus toward the labial external cantus.

Figure 5 - Measure nº. 5, along the mandible, starting from the site of earlobe implantation.

Figure 6 - Measure nº. 6, perpendicular to the site of earlobe implantation.

Figure 7 - Measure nº. 7, parallel to the posterior upper incision.
preauricular (measure no. 1); postauricular (measure no. 2); parallel to sideburn (measure no. 3); from the upper tragus toward the labial external cantus (measure no. 4); along the mandible, starting from the site of earlobe implantation (measure no. 5); perpendicular to the site of earlobe implantation (measure no. 6) parallel to the posterior upper incision (measure no. 7).
The circular plication of the SMAS was done starting always in the posterior region of the ear, running toward the neck and face, and extending up to the sideburn incision (Figure 8). The needle was passed in a cranial and posterior direction to place the thread behind the auricle (Figure 9), bringing it back to the anterior region, in order to be pulled (Figure 10) and tied, thus performing the SMAS suspension. Measures 3 to 7 were taken again. Excess skin was excised, and sutures were done. The same procedure was performed on the right side of the face.

Figure 8 - Facial plicature.

Figure 9 - Needle passed.

Figure 10 - Tractioned thread.
RESULTS
Based on the measures obtained, 40 diagrams were elaborated (Diagrams 1 to 20, right and left sides), in which the shaded area shows the reduction in each case (Figures 11 and 12). Those areas were analyzed using the ImageJ software.

Figure 11 - Diagrams of the patients 1 to 10.

Figure 12 - Diagrams of the patients 11 to 20.
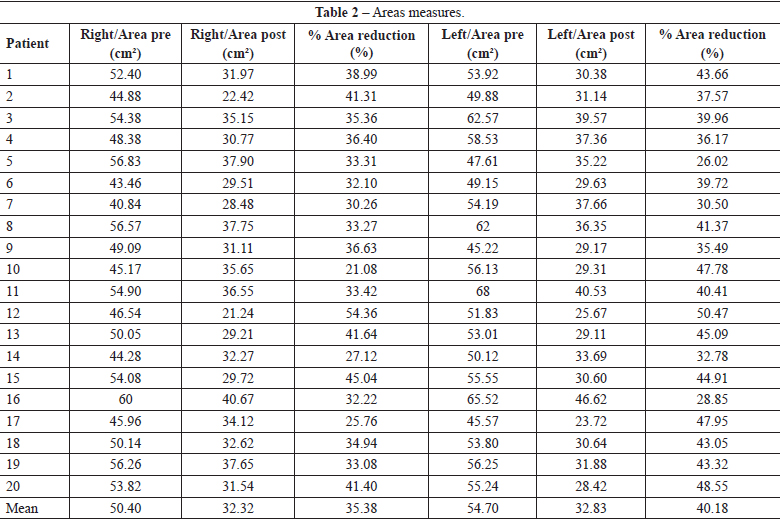
A variation in the undermined areas was verified ranging from 40.84 cm2 to 60 cm2 (mean of 50.4 cm2) on the right side of the face, and from 45.22 cm2 to 68 cm2 (mean of 54.7 cm2) on the left side. After suspension, the right side showed a variation ranging from 21.24 cm2 to 37.9 cm2 (mean of 32.32 cm2), and the left side from 23.72 cm2 to 46.62 cm2 (mean of 32.83 cm2). The area reduction on the right side ranged from 21.08% to 54.36% (mean of 35.38%), while on the left side, there was a variation ranging from 26.02% to 50.47% (mean of 40.18%) (Table 2). Considering both sides, the average undermined area measured 52.55 cm2, and the final average area measured 32.58 cm2, with an average reduction of 38%.
DISCUSSION
Treatment comprising any of the multiple options of techniques that approach the SMAS4-11 is a relevant surgical step in rhytidoplasty procedures. However, considering that the evaluation of the effectiveness of each technique has lately been kept restricted to photographic analyses and subjective impressions, the authors felt it was necessary to plan a quantitative evaluation of the techniques of SMAS suspension, at least at surgery end time.
The aim of this study was to offer a standard for comparison of measures, in the light of a method of SMAS suspension, and not to praise the used technique. It is important to emphasize that the diagrams accurately represent the areas that suffered greater or lighter traction.
CONCLUSIONS
The round block SMAS treatment has been shown to be capable of yielding a 38% reduction in surgically-undermined areas, with the purpose of allowing pleasant facial rejuvenation. Since that there is no other parameter to compare, this paper may be used as a reference for evidence-based evaluation of the efficacy of different rhytidoplasty techniques.
REFERENCES
1. Mitz V, Peyronie M. The superficial musculo-aponeurotic system (SMAS) in the parotid and cheek area. Plast Reconstr Surg. 1976;58(1):80-8.
2. Stocchero IN. The roundblock SMAS treatment. Plast Reconstr Surg. 2001;107(7):1921-3.
3. Stocchero IN. Shortscar face-lift with the roundblock SMAS treatment: a younger face for all. Aesthetic Plast Surg. 2007;31(3):275-8.
4. Duminy F, Hudson DA. The mini rhytidectomy. Aesthetic Plast Surg. 1997;21(4):280-4.
5. Saylan Z. The S-lift: less is more. Aesthetic Surg J. 1999;19(4):406-9.
6. Tonnard P, Verpaele A, Monstrey S, Van Landuyt K, Blondeel P, Hamdi M, et al. Minimal access cranial suspension lift: a modified S-lift. Plast Reconstr Surg. 2002;109(6):2074-86.
7. Baker DC. Minimal incision rhytidectomy (short scar face lift) with lateral SMASectomy: evolution and application. Aesthetic Surg J. 2001;21(1):14-26.
8. Marchac D. Against the "visible" short scar face lift. Aesthet Surg J. 2008;28(2):200-8.
9. Marchac D, Nasr au lieu de Nask M. Avoiding the operated on look in multiple face lifts. J Plast Reconstr Aesthet Surg. 2008;61(12):1449-58.
10. Marchac D. Évaluation de 50 liftings cervicofaciaux monobloc avec suspension. Ann Chir Plast Esthet. 2009;54(2):103-11.
11. van der Lei B, Cromheecke M, Hofer SO. The purse-string reinforced SMASectomy short scar facelift. Aesthet Surg J. 2009;29(3):180-8.
1. Assistant professor of the Plastic Surgery Department of the Faculdade de Medicina do ABC, full member of the Sociedade Brasileira de Cirurgia Plástica/ Brazilian Society of Plastic Surgery (SBCP), medical director of the Centro Médico Viver Melhor, São Paulo, SP, Brazil.
2. Full member of the SBCP, plastic surgeon of the University Hospital of the Universidade de São Paulo, São Paulo, SP, Brazil.
3. Aspirant member of the SBCP, trainee of the Instituto de Cirurgia Plástica Santa Cruz, São Paulo, SP, Brazil.
4. Full member of the SBCP, associate physician of the Instituto do Câncer do Estado de São Paulo, São Paulo, SP, Brazil.
Correspondence to:
Ithamar Nogueira Stocchero
Rua Abílio Soares, 1.337
São Paulo, SP, Brazil - CEP 04005-005
E-mail: dr.ithamar@vivermelhor.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: June 22, 2012
Article accepted: August 5, 2012
This study was performed at the Centro Médico Viver Melhor, São Paulo, SP, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket