



Original Article - Year 2012 - Volume 27 -
Comparison of the aesthetic outcomes of breast reconstruction by using ipsilateral or contralateral TRAM flaps
Análise dos resultados estéticos na reconstrução mamária com TRAM ipsilateral vs. contralateral
ABSTRACT
BACKGROUND: Breast reconstruction by using the rectus abdominis muscle (transverse rectus abdominis myocutaneous, TRAM) flaps is a common procedure that has been performed since the 1990s. Ipsilateral TRAM flaps were proven to be as safe as contralateral flaps for breast reconstruction. However, studies comparing the aesthetic outcomes of the two procedures are poorly described in the literature. The aim of this study was to compare the cosmetic outcomes of ipsilateral and contralateral pedicled flaps.
METHODS: We prospectively evaluated 29 cases of immediate reconstruction with ipsilateral (group 1) or contralateral (group 2) TRAM flaps. The aesthetic outcomes were analyzed and the two groups were compared.
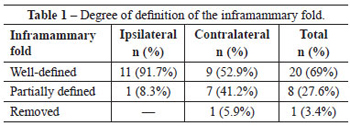
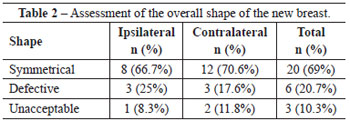
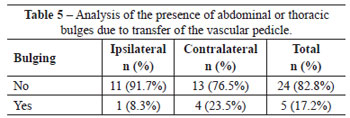
RESULTS: The average age of the patients was 43 ± 7 years. In group 1 (ipsilateral TRAM), 91.7% of the patients presented a well-defined inframammary fold, as compared to 52.9% of the patients in group 2 (contralateral TRAM). In group 1, 8.3% of patients showed xiphoid bulges, whereas they were observed in 23.5% of patients in group 2. The difference in the overall shape of the reconstructed breast was not significant; symmetry was observed in 66.7% and 70.6% of patients in groups 1 and 2, respectively.
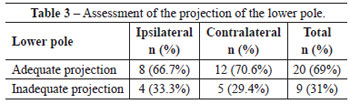
CONCLUSIONS: Ipsilateral TRAM flaps allow better preservation of the inframammary fold and cause less xiphoid bulge. However, the overall shape of the breast and the projection of its lower pole were similar between the two groups.
Keywords: Breast/surgery. Mammaplasty. Reconstructive surgical procedures. Surgical flaps. Abdominal muscles.
RESUMO
INTRODUÇÃO: A reconstrução mamária com retalho do músculo reto abdominal (TRAM, do inglês transverse rectus abdominis myocutaneous) tem se tornado um procedimento comumente realizado desde a década de 1990. O TRAM ipsilateral vem demonstrando ser tão seguro quanto o retalho contralateral na reconstrução mamária. Entretanto, estudos avaliando o resultado estético com as duas técnicas são escassos na literatura. A proposta deste estudo é comparar os resultados cosméticos entre os retalhos pediculados ipsilateral e contralateral.
MÉTODO: Foi realizada avaliação prospectiva de 29 pacientes submetidas a reconstrução imediata com TRAM ipsilateral e contralateral. Os grupos foram comparados entre si, analisando-se os resultados estéticos.
RESULTADOS: O estudo incluiu 29 pacientes, com média de idade foi 43 ± 7 anos. O grupo 1 (TRAM ipsilateral) apresentou o sulco inframamário bem definido em 91,7% dos casos, comparativamente a 52,9% no grupo 2 (TRAM contralateral). Observou-se abaulamento na região xifoide em 8,3% dos pacientes do grupo 1 e em 23,5% dos pacientes do grupo 2. A diferença na forma global da mama reconstruída não foi importante, com 66,7% e 70,6% de simetria nos grupos 1 e 2, respectivamente.
CONCLUSÕES: O TRAM ipsilateral demonstrou melhor manutenção do sulco inframamário e menor abaulamento na região xifoide. Entretanto, a forma global da mama e a projeção do polo inferior da mama foram similares entre os dois grupos.
Palavras-chave: Mama/cirurgia. Mamoplastia. Procedimentos cirúrgicos reconstrutivos. Retalhos cirúrgicos. Músculos abdominais.
The pedicled transverse rectus abdominal myocutaneous (TRAM) flap has become the gold standard procedure for autologous breast reconstruction. Anatomical and clinical studies have increased knowledge about the vascular structure of the flap and the safety of this technique. However, studies assessing the aesthetic outcomes of ipsilateral and contralateral pedicled flaps are poorly described in the literature1-3.
The original description of the procedure was based on the ipsilateral pedicled flap. However, doubts over the position and the potential vascular torsion of this flap made the contralateral TRAM flap the preferred option for many surgeons1.
Recently, studies have shown that the ipsilateral TRAM flap is as safe as the contralateral flap. Moreover, a shorter distance must be covered by flap rotation, thus requiring less dissection of the vascular pedicle and facilitating the positioning of the flap in the area of the defect. Some authors point out an additional advantage, that is the versatility of this procedure in breast reconstruction, which allows better preservation of the inframammary fold and reduces contour loss of the xiphoid appendix1,4,5.
The aim of this study was to compare the cosmetic outcomes of ipsilateral and contralateral TRAM flaps after immediate reconstruction performed at the Plastic Surgery and Reconstructive Microsurgery Service of the Walter Cantídio University Hospital (Fortaleza, CE, Brazil).
METHOD
This is a quantitative, descriptive, and prospective study, performed at the Plastic Surgery and Microsurgery Service of the Walter Cantídio University Hospital (Fortaleza, CE, Brazil).
In this study, 29 patients who underwent immediate breast reconstruction with ipsilateral or contralateral TRAM flaps between 2009 and 2011 were evaluated.
Information such as age, comorbidities, surgical procedure, adjuvant treatment, complication rate, and qualitative assessment (performed out by the same investigator) of the aesthetic postoperative outcomes was collected and recorded on forms.
The data were analyzed using the Statistical Package for the Social Sciences (SPSS) program, version 16.0.
Surgical Procedure
Before the operation, the patients were asked to lie down in an orthostatic position and were marked to define the inframammary fold and the previous midclavicular and axillary lines. An abdominal and tension-free ellipse was designed; this ellipse was large enough to cover the defect.
Inferior epigastric vessels were visualized and clamped. The flap was lifted from the lateral to the medial portion, over the edge of the rectus abdominis muscle. The umbilical scar was preserved until the costal margin.
A central incision connecting the abdomen and the postmastectomy defect was made, preserving the inframammary fold and the vascularization of the mastectomized skin. To avoid pedicle rotation, the right ipsilateral flap was rotated clockwise and on the left side, the opposite movement was performed during flap transfer. The flap was de-epithelized and the excess tissue discarded. The abdominal wall was reconstructed using a Marlex mesh and two suction drains were placed in the breast and abdomen, respectively.
RESULTS
We evaluated 29 patients (average age 43 ± 7 years; range, 30-60 years) who underwent immediate breast reconstruction with TRAM flaps.
With respect to the pedicle used for breast reconstruction, the surgical procedures were divided into two groups: group 1 (ipsilateral TRAM) and group 2 (contralateral TRAM). Patients undergoing surgeries in which ipsilateral and contralateral pedicles were used corresponded to 41.4% and 58.6% of the total population, respectively.
The body mass index (BMI) of patients belonging respectively to groups 1 and 2 was as follows: obese, 33.3% and 29.4%; overweight, 33.3% and 41.2%; and normal weight, 33.4% and 29.4%. No smokers or patients with significant comorbidities were found in the two groups. A higher number of patients underwent axillary dissection in group 2 as compared to group 1 (94.1% vs. 66.7%, respectively).
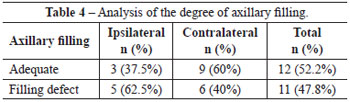
Variables such as the definition of the inframammary fold, the overall shape of the new breast, the projection of the lower pole, the degree of axillary filling, and the presence of abdominal or thoracic bulges occurring upon transfer of the vascular pedicle were compared between the two groups in order to qualitatively evaluate the aesthetic outcomes (Tables 1 to 5). Patients who did not undergo axillary dissection were excluded from the evaluation of axillary filling to reduce bias in comparison of the groups.
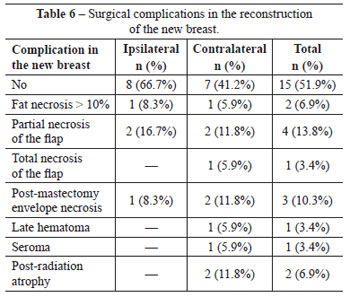
Surgical complications associated with breast reconstruction are described for the two groups in Table 6. No systemic complications such as deep vein thrombosis, embolism, infection, or blood volume loss requiring blood transfusion were observed in these procedures. One patient belonging to group 1 developed abdominal seroma and another patient in group 2 presented with postoperative umbilical stenosis.
Figures 1 to 6 illustrate some cases of this series.

Figure 1 - Postoperative aspect of a patient who underwent breast reconstruction with ipsilateral TRAM flap. A satisfactory aesthetic result was observed, with a well-defined inframammary fold.

Figure 2 - Postoperative aspect of a patient who underwent breast reconstruction with ipsilateral TRAM flap. A satisfactory aesthetic result was observed, with proper symmetry of the reconstructed breast as compared to the contralateral breast.

Figure 3 - Postoperative aspect of a patient who underwent breast reconstruction with contralateral TRAM flap. A satisfactory aesthetic result was observed, with a well-defined inframammary fold, although inappropriate axillary filling was found.

Figure 4 - Postoperative aspect of a patient who underwent breast reconstruction with contralateral TRAM flap. A satisfactory aesthetic result was observed, with removal of the medial inframammary fold.

Figure 5 - Postoperative aspect of a patient who underwent breast reconstruction with contralateral TRAM flap. A satisfactory aesthetic result was observed, with delimited inframammary fold.

Figure 6 - Postoperative aspect of a patient who underwent breast reconstruction with contralateral TRAM flap. A symmetrical result was observed, with bilateral removal of the inframammary fold in the medial region and axillary filling defect.
DISCUSSION
Since the original description reported by Hartrampf et al.6 in 1982, breast reconstruction with TRAM flaps has become an increasingly common procedure for immediate breast reconstruction, because it confers satisfactory tissue volume and similar consistency to the contralateral breast. The versatility of the positioning and remodeling of this flap in the creation of a new breast provides aesthetic outcomes comparable to other procedures available for breast reconstruction. However, the improvement of reconstructive techniques does not develop as fast as the increasing demand from patients for better cosmetic outcomes. This renders the creation of a new breast with autologous flaps difficult and can lead to poor definition of the inframammary fold, inadequate axillary filling after draining of the lymph node, and asymmetric projection of the lower pole as compared to the contralateral breast1,5,7,8.
The ipsilateral TRAM flap has the inherent advantage of providing increased pedicle length, because a shorter distance is required for flap transposition in the ipsilateral TRAM flap as compared to the contralateral TRAM flap. Lower tension on the pedicle reduces venous resistance and improves flap perfusion. Moreover, it diminishes the necessity for extensive flap dissection or costal cartilage removal, maneuvers that can be used with the contralateral TRAM flap to reduce tension1-4.
In patients with a short torso (a short abdomen and abdominal rectus muscle), the ipsilateral TRAM flap was inserted free of tension. Patients with lower abdominal scarring required a larger skin area, which implied a relatively short pedicle. In the presence of an inferior median scar, the creation of an ipsilateral TRAM flap is ideal and maximizes the use of the hemiabdomen1.
However, in cases of ptotic breasts, contralateral TRAM flaps in a vertical position were preferred to better fill the lower pole. Ozkan et al.4 also reported using this technique in small breasts1.
The literature highlights an additional advantage of ipsilateral TRAM flaps regarding the definition of the medial inframammary fold and the reduction of sternal bulges caused by muscular repositioning after flap transfer1-4. In this study, most of the patients presented a well-defined inframammary fold. Patients belonging to group 1 showed better results, as compared to patients in group 2, with respect to inframammary fold definition and the absence of bulges; this observation was is in agreement with the literature. Although ipsilateral pedicled TRAM flaps showed the above-mentioned advantages, no significant difference was observed between the two groups with respect to the overall shape of the new breast and the projection of the lower pole.
In this study, assessment of the degree of axillary filling was constrained by the differences observed in patients who underwent different levels of axillary dissection and by the reduced cohort size upon exclusion of patients who did not undergo axillary dissection.
CONCLUSIONS
In conclusion, ipsilateral pedicled TRAM flaps confer higher definition of the inframammary fold and reduce xiphoid bulges occurring upon flap transfer in the sternal region. However, the overall shape of the breast and the projection of its lower pole were similar in the two groups.
REFERENCES
1. Tan BK, Joethy J, Ong YS, Ho GH, Pribaz JJ. Preferred use of the ipsilateral pedicled TRAM flap for immediate breast reconstruction: an illustrated approach. Aesthetic Plast Surg. 2011;36(1):128-33.
2. Clugston PA, Gingrass MK, Azurin D, Fisher J, Maxwell GP. Ipsilateral pedicled TRAM flaps: the safer alternative? Plast Reconstr Surg. 2000;105(1):77-82.
3. Omranipour R, Lebaschi AH, Mohagheghi MA, Arab-Kheradmand A, Abasahl A. Outcomes of breast reconstruction with pedicled transverse rectus abdominis myocutaneous (TRAM) flap at Cancer Institute: a retrospective study of 10 years of experience. Acta Med Iranica. 2008;46(3):218-24.
4. Ozkan A, Cizmeci O, Aydin H, Ozden BC, Tümerdem B, Emekli U, et al. The use of the ipsilateral versus contralateral pedicle and vertical versus horizontal flap inset models in TRAM flap breast reconstruction: the aesthetic outcome. Aesthetic Plast Surg. 2002;26(6):451-6.
5. Janiga TA, Atisha DM, Lytle IF, Wilkins EG, Alderman AK. Ipsilateral pedicle TRAM flaps for breast reconstruction: are they as safe as contralateral techniques? J Plast Reconstr Aesthet Surg. 2010;63(2):322-6.
6. Hartrampf CR, Scheflan M, Black PW. Breast reconstruction with a transverse abdominal island flap. Plast Reconstr Surg. 1982;69(2):216-25.
7. Gomes AAR, Pessoa SGP. Retalho TRAM com dissecção mínima para reconstrução mamária. Rev Bras Cir Plást. 2010;25(4):652-6.
8. Fayman MS, Potgieter E, Becker PJ. The pedicle tram flap: a focus on improved aesthetic outcome. Aesthetic Plast Surg. 2006;30(3):301-8.
1. Aspiring member in training of the Sociedade Brasileira de Cirurgia Plástica (Brazilian Society for Plastic Surgery) - SBCP, resident physician at the Plastic Surgery and Reconstructive Microsurgery Service of the Walter Cantídio University Hospital, Fortaleza, CE, Brazil.
2. Specialist member of the SBCP, plastic surgeon at the Plastic Surgery and Reconstructive Microsurgery Service of the Walter Cantídio University Hospital, Fortaleza, CE, Brazil.
3. Full member of the SBCP, preceptor of the Plastic Surgery and Reconstructive Microsurgery Service of the Walter Cantídio University Hospital, Fortaleza, CE, Brazil.
4. Full member of the SBCP, regent of the Plastic Surgery and Reconstructive Microsurgery Service of the Walter Cantídio University Hospital, Fortaleza, CE, Brazil.
Correspondence to:
Juliana Régia Furtado Matos
Rua Mombaça, 164 - Aldeota
Fortaleza, CE, Brazil - CEP 60160-190
E-mail: julianarfm@gmail.com
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: January 12, 2012
Article accepted: April 4, 2012
This study was performed in the Walter Cantídio University Hospital, Fortaleza, CE, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket