



Original Article - Year 2012 - Volume 27 -
Oblique thighplasty in patients after massive weight loss
Coxoplastia oblíqua em pacientes após grandes perdas ponderais
ABSTRACT
BACKGROUND: Trophic skin alterations that occur during aging are observed more often in the thighs and arms than in other body regions. Patients experiencing substantial weight loss after bariatric surgery exhibit more evident problems, including unsightly appearance, discomfort, difficulty walking, and hygiene problems. The present surgical approach aims to reverse these effects by means of resection of the cutaneous excess.
METHODS: Thirty patients who previously underwent bariatric surgery and experienced substantial weight loss were selected. All patients also underwent abdominoplasty with or without brachioplasty simultaneously or at different times. The cutaneous resection was oriented along an oblique and sinuous line along the anterior face of the thighs in the projection of the sartorius muscle route. All patients were monitored for a minimum period of 6 months postoperatively.
RESULTS: The surgery significantly improved the internal contours of the thighs, improving the patients' quality of life. Four patients had small suture dehiscences, and 2 had lymphocele. No hematomas, infection, or distortions in the external genitalia were observed.
CONCLUSIONS: The oblique resection of cutaneous excesses was applied specifically in patients who experienced substantial weight loss after bariatric surgery. This technique significantly decreased the volume of each thigh and readjusted contours without increasing morbidity.
Keywords: Bariatric surgery. Weight loss. Plastic surgery. Thigh/surgery.
RESUMO
INTRODUÇÃO: As alterações tróficas da pele com o avançar da idade são observadas com maior frequência nas coxas e nos braços, quando comparadas às demais regiões do corpo. Nos pacientes com grandes perdas ponderais após cirurgia bariátrica, as consequências são muito mais evidentes, com aspectos pouco estéticos, combinados a desconforto, dificuldade de deambulação e problemas de higiene. A proposta cirúrgica visa a reverter esses efeitos mediante a ressecção dos excessos cutâneos.
MÉTODO: Foram selecionados 30 pacientes previamente submetidos a cirurgia bariátrica, com grandes perdas de peso. Todos os pacientes foram também submetidos a abdominoplastia e/ou abdominoplastia combinada com braquioplastia, no mesmo tempo ou em tempos operatórios diversos. A orientação da ressecção cutânea realizada determinou uma linha oblíqua e sinuosa ao longo da face anterior das coxas, na projeção do trajeto do músculo sartório. Todos os pacientes foram seguidos pelo período mínimo de 6 meses de pós-operatório.
RESULTADOS: A cirurgia possibilitou significativa melhora do contorno interno das coxas, assim como da qualidade de vida dos pacientes. Entre os pacientes avaliados, 4 apresentaram pequenas deiscências de sutura e 2, linfocele. Não foram observados hematoma, infecção ou distorções na genitália externa.
CONCLUSÕES: A ressecção oblíqua dos excessos cutâneos tem sido aplicada especificamente em pacientes que apresentaram grandes perdas de peso após cirurgia bariátrica. A técnica possibilitou redução significativa do volume de cada coxa, com readequação do contorno, sem aumentar a morbidade.
Palavras-chave: Cirurgia bariátrica. Perda de peso. Cirurgia plástica. Coxas/cirurgia.
The thigh is one of the regions of the body that undergoes large cutaneous alterations after substantial weight loss due to the presence of fat deposits of different textures and volumes; variation in the position of the scar after the surgery in the short, medium, and long terms; and risk factors inherent to the surgery itself1,2.
Aesthetic plastic surgery for the thighs was first described about 55 years ago and has been undergoing continuous tactical and technical revisions aimed at improving results3,4. However, this procedure has had limited reception by surgeons and patients due to secondary problems, including scar enlargement, caudal displacement of the inguinal crease, deformities of the external genitalia, and poor quality results5. Better aesthetic results were achieved in the long term with a lower incidence of complications only after the suspension and anchoring of the superficial fascia in cases of moderate sagging and adiposity due to the natural sagging associated with aging6,7. With the continuous increase in the number of former morbidly obese patients who have received bariatric surgery, the large volumes of adipose skin and tissues to be resected demand new procedures that involve circumferential resections in the hip and thighs to improve the patients' quality of life8-12.
Oblique resection along the cutaneous projection of the sartorius muscle is the most indicated technique for patients with large volumes of skin associated with sagging and adiposity around the entire length of the thighs and in the anterior and internal faces due to the muscle's more stable position postoperatively in the medium and long terms. Although largely evident, patients tolerate the resultant scars because of the improvement in their quality of life13 and the associated minimal complications.
METHODS
From May 2003 to December 2010, 30 patients with excessive weight loss underwent thighplasty by means of oblique anterior transverse cutaneous resection. Twenty-three patients were female, and 7 were male. The patients' ages at the time of surgery ranged from 26 to 69 years.
All patients previously underwent bariatric surgery. The average weight after weight loss was 110 kg and 92.5 kg at thighplasty (range, 65 to 129 kg).
Patients had significant volumes of sagging fat and skin mostly at the medial third and anterior internal regions of the thighs.
In addition to the routine preoperative examinations, all patients underwent vascular assessment; none of them had any type of circulatory problem postoperatively.
Preoperative delineations
Patients were marked in a standing position with abducted legs 24 hours before the surgery.
A line was drawn in the cutaneous projection of the sartorius muscle, followed by bi-digital clamping of the excess skin to be resected. The area acquired the shape of a wide fuse with the upper limit in the proximity of the anterior superior iliac spine and variable inferior extremity up to the internal tuberosity of the tibia, according to the volume of skin to be resected (Figure 1).

Figure 1 - Bi-manual maneuver for assessing the cutaneous excesses to be resected in a single block. The larger axis of resection follows the projection line of the sartorius muscle.
Surgical technique
All patients were operated on in the horizontal supine position under epidural or general anesthesia with endotracheal intubation and prophylactic compression of the lower limbs.
The resections were standardized in a single block using an electrocautery device in the entire area of the previous delineation until the suprafascial plane without any extra cutaneous dissection beyond the incised edges. Suturing was performed with isolated sutures using absorbable thread in 3 planes: 2-0 polydioxanone (PDS), 3-0 Monocryl, and 4-0 Monocryl in the subcutaneous cellular tissue, dermal, and intracuticular planes, respectively.
Neither drains nor local infiltration with epinephrine was used. The operation time ranged from 1 to 2 hours.
In the same surgery, all patients underwent abdominoplasty; abdominoplasty was combined with brachioplasty in 2 patients.
Postoperative care
At the end of the surgery, the suture lines were covered with porous adhesive tape and the patients wore elastic stockings of moderate compression up to the upper half of the legs.
The patients begun to walk and were discharged after 24 hours with instructions for bathing without the need to replace the dressings.
Antibiotic therapy, usually first-generation cephalosporin, was applied over 7 days, and non-steroid analgesics were prescribed as needed.
Inpatient returns were scheduled every 7 days during the first 3 weeks. In the absence of complications, the patients were authorized to perform activities that did not require substantial effort.
All patients were monitored for a minimum of 6 months postoperatively.
RESULTS
The surgery significantly improved the internal contour of the thighs, improving the quality of life of all patients.
Four cases of small suture dehiscences and 2 cases of lymphocele in the distal third of the medial face of the thighs were observed; all were resolved within 3 weeks by means of aspiration, compression, and antibiotic therapy. These complications were attributed to deeper cutaneous dissection close to the internal face of the knee at which the lymphatic plexus is more superficial. The experience gained in dealing with these complications motivated the implementation of more superficial cutaneous resection in subsequent cases.
No hematomas, infection, or distortions in the external genitalia were observed.
Figures 2 to 6 show images of selected patients that were operated on.

Figure 2 - Cutaneous resection in a single block that reaches the aponeurotic plane without dissection of the incision edges.

Figure 3 - Appearance of the suture lines performed in 3 planes, positioned away from the external genitalia over the cutaneous projection of the sartorius muscle from the external third of the inguinal line to the internal face of the knee. Transoperative period of "fleur-de-lis"-type abdominoplasty during the same surgery.

Figure 4 - In A, anterior view of a 45-year-old formerly morbidly obese patient after losing 140 kg after bariatric surgery. The patient weighed 90 kg before surgery with a large abdominal cutaneous apron. In B, delineations on the thighs for the resection of cutaneous excess according using the "smooth S" described for the technique. In C, 2 years postoperatively without distortion of the external genitalia. Further breast reduction and abdominoplasty complemented the corporoplasty. In D and E, lateral view of the thighs in the pre- and postoperative periods, respectively.

Figure 5 - In A, anterior view of a 69-year-old patient after losing 94 kg due to bariatric surgery who underwent thighplasty according to the proposed technique combined with abdominoplasty; she weighed 88 kg at the time of surgery. In B, 18 months postoperatively without changes in the scar positions. In C and D, lateral view of the thighs in the pre- and postoperative periods, respectively; clear improvement in the internal contour of the thighs and scars ending below the internal tuberosity of the knee for resection of cutaneous excess.
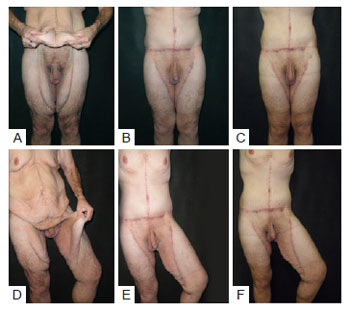
Figure 6 - In A, B, and C, a male patient who lost 96 kg after bariatric surgery. The patient weighed 94 kg and underwent thighplasty and abdominoplasty simultaneously. Anterior views in the preoperative period, and 6 and 13 months postoperatively. In D, E, and F, lateral view in the preoperative period, and 6 and 13 months postoperatively.
DISCUSSION
The anatomical preservation of the superior internal triangular area of the thigh close to the groin is very important and should not undergo surgical intervention13,14. Another detail is the nonexistence of dead space, which is very frequently encountered in body contour surgeries and causes seroma15-18.
In all operated cases, the en bloc resection of cutaneous/adipose excesses without resecting edges was performed easily with little trauma in the surrounding regions. This consequently reduced edema, decreased the risk of tension in the suture, and minimized the incidence of dehiscences19-21.
It is also important to consider that aged patients with only sagging problems should be treated and considered differently from those with substantial weight loss22-24. In these patients, resections, including transverse fusions along the inguinal crease, vertical fusiform resection along the thigh internal face, and even L-shaped resections, have limitations and aesthetic imperfections despite the suturing of the superficial fascia in the Colles' fascia25. The most frequent aesthetic imperfections are enlargement of the suture line, migration of the scar position due to caudal traction, and external genitalia dysmorphia in female patients. In addition, some results are unsatisfactory due to the limited resection volume.
Although L-shaped resection provides good aesthetic results26, positioning the scar at the inguinal region and external face of the thigh can be associated with secondary problems such as suture dehiscence, caudal displacement of the inguinal scar, vulva distortion, and lymphatic vessels lesion.
Although more evident in the superior and medial thirds of the anterior face of the thigh, the scar is accepted and tolerated by post-bariatric patients because it does not have late enlargement or migrate from its initial position; moreover, it results in improved contour of the thighs and fast postoperative recovery and does not distort the external genitalia in the long term.
CONCLUSIONS
Oblique thighplasty is specifically indicated for patients who experience substantial weight loss after bariatric surgery with substantial skin sagging with or without adipose tissue.
This technique creates a scar along the whole cutaneous projection of the sartorius muscle, which can be elongated up to the internal superior third of the leg, maintaining the anatomic integrity of the superior internal region of the thighs. The resection is performed in a single block without leaving dead space. The scar neither detaches from its initial position nor enlarges significantly, avoiding the need for further retouching. This procedure improves the contour of the thighs and does not cause secondary distortions in the external genitalia of female patients. The anterior and transverse position of the scar in the thighs is accepted by these types of patients.
REFERENCES
1. hermak MA, Mallalieu J, Chang D. Does thighplasty for upper thigh laxity after massive weight loss require a vertical incision? Aesthet Surg J. 2009;29(6):513-22.
2. Lockwood T. Lower body lift with superficial fascial system suspension. Plast Reconstr Surg. 1993;92(6):1112-25.
3. Schultz RC, Feinberg LA. Medial thigh lift. Ann Plast Surg. 1979;2(5):404-10.
4. Lewis Jr JR. The thigh lift. J Int Coll Surg. 1957;27(3):330-4.
5. Planas J. The "crural meloplasty" for lifting of the thighs. Clin Plast Surg. 1975;2:495-503.
6. Lockwood TE. Fascial anchoring technique in medial thigh lifts. Plast Reconstr Surg. 1988;82(2):299-304.
7. Colles A. A treatise on surgical anatomy: anatomy of the perineum. Dublin: Gilbert and Hodges; 1811.
8. Baroudi R, Moraes M. Philosophy, technical principles, selection, and indication in body contouring surgery. Aesthetic Plast Surg. 1991;15(1):1-18.
9. Lockwood TE. Lower-body lift. Aesthet Surg J. 2001;21(4):355-70.
10. Lockwood TE. Maximizing aesthetics in lateral-tension abdominoplasty and body lifts. Clin Plast Surg. 2004;31(4):523-37.
11. Hurwitz DJ, Zewert T. Body contouring surgery in the bariatric surgical patient. Oper Tech Plast Reconstr Surg. 2002;8:87-95.
12. Hurwitz DJ. Single-staged total body lift after massive weight loss. Ann Plast Surg. 2004;52(5):435-41.
13. Kenkel JM, Eaves FF 3rd. Medial thigh lift. Plast Reconstr Surg. 2008;122(2):621-2.
14. Leitner DW, Sherwood RC. Inguinal lymphocele as a complication of thighplasty. Plast Reconstr Surg. 1983;72(6):878-81.
15. Aly AS, Cram AE, Chao M, Pang J, McKeon M. Belt lipectomy for circumferential truncal excess: the University of Iowa experience. Plast Reconstr Surg. 2003;111(1):398-413.
16. Nemerofsky RB, Oliak DA, Capella JF. Body lift: an account of 200 consecutive cases in the massive weight loss patient. Plast Reconstr Surg. 2006;117(2):414-30.
17. Shermak MA, Chang D, Magnuson TH, Schweitzer MA. An outcomes analysis of patients undergoing body contouring surgery after massive weight loss. Plast Reconstr Surg. 2006;118(4):1026-31.
18. Taylor J, Shermak M. Body contouring following massive weight loss. Obst Surg. 2004;14(8):1080-5.
19. Arthus ZM, Cuadrado D, Sohn V, Wolcott K, Lesperance K, Carter P, et al. Post-bariatric panniculectomy: pre-panniculectomy body mass index impacts the complication profile. Am J Surg. 2007;193(5):567-70.
20. Kim J, Stevenson TR. Abdominoplasty, liposuction of the flanks, and obesity: analyzing risk factors for seroma formation. Plast Reconstr Surg. 2006;117(3):773-81.
21. Kuroi K, Shimozuma K, Taguchi T, Imai H, Yamashiro H, Ohsumi S, et al. Evidence-based risk factors for seroma formation in breast surgery. Jpn J Clin Oncol. 2006;36(4):197-206.
22. Lockwood TE. Superficial fascial system (SFS) of the trunk and extremities: a new concept. Plast Reconstr Surg. 1991;87(6):1009-18.
23. Illouz YG, De Villers. Body sculpturing by lipoplasty. New York: Churchill Livingstone; 1989.
24. Lewis Jr JR. Correction of ptosis of the thighs: the thigh lift. Plast Reconstr Surg. 1966;37(6):494-8.
25. Mathes DW, Kenkel JM. Current concepts in medial thighplasty. Clin Plast Surg. 2008;35(1):151-63.
26. Hurwitz DJ. Medial thighplasty. Aesthet Surg J. 2005;25(2):180-91.
1. Full member of the Sociedade Brasileira de Cirurgia Plástica (Brazilian Society of Plastic Surgery) - SBCP, full member of the Colégio Brasileiro de Cirurgiões (Brazilian Association of Surgeons), full member of the International Society of Aesthetic Plastic Surgery (ISAPS), head of the Plastic Surgery Department of Hospital Geral de Andaraí, Rio de Janeiro, RJ, Brazil.
2. Associate member of the SBCP, plastic surgeon at the Plastic Surgery Department of Hospital Geral de Andaraí, Rio de Janeiro, RJ, Brazil.
3. Resident physician of the General Surgery Department of Hospital Federal Bonsucesso, Rio de Janeiro, RJ, Brazil.
Carlos Del Pino Roxo
Av. Ayrton Senna, 1850 - sala 352 - Barra da Tijuca
Rio de Janeiro, RJ, Brazil - CEP 22631-390
E-mail: drcroxo@rjnet.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: January 17, 2012
Article accepted: March 11, 2012
Study conducted at the Plastic Surgery Department of Hospital Geral de Andaraí, Rio de Janeiro, RJ, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket