



Original Article - Year 2012 - Volume 27 -
Surgical approach to the treatment of gynecomastia according to its classification
Abordagem cirúrgica para o tratamento da ginecomastia conforme sua classificação
ABSTRACT
BACKGROUND: Gynecomastia is the most common benign proliferation of the glandular tissue of the male breast and is caused by an alteration of the balance between estrogen and androgen concentrations. In most cases, the treatment of choice is surgery. In this study, we aimed to indicate the efficacy of established surgical procedures for the correction of gynecomastia, as evaluated according to Simon's classification, and to present a novel contribution.
METHODS: This study was performed between March 2009 and March 2011. It included 32 male patients, aged between 13 and 45 years. The type of incision was chosen on the basis of the need for skin resection. We used 4 techniques described in the literature and a modified procedure of circular incision with inferior, superior, lateral, and medial extensions, which we employed when excess skin was also present in the lower pole of the breast.
RESULTS: Idiopathic gynecomastia was the most common etiology among our patients, followed by obesity and by use of anabolic steroids.
CONCLUSIONS: The common procedure to correct gynecomastia was based on the inferior periareolar incision proposed by Webster, which we employed in patients who did not require skin resection. In the presence of excess skin, the technique chosen varied according to the amount of tissue to be resected. In the present report, we propose a novel technique that facilitates larger dermal, glandular, and fatty breast tissue removal when compared to other procedures previously used by this surgeon.
Keywords: Plastic surgery/methods. Breast/surgery. Gynecomastia.
RESUMO
INTRODUÇÃO: A ginecomastia é a proliferação benigna mais comum do tecido glandular da mama masculina, causada pela alteração do equilíbrio entre as concentrações de estrógeno e andrógeno. Na maioria dos casos, o principal tratamento é a cirurgia. O objetivo deste trabalho foi demonstrar a aplicabilidade das técnicas cirúrgicas consagradas para a correção da ginecomastia, de acordo com a classificação de Simon, e apresentar uma nova contribuição.
MÉTODO: Este trabalho foi realizado no período de março de 2009 a março de 2011, sendo incluídos 32 pacientes do sexo masculino, com idades entre 13 anos e 45 anos. A escolha da incisão foi relacionada à necessidade ou não de ressecção de pele. Foram utilizadas quatro técnicas da literatura e uma modificação da técnica por incisão circular com prolongamentos inferior, superior, lateral e medial, quando havia excesso de pele também no polo inferior da mama.
RESULTADOS: A principal causa da ginecomastia identificada entre os pacientes foi idiopática, seguida pela obesidade e pelo uso de esteroides anabolizantes.
CONCLUSÕES: A técnica mais utilizada foi a incisão periareolar inferior proposta por Webster, quando não houve necessidade de ressecção de pele. Na presença de excesso de pele, a técnica escolhida variou de acordo com a quantidade do tecido a ser ressecado. A nova técnica proposta permitiu maior remoção do tecido dermocutâneo glandular e gorduroso da mama, quando comparada às demais técnicas utilizadas na experiência do cirurgião.
Palavras-chave: Cirurgia plástica/métodos. Mama/cirurgia. Ginecomastia.
Gynecomastia affects 40-65% of adult men and is characterized by a soft, symmetrical, and discoid enlargement of the male breast1-5. Gynecomastia is known as the most common benign proliferation of the glandular tissue of the male breast and is usually caused by an increased concentration of estrogen as a consequence of aging, disease, drug consumption, or idiopathic factors. In rare cases the condition may be caused by an endocrine tumor1,2,6,7. Gynecomastia progresses as a result of an alteration in the balance between estrogen and androgen concentrations1. This balance is essential for normal breast cell growth.
Classifications of different grades of gynecomastia have been proposed; among these, Simon's classification is the most accepted1,7, and it has been adopted in the present study.
Gynecomastia may result from physiological changes during growth and development or may be pathologically induced. There are 3 peaks of physiologic gynecomastia. The first occurs during the neonatal period and the second occurs during puberty, usually regressing by approximately age 17 years. In both cases, gynecomastia usually regresses spontaneously. The third peak occurs in older men and seems to have a variety of causes, such as a decrease in testosterone due to testicular aging2,4,7-10.
The correlation between male breast cancer and gynecomastia is controversial, with reported coexistence ranging from 2% to 35%; however, there is much evidence to suggest that the 2 conditions are not related1,6.
Most cases are idiopathic, and surgery is the primary choice of treatment for patients whose gynecomastia does not regress spontaneously or when psychosocial issues become severe3,7. Recently, several hormonal therapies have been suggested for the treatment of gynecomastia but have not met with success1,6,7.
The second leading cause of gynecomastia is due to the use of drugs that may trigger this condition. In this case, however, gynecomastia in adult males is usually considered a side effect compared to the other adverse effects caused by the body's reaction to consumption of the drug1. Risperidone, phenothiazine, selective serotonin (5-hydroxytryptamine; 5HT) reuptake inhibitors, methyldopa, tricyclic antidepressants, marijuana, heroin, saquinavir, minocycline, finasteride, sulpiride, and domperidone are some drugs that have been reported to induce gynecomastia1,4-6,11,12.
The diagnosis requires a careful analysis of the patient's clinical history and physical examination2,6. The detection of a palpable mass in a male patient's breast could lead to the diagnosis of pseudogynecomastia, gynecomastia, breast cancer, and numerous other benign conditions.
The most common surgical procedure employed for gynecomastia treatment is subcutaneous mastectomy, which involves resection of the glandular tissue by a periareolar or transareolar approach, with or without liposuction. Skin resection is required in patients presenting with accentuated breast size, ptosis, and excess skin6,8. The main problems caused by the surgery are unsightly scars, redundant skin, and migration of the nipple7.
The aim of this study was to indicate the efficiency of 4 established surgical procedures for the correction of gynecomastia, as categorized by Simon's classification. We also present a modification of the circular incision technique with superior, lateral, and medial extensions that may be used when excess skin is also present in the lower pole of the breast.
METHOD
The study was conducted between March 2009 and March 2011. We selected 32 male patients between 13 and 45 years who were referred to Plastic Surgery Service of the Hospital Belo Horizonte/FELUMA da Faculdade de Ciências Médicas de Minas Gerais (Hospital of Belo Horizonte/ FELUMA of the Faculty of Medical Sciences of Minas Gerais, Belo Horizonte, MG, Brazil) or who presented to the clinic voluntarily. All patients showed dissatisfaction with their condition and sought an aesthetic correction.
The following information was recorded: name, age, weight, height, grade of gynecomastia according to Simon's classification, location (unilateral or bilateral), time of evolution, skin color, cause of gynecomastia, symptoms (aesthetics, palpable mass, pain, or papillary discharge).
The choice of the procedure was based on Simon's classification and the need for skin resection. Surgical correction of gynecomastia in this study was performed using the techniques described below.
1. Inferior periareolar incision (proposed by Webster): This technique was used in cases of gynecomastia without excess skin, as described by Freitas and Mélega13.
2. Periareolar circular incision: This technique was applied in cases of gynecomastia with excess skin, as described by Camargos et al.14 and Cunha et al.15.
3. Inferior periareolar incision with superior, lateral, and medial extensions: This technique was applied in cases of gynecomastia with excess skin. First, the ideal position for the papillary-areola complex (PAC) was preoperatively marked. However, due to the superior, medial, and lateral excess skin, additional marks were made with incision extensions in regions measured with a bidigital maneuver (flying saucer), which allowed the resection of as much skin as possible. This avoided flaccidity upon removal of the glandular and fatty tissue and improved PAC positioning. The vertical bipedicled de-epidermized flap was maintained, as per McKissock, to promote a proper blood flow through the PAC16.
4. Periareolar circular incision with transverse lateral extension: This technique was applied in cases of gynecomastia with excess skin. The preoperative planning followed the same procedure described in 2. However, because of the larger amount of excess lateral skin in the thoracic region, lateral marks were made with a bidigital maneuver, allowing for a greater skin resection without extending beyond the anterior axillary line16.
5. Circular incision with inferior, superior, lateral, and medial extensions (personal modification): This technique is a personal modification developed inside the clinic that was applied to patients who required a wider resection of breast tissue in the lower pole. It consisted of a modification of the inferior periareolar incision with superior, lateral, and medial extensions. The preoperative mark followed the same procedure as described in 3; however, in addition, an inferior mirror extension was also performed. The bipedicled flap was maintained (option 1) or, when necessary, resection of the inferior pedicle was performed (option 2), allowing for better PAC accommodation. The procedure is illustrated in Figures 1 to 7.
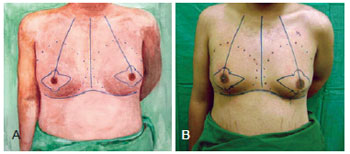
Figure 1 - Preoperative marking for a circular incision with inferior, superior, lateral, and medial extensions.
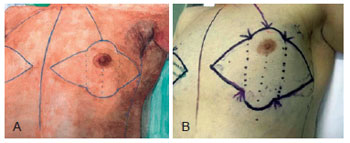
Figure 2 - Detailed preoperative marking for a circular incision with inferior, superior, lateral, and medial extensions.

Figure 3 - PAC de-epidermization with the medial and lateral extension incisions used in the circular incision technique with inferior, superior, lateral, and medial extensions.
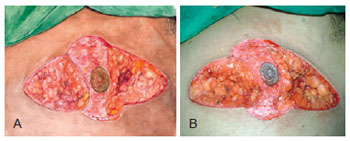
Figure 4 - Resection of medial and lateral regions in the circular incision technique with inferior, superior, lateral, and medial extensions.

Figure 5 - Bipedicle PAC flap (option 1) in the circular incision technique with inferior, superior, lateral, and medial extensions.
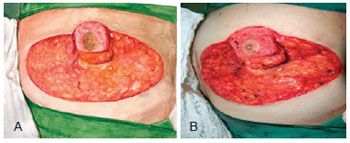
Figure 6 - Resection of the lower pedicle of PAC (option 2) in the circular incision technique with inferior, superior, lateral, and medial extensions
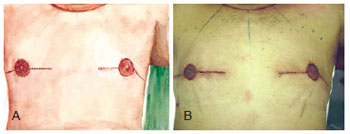
Figure 7 - Immediate postoperative result after circular incision with inferior, superior, lateral, and medial extensions.
RESULTS
The data of the 32 patients included in this study, obtained during the anamnesis, includes information on the procedures used, the weight of breast tissue removed, whether associated liposuction was performed, any postoperative complications, and patient satisfaction level.
Figure 8 shows the main causes of gynecomastia in the patients evaluated in this study, whereas Figure 9 shows gynecomastia etiologies according to age group.
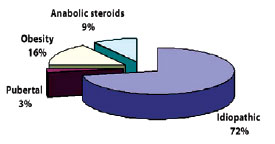
Figure 8 - Leading causes of gynecomastia.
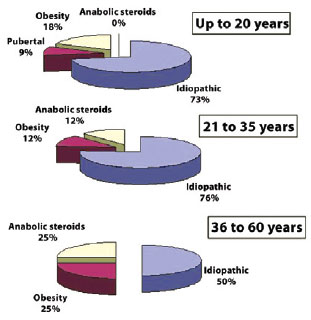
Figure 9 - Gynecomastia etiologies according to patient age.
Figure 10 presents the distribution of incisions used in this study.
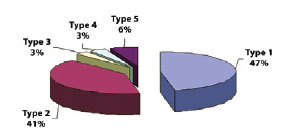
Figure 10 - Distribution of incision procedures. Type 1 = inferior periareolar incision proposed by Webster; Type 2 = periareolar circular incision; Type 3 = inferior periareolar incision with superior, lateral, and medial extensions; Type 4 = periareolar circular incision with lateral transverse extension; Type 5 = circular incision with inferior, superior, lateral, and medial extensions.
Laboratory examinations did not reveal any evidence of pathology associated with gynecomastia in the patients evaluated. Pathological examinations confirmed the presence of gynecomastia in all cases.
Figure 11 associates the surgical procedures employed to the grade of gynecomastia according to Simon's classification.
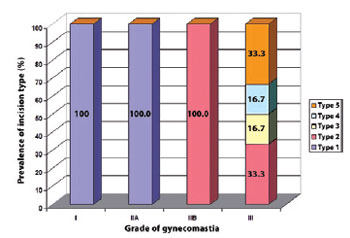
Figure 11 - Correlation between the prevalence of incision type used and the grade of gynecomastia according to Simon's classification. Type 1 = inferior periareolar incision proposed by Webster; Type 2 = periareolar circular incision; Type 3 = inferior periareolar incision with superior, lateral, and medial extensions; Type 4 = periareolar circular incision with lateral transverse extension; Type 5 = circular incision with inferior, superior, lateral, and medial extensions.
Figures 12 to 15 present preoperative and 6-month postoperative photographs of several patients.

Figure 12 - Patient TB, gynecomastia grade IIA, treated with inferior periareolar incision. In A, preoperative appearance. In B, 6-month postoperative appearance.
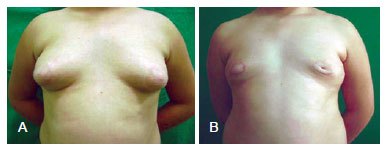
Figure 13 -Patient DT, gynecomastia grade III, treated with periareolar circular incision. In A, preoperative appearance. In B, 6-month postoperative appearance.

Figure 14 - Patient LF, gynecomastia grade III, treated with circular periareolar incision with lateral transverse extension. In A, preoperative appearance. In B 6-month postoperative appearance.

Figure 15 - Patient DF, gynecomastia grade III, treated with circular incision with inferior, superior, lateral and medial extensions. In A, preoperative appearance. In B, 6-month postoperative appearance.
DISCUSSION
The leading cause of gynecomastia is idiopathic, as other authors have found3,7, followed by obesity and use of anabolic steroids. These latter 2 causes reflect, in part, the profile of modern society, in which an excessive weight gain is linked to a sedentary lifestyle or to disorders that might be derived from it, such as anxiety, depression, and others. On the other hand, the use of drugs for aesthetic purposes is a fast and easy way to modify the appearance, although the result is achieved through an alteration of hormone concentrations. It was found that obesity is the second leading cause of gynecomastia in all age groups, particularly in patients aged less than 20 years old. In patients aged over 20 years, anabolic steroids are the second leading cause of gynecomastia.
The main procedure used in this study for the correction of gynecomastia was the inferior periareolar incision proposed by Webster, because most of the patients did not present with excess skin. This is a simple technique, which leaves a good quality scar that is barely noticeable in most cases; it is used with Simon's classification grade I and IIA. All the patients were satisfied with the aesthetic result 6 months after surgery, which may be attributed to the small size required for the incision and its location.
In cases in which the excision of excess skin was required, the surgical technique most often used was the circular periareolar incision, which was applied to more than 40% of the patients with grades of gynecomastia varying between IIB and III. This technique requires additional surgical care to render the scar acceptable. Moreover, this procedure showed a higher number of complications (38.5%) such as hypertrophic and keloid scars, which accounted for 60% of the complications observed. The complaints were mainly from patients whose obesity was the cause of gynecomastia and where the weight of material removed from the breasts was more than 100 g. These complications were associated with early physical activity performed by the patients, which generated an increased tension in the scar leading to dehiscence, hypertrophic scars, and keloids. With an aim toward avoiding future complications in other patients, the surgeon applied a higher number of subdermal stitches and reinforced the postoperative recommendations.
In cases that were classified as grade III according to Simon, in which more excess skin is involved, elaborate techniques were employed, including the modification proposed herein. This consists of a circular incision with inferior, superior, lateral, and medial extensions. This new surgical contribution allowed a larger removal of excess dermal, glandular, and fatty tissue, which, in the experience of the surgeon, leads to patient satisfaction. All patients with gynecomastia who were treated with the incision described in points 3, 4, and 5 in the Methods were satisfied with their results 6 months after surgery. This was also achieved by an extensive experience in closing the tissue with a higher number of subdermal stitches, which prevented damage during healing. Patients were instructed to better collaborate in their recovery activities, by avoiding physical exertion, not raising their arms above the shoulder for at least 20 days, and using a compression vest for at least 30 days.
CONCLUSIONS
The surgical approach used in this study for the treatment of gynecomastia varied according to Simon's classification. Through these results, we conclude that, in cases in which the resection of skin was not required, the inferior periareolar incision proposed by Webster was the best option. In cases wherein excess skin is present, the chosen procedure varied according to the amount of tissue that had to be resected. All the established procedures indicated their importance and efficacy in the correction of gynecomastia; however, in cases in which a more extensive resection of breast tissue in the lower pole was required, the modified technique presented in this study exhibited the best aesthetic result and satisfaction level, according to the patients.
REFERENCES
1. Daniels IR, Layer GT. Gynaecomastia. Eur J Surg. 2001;167(12):885-92.
2. Hassan HC, Cullen IM, Casey RG, Rogers E. Gynaecomastia: an endocrine manifestation of testicular cancer. Andrologia. 2008;40(3):152-7.
3. Ridha H, Colville RJ, Vesely MJ. How happy are patients with their gynaecomastia reduction surgery? J Plast Reconstr Aesthet Surg. 2009;62(11):1473-8.
4. Steele RS, Martin MJ, Place RJ. Gynecomastia: complications of the subcutaneous mastectomy. Am Surg. 2002;68(2):210-3.
5. Kaneda Y, Fujii A. Gynecomastia with sulpiride. J Clin Pharm Ther. 2002;27(1):75-7.
6. Johnson RE, Murad MH. Gynecomastia: pathophysiology, evaluation, and management. Mayo Clin Proc. 2009;84(11):1010-5.
7. Autorino R, Perdonà S, D'Armiento M, De Sio M, Damiano R, Cosentino L, et al. Gynecomastia in patients with prostate cancer: update in treatment options. Prostate Cancer Prostatic Dis. 2006;9(2):109-14.
8. Coskun A, Duzgun SA, Bozer M, Akinci OF, Uzunkoy A. Modified technique for correction of gynaecomastia. Eur J Surg. 2001;167(11):822-4.
9. Rosewater S, Gwinup G, Hamwi GJ. Familial gynecomastia. Ann Intern Med. 1965;63:377-85.
10. Einav-Bachar R, Philip M, Aurbach-Klipper Y, Lazar L. Prepubertal gynaecomastia: aetiology, course and outcome. Clin Endocrinol (Oxf). 2004;61(1):55-60.
11. Kaiyadan F, Gopinath S, Jayasree MG, Parmar C. Finasteride-induced gynaecomastia. Indian J Dermatol Venerol Leprol. 2009;75(3):309-10.
12. Caocci G, Atzeni S, Orru N, Azzena L, Martorana L, Littera R, et al. Gynecomastia in a male after dasatinib treatment for chronic myeloid leukemnia. Leukemia. 2008;22(11):2127-8.
13. Freitas AG, Mélega JM. Ginecomastia. In: Mélega JM, eds. Cirurgia plástica: fundamento e arte. Cirurgia reparadora de troncos e membros. São Paulo: MEDSI; 2002. p.19-27.
14. Camargos AG, Ferreira EM, Ferreira FPM, Lima JCSA. Correção de ginecomastia pela via periareolar circular: uma alternativa para ressecção do excesso de pele. Rev Soc Bras Cir Plást. 2007;22(2):107-15.
15. Cunha MTR, Bento JFG, Bozola AR. Periareolar mammaplasty for treatment of gynecomastia with breast ptosis and excess skin. Int J Cosm Surg Aesth Derm. 2004;5(2):178-84.
16. McKissock PK. Reduction mammaplasty by the vertical bipedicle flap technique: rationale and results. Clin Plast Surg. 1976;3(2):309-20.
Full Member of the Sociedade Brasileira de Cirurgia Plástica (Brazilian Society of Plastic Surgery), medical residency preceptor of the Hospital Belo Horizonte/FELUMA da Faculdade de Ciências Médicas de Minas Gerais (Hospital of Belo Horizonte/FELUMA of the Faculty of Medical Sciences of Minas Gerais), Belo Horizonte, MG, Brazil.
Correspondence to:
Mário Múcio Maia de Medeiros
Hospital Belo Horizonte
Av. Antônio Carlos, 1694 - Térreo - Sala 13 - Cachoeirinha
Belo Horizonte, MG, Brazil - CEP 31210-010
E-mail: mariomaia.plastica@gmail.com
Article submitted to SGP (Sistema de Gestão de Publicações/ Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: May 2, 2012
Article accepted: June 20, 2012
This study was performed at the Plastic Surgery Service of the Hospital Belo Horizonte/ FELUMA da Faculdade de Ciências Médicas de Minas Gerais (Hospital of Belo Horizonte/FELUMA of the Faculty of Medical Sciences of Minas Gerais), Belo Horizonte, MG, Brazil.
This study was presented at the 48th Brazilian Congress of Plastic Surgery, Goiânia, 2011. The author passed the examination and was promoted to full member of Sociedade Brasileira de Cirurgia Plástica (Brazilian Society of Plastic Surgery).
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket