INTRODUCTION
Advances in optical magnification techniques have allowed surgeons to approach smaller
structures, creating a huge range of possibilities for different specialties. This
set of procedures aided by optical magnification is known as microsurgery1.
Soon after the dissemination of the techniques, it was realized that a properly trained
surgeon2 was a fundamental component. Thus, the first training laboratories soon appeared,
Brazil being a pioneer in South America, in 19713.
The training sequence varies a little between the various current centers and generally
starts with familiarization with the microscope and other materials, followed by learning
variations of microsurgical sutures, with simple materials such as latex gloves4, until evolving to vascular anastomoses in non-living and living models, when available5.
The training aims to develop the professional skills of the surgeon, to prepare and
provide security during his clinical activities; excellent results are anticipated
in vascular anastomoses patency, since the primary services report flap survival rates
above 90%6,7.
Non-biological models avoid ethical conflicts related to the use of animals, in addition
to the fact that some are accessible, such as tubes made of synthetic materials, and
others allow a more accurate assessment of skills, particularly virtual ones; however,
animal models are more consistent and closer to the reality found in clinical practice8-10.
One of the techniques necessary for training in microsurgery is vascular anastomosis.
Some fundamental rules of vascular anastomoses should be followed, which include well-vascularized
proximal and distal margins, free of active disease and tension. The anastomosis also
should be hemostatic, circumferentially air-tight, and have inverted edges11.
Thrombosis being one of the main obstacles to the success of vascular flow, specific
animal models have been developed to assess the impact of endothelial damage on thrombosis
formation 12, demonstrating how aggression to the intimal layer can evolve into this complication
and how external applications of different forces can cause similar consequences 13. Even though the concept of compression anastomosis has been investigated for nearly
two centuries, it has not yet achieved widespread acceptance, but it could be a way
of reducing the risk of thrombosis11.
It is known that after arterial thrombosis of the anastomosis, the flap may survive
with only conservative therapy when the event occurs after a minimal critical period.
This time is most likely to occur after the 12th postoperative day, but this minimum
critical period may be as low as 6 days for arterial occlusion14. Thus, it is essential to comprehend and develop ways to avoid thrombosis, when feasible,
and treat it, when necessary, for successfully performing complex microsurgical flaps.
OBJECTIVE
This study primarily aimed to evaluate the impact of immediate intermittent compression
on microsurgical arterial anastomoses and their patency in an experimental model.
The secondary objective was to evaluate the impact of gentle fixed compression immediately
after vascular clamp removal.
METHODS
During experimental training, 12 Wistar rats (male sex; age, 60-90 days) were selected
for sectioning and anastomoses of the two femoral arteries, to assess the impact of
immediate intermittent compression on microsurgical arterial anastomoses. All animals
received bilateral anastomosis by the same method.
The study was carried out between April and July 2021 and the CEP approval number
is 1378/2021.
The 24 arterial anastomoses were randomly divided into three groups, as described
below. A draw was performed immediately before the anesthesia of the rats, and a paper
written with the technique to be performed on each rat was removed from the bag.
Group 1 (G1) - Intermittent Compression for 60 s Group 2 (G2) - Fixed Compression
for 60 s Group 3 (G3) - Control (observation only)
In Group 1, immediately after microsurgical anastomosis, 60 gentle intermittent compressions
were performed, such as massage, for 60 seconds (Figure 1). In Group 2, the same gentle compression was applied constantly, for 60 seconds.
In Group 3, anastomosis was only observed without any intervention. The measurement
of the diameter of the vessels was performed with a millimeter ruler under a microscopic
view with a 10x magnification before the procedure.
Figure 1 - Intermittent compression applied over the newly performed arterial anastomosis.
Figure 1 - Intermittent compression applied over the newly performed arterial anastomosis.
Schedule
The study was divided into two intervention periods. The first period involved a random
division of the femoral arteries to separate the groups and perform the initial surgery.
In the second period, after 7 days, the final patency of the anastomosis was checked.
Initial data included weight, vessel diameter at the section point, surgical time
for end-to-end arterial anastomosis, and the number of sutures. The final data included
weight and patency assessments after 7 days.
Anesthesia
We opted for combined anesthesia using 10% ketamine hydrochloride (Cetamin®, Syntec, Brazil) and 2% xylazine hydrochloride (Xilazin®, Syntec, Brazil) intraperitoneally, at doses of 80 and 10 mg/kg, respectively, associated
with lidocaine (Xylestesin®, Cristália, Brazil) for application at the incision sites at a dose of 7 mg/kg. For
intra-and postoperative analgesia, tramadol (Tramadon®, Cristália, Brazil) and dipyrone (Febrax®, Lema-Injex Biologic, Brazil) were subcutaneously administered at doses of 5 mg/kg
and 100 mg/kg, respectively. Dipyrone was reapplied daily for pain control until the
second procedure and subsequent euthanasia of the animal with thiopental (Thiopentax®, Cristália, Brazil), at a dose of 120 mg/kg, on the seventh day.
Surgery
After initial weighing and trichotomy of the bilateral inguinal region, an oblique
incision was made in the inguinal region of the rat, with opening and dissection by
plane until the identification of the femoral vessels. The femoral artery was dissected
and isolated at its most proximal and largest caliber, with a blue ribbon under it
for better contrast. At this point, the adventitial layer was removed, and the diameter
of the artery was measured at the point where it was sectioned. Before the section,
the double metallic clamp was positioned proximally and distally to this point. An
interrupted suturing was initiated using 10-0 mono nylon, with 3/8 and 0.65 cm cylindrical
needles to perform the anastomosis. After the end-to-end suture was timed and the
number of sutures was counted, immediately after clamp removal, one of the three proposals
was performed, according to the group chosen for the artery. We allowed 30 min to
check the patency, as described below and then proceeded to the approximation of the
muscle, subcutaneous tissue, and skin of the rat using 5-0 mono nylon simple sutures.
After 7 days, the rats were anesthetized again. After weight measurement, the vascular
suture was reexplored, and patency was checked.
Patency test
Patency was always verified by an independent examiner.
Patency at 30 min and 72 h was verified using the technique proposed by Acland13. Two forceps were placed distally to the anastomosis, and a maneuver was performed
to empty the central region at both sites. Subsequently, the proximal forceps were
released to refill the central space. If the created intravascular space was immediately
filled with blood proximal to the distal direction, we considered the patency (flow)
to be successful.
Vessel staining and pulsation were considered indirect signs of successful patency
(flow).
The absence of flow after 30 min or 7 days was considered an anastomosis failure.
The limitation of this test is that although it is useful to verify the technique,
it does not consider the blood flow.
Statistical analysis
The data were tabulated using Microsoft Excel software. Profile analysis was used
to determine the initial and final weights (Table 1).
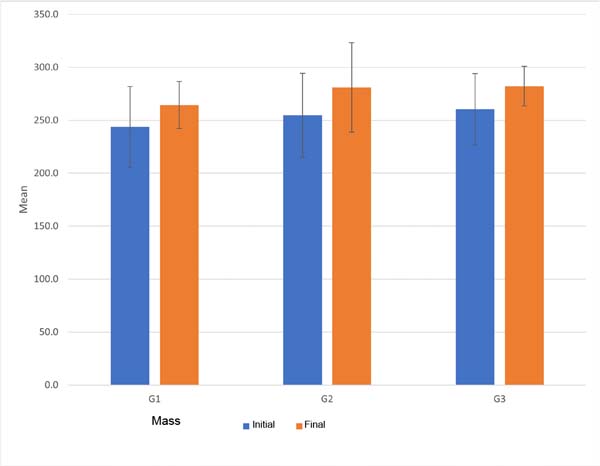
Table 1 - Mean and standard deviation for mass according to the moment.
| Mass (g) |
|
Initial |
Final |
| G1 |
243.8 |
264.4 |
| 38.2 |
22.2 |
| G2 |
254.6 |
281.0 |
| 39.5 |
42.2 |
| G3 |
260.4 |
282.1 |
| 33.5 |
18.7 |
Table 1 - Mean and standard deviation for mass according to the moment.
Analysis of variance was used for other quantitative variables (Table 2).
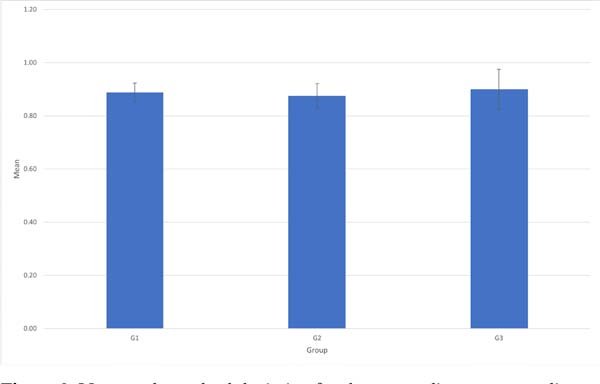
Table 2 - Mean and standard deviation for variables according to the group.
| Variables |
|
Artery diameter
(mm) |
Number of sutures |
Time (min) |
| G1 |
0.89 |
6.5 |
25.6 |
| 0.04 |
1.4 |
2.0 |
| G2 |
0.88 |
7.0 |
24.5 |
| 0.05 |
0.8 |
3.7 |
| G3 |
0.90 |
6.0 |
24.5 |
| 0.08 |
1.1 |
3.9 |
| p |
0.67 |
0.22 |
0.74 |
Table 2 - Mean and standard deviation for variables according to the group.
For patencies in the initial and final moments, the McNemar test was used (Table 3).
Table 3 - Absolute and relative frequency of initial and final patency according to the group.
| Patency |
|
Initial |
Final |
p |
| G1 |
8 |
5 |
0.07 |
| 100.0 |
62.5 |
| G2 |
8 |
2 |
0.48 |
| 100.0 |
25.0 |
| G3 |
8 |
4 |
0.23 |
| 100.0 |
50.0 |
| Total |
24
100.0
|
11
45.8
|
|
Table 3 - Absolute and relative frequency of initial and final patency according to the group.
Experimental Laboratory
All activities were performed in an experimental laboratory at the University of Medicine
of Botucatu, where bioterium, basic microsurgical material (Microsuture®), and microscopes (DFV®) with magnification up to 40 times are available.
Animals were kept in different cages, with water and food ad libitum, an air exhaust
system, 12 h of light/dark cycles, and temperature control, in addition to materials
for environmental enrichment.
At the end of the procedure, the rats were sacrificed, and respective carcasses were
kept frozen at -20 °C until further use for experimental training. When necessary,
the carcasses were incinerated.
Animal Use Ethics Commission (AUEC)
This research was conducted according to the rules of the AUEC of the University of
Medicine of Botucatu and was approved by the same under registration number 1378/2020.
RESULTS
Twenty-four anastomoses were performed in the 12 rats included in the study, which
were divided into three groups, with 8 vascular anastomoses in each group. Initially,
the weight of the animals was evaluated before performing the procedure and, after
the surgery, the rats showed weight gain in all three groups (p < 0.001), as can be seen in Figure 2. The average of the individual weight values of the rats in each group can be seen
in Table 1, however, there was no statistically significant difference in weight when comparing
the three groups (p= 0.53), nor when comparing weights before and after the procedure (p= 0.84).
Figure 2 - Mean and standard deviation for mass according to the moment.
Figure 2 - Mean and standard deviation for mass according to the moment.
Another quantitative variable evaluated before the procedure was the measurement of
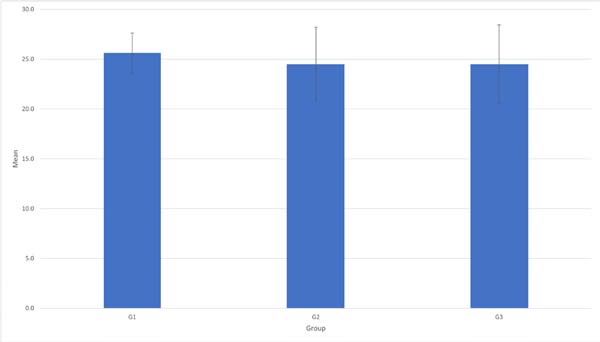
the diameter of the artery to be anastomosed, as can be seen in Figure 3 (p= 0.67), and the number of sutures performed in each group, as can be seen in Figure 4 (p= 0.22). There was no statistical significance (p>0.05) in terms of the frequency of patency according to the group. The mean operative
time was also considered in each group, being slightly greater than 25 minutes in
Group 1, which can be seen in Figure 5 (p= 0.74).
Figure 3 - Mean and standard deviation for the artery diameter according to the group.
Figure 3 - Mean and standard deviation for the artery diameter according to the group.
Figure 4 - Mean and standard deviation for time according to the group.
Figure 4 - Mean and standard deviation for time according to the group.
Figure 5 - Mean and standard deviation for time according to the group.
Figure 5 - Mean and standard deviation for time according to the group.
Regarding the patency rate, it was observed that in all groups there was a patency
rate of 100% immediately after the anastomosis, but after 7 days the patency rate
was 62.5% (p=0.07), 25% (p =0.48), and 50% (p=0.13) in Groups 1, 2, and 3 respectively. Consequently, the thrombosis rate was 37.5%,
75% and 50% in groups 1, 2, and 3, respectively, highlighting that in Group 2 there
was a higher rate of thrombosis in relation to the other groups with statistically
significant difference (p< 0.05).
DISCUSSION
The practical application of microsurgery in specialized services involves a triad
of fundamental conditions: professional training, appropriate instruments, and hospital
support3. Through a literature review, it was not possible to identify any studies that applied
any tactic similar to our research, although several studies discussed factors that
would be important to prevent or treat arterial thrombosis.
It might be complex to predict which anastomosis might be damaged by thrombosis. In
humans, it is crucial to consider the patient’s clinical condition; however, this
is more complex in animal models without specific or genetically programmed alterations.
The usefulness of ultrasonography by flow measurement has already been demonstrated;
however, the procedure is not viable in common laboratories15.
Irrigation with heparin solution has already proven to be useful in the prevention;
however, it has not been described as capable of causing thrombolysis13. Some studies have attempted to define a balanced concentration of this solution
16 and have estimated that 100 U/mL is superior to 250 U/mL. The dose used in our experience
was 150 U/mL and we considered it safe, as we did not observe any abnormal bleeding.
Heparin, as well as its derivatives, including Dalteparin (a low molecular weight
form of heparin), which does not increase the risk of surgical bleeding, are known
to be an effective microsurgical anastomoses approach17.
Lidocaine has a special effect on the treatment of vasospasms, with a rapid onset
of action, but of short duration18. The 2% lidocaine applied in our study had a satisfactory arterial dilation effect,
concerning the action interval proposed by Ogawa et al.19.
Several studies have evaluated the use of certain medications, including acetylsalicylic
acid, parenteral heparin, and glycoprotein IIB-IIIA inhibitors (tirofiban); however,
these show benefits only when administered together20. When heparin and tirofiban were associated with intraluminal injection before passing
the last point of the anastomosis, there was a significant increase in serial patency
with 62 anastomoses21.
Some natural antioxidant flavonoids, such as epigallocatechin, which is present in
green tea, were tested against saline solution on the microsurgical arterial anastomosis
site with good effects; when easily accessible to the laboratory, they can be another
tool to prevent early thrombosis and cause vasodilation22.
Type III phosphodiesterase inhibitors, such as cilostazol, have already been successfully
applied in animal models designed to develop arterial thrombosis, with a statistically
significant success23. However, due to its application a few hours before surgery, it increases the preparation
time for training and is not as practical as the measures presented in our series,
which were all performed quickly and during the intraoperative period.
Pentoxifylline, a xanthine-derived drug with peripheral vasodilator action, has already
been successfully used in experimental models that favor thrombosis24. However, the technique involved serial applications, which also increased the preparation
time and the cost of training.
Among other possibilities, the use of 10% ethanol, applied subcutaneously, close to
the vessel area, 7 days before the surgical approach, has been reported25. Ethanol can activate nitric oxide and prostaglandins, reduce vasospasm, and inhibit
platelet aggregation. This study reported an increase in vascular diameter and lower
rates of arterial thrombosis.
Botulinum toxin also plays a role in the prevention of arterial thrombosis. Both types
A26 and B27 show benefits by reducing thrombosis rates, in addition to generating vessels with
larger diameters.
Mechanical actions also directly affect patency rates. When some type of torsion28 or changes in the angulations29 of the anastomoses are performed, the patency rates decrease proportionally.
When comparing the patency rate between the different techniques, the intermittent
compression was superior, in absolute numbers, in relation to the others; fixed compression
had the lowest absolute patency index. However, there was no statistical difference
between the groups, although Group 1, intermittent compression, showed p=0.07. Considering that the number of rats in this study was small, a probable statistical
difference could be expected if more arterial anastomoses were performed. It was not
possible to find in the literature other articles that carried out studies with the
use of fixed and intermittent compression to reduce thrombosis and therefore it was
not possible to make a comparison with similar articles.
Most studies compare the rates of anastomosis patency in the period between one and
24 hours after the procedure. A recent study published with the use of heparin in
arterial microsurgical anastomosis found a rate of 13% of thrombosis after 1 hour
of anastomosis compared with the control group. Another study that compared the patency
of surgical microsurgical anastomosis using sildenafil and papaverine observed an
immediate thrombosis rate of 20% and 30%, respectively, compared to the control group30. The present article compared the groups with the patency rate at 7 days after anastomosis,
which may explain the lower patency rates compared to the literature.
A fundamental tactic is the need to avoid the use of solutions or surgical environments
at low temperatures since hypothermia is known to be a complicating factor, leading
to vasospasm and higher rates of thrombosis.
In the future, the presented tactic can be tested in venous anastomoses, serving as
advanced training since the veins of the approached animals have a small caliber,
making the procedure more challenging. Further studies using a greater “n” should
be conducted to validate the superiority of the intermittent compression technique.
There are some methodological limitations in the present study: the small number of
animals as a consequence of the low availability in the experimental surgery, the
absence of a group with heparin, and the fact that the anastomosis performed at one
femoral artery may affect the contralateral anastomosis patency.
CONCLUSION
Arterial compression proved to be a possibility in an attempt to reduce thrombosis
rates in microsurgical arterial anastomosis. Although intermittent compression had
lower risks of thrombosis, there was no statistically significant difference in this
study. It was also observed that fixed compression increased the chances of anastomosis
failure. Thus, it is necessary to carry out studies with larger populations to determine
the validity of mechanical methods in arterial anastomoses.
Acknowledgments
We thank the professionals of the Experimental Research Units of the University of
Medicine of Botucatu and professor and statistician, Lídia Raquel de Carvalho. We
would like to thank Editage for English language editing.
REFERENCES
1. Rickard RF, Hudson DA. A history of vascular and microvascular surgery. Ann Plast
Surg. 2014;73(4):465-72.
2. Viterbo F. A importância da microcirurgia na cirurgia plástica. Rev Bras Cir Plást.
2012;27(1):2.
3. Cunha MS, Ramos RS, Torres ALG, Souza DAM, Agra IMG, Eulálio JN. Aplicação da microcirurgia
no serviço de cirurgia plástica da Universidade Federal da Bahia: análise dos resultados
e complicações. Rev Col Bras Cir. 2005;32(6):297-303.
4. Pessoa BBGP, Pessoa SGP. Treinamento em microanastomoses utilizando tubos de látex.
Acta Cir Bras. 2002;17(2):143-6.
5. Dias IS, Pessoa SGP, Benevides AN, Macêdo JE. Treinamento inicial em microcirurgia
Rev Bras Cir Plást. 2010;25(4):595-9.
6. Brown E, Suh HP, Han HH, Pak CJ, Hong JP. Best new flaps and tips for success in microsurgery.
Plast Reconstr Surg. 2020;146(6):796-807.
7. Colakoglu S, Tebockhorst S, Chong TW, Mathes DW. Patient safety in microvascular plastic
surgery. J Reconstr Microsurg. 2019;35(9):631-9.
8. Abi-Rafeh J, Zammit D, Mojtahed Jaberi M, Al-Halabi B, Thibaudeau S. Nonbiological
Microsurgery Simulators in Plastic Surgery Training: A Systematic Review. Plast Reconstr
Surg. 2019;144(3):496e-507e.
9. Kinshoku MR, Rodriguez CAL, Fidalgo RS, Duran CCG, Leme PLS, Duarte IS. Rational use
of animal models for research and microsurgery training. Rev Col Bras Cir. 2012;39(5):414-7.
10. Mathon B. Learning vascular microsurgical techniques on an animal model. Neuro-Chirurgie.
2014;60(5):227-33.
11. Mücke T, Wolff C, von Düring M, Mitchell DA, Ritschl LM, Fichter AM. Form and size
matter: Increased risk of thrombosis in microvessels with surgically created endothelial
lesions. J Reconstr Microsurg. 2017;33(1):40-4.
12. Kaidar-Person O, Rosenthal RJ, Wexner SD, Szomstein S, Person B. Compression anastomosis:
history and clinical considerations. Am J Surg. 2008;195(6):818-26.
13. Chen LE, Seaber AV, Urbaniak JR. Thrombosis and thrombolysis in crushed arteries with
or without anastomosis: a new microvascular thrombosis model. J Reconstr Microsurg.
1996;12(1):31-8.
14. Menezes Neto BF, Oliveira Neto FV, Secanho MS, Carvalho LB, Moragas WR, Fernandes
MS. Submerged vascular anastomosis. A technique for vascular suturing in experimental
microsurgery. Acta Cir Bras. 2021;36(8):e360807.
15. Yoon AP, Jones NF. Critical time for neovascularization/angiogenesis to allow free
flap survival after delayed postoperative anastomotic compromise without surgical
intervention: A review of the literature. Microsurgery. 2016;36(7):604-12.
16. Shaughness G, Blackburn C, Ballestín A, Akelina Y, Ascherman JA. Predicting Thrombosis
Formation in 1-mm-Diameter Arterial Anastomoses with Transit-Time Ultrasound Technology.
Plast Reconstr Surg. 2017;139(6):1400-5.
17. Cox GW, Runnels S, Hsu HS, Das SK. A comparison of heparinised saline irrigation solutions
in a model of microvascular thrombosis. Br J Plast Surg. 1992;45(5):345-8.
18. Malm K, Dahlbäck B, Arnljots B. Low-molecular-weight heparin (dalteparin) effectively
prevents thrombosis in a rat model of deep arterial injury. Plast Reconstr Surg. 2003;111(5):1659-66.
19. Ogawa H, Kusumoto J, Nomura T, Hashikawa K, Terashi H, Sakakibara S. Wire Myography
for Continuous Estimation of the Optimal Concentration of Topical Lidocaine as a Vasodilator
in Microsurgery. J Reconstr Microsurg. 2021;37(6):541-50.
20. Yokoyama T, Kadota S, Takeuchi K, Tosa Y, Kadomatsu K, Shimizu Y, et al. Changes in
the blood flow and prevention of vasospasm of the femoral artery by topical application
of lidocaine in rats. Ann Plast Surg. 2011;67(2):178-83.
21. Chung TL, Pumplin DW, Holton LH 3rd, Taylor JA, Rodriguez ED, Silverman RP. Prevention
of microsurgical anastomotic thrombosis using aspirin, heparin, and the glycoprotein
IIb/IIIa inhibitor tirofiban. Plast Reconstr Surg. 2007;120(5):1281-8.
22. Yates YJ, Farias CL, Kazmier FR, Puckett CL, Concannon MJ. The effect of tirofiban
on microvascular thrombosis: crush model. Plast Reconstr Surg. 2005;116(1):205-8.
23. İğde M, Onur Öztürk M, Yaşar B, Hakan Bulam M, Ergani HM, Ünlü RE. Antithrombotic
effect of epigallocatechin gallate on the patency of arterial microvascular anastomoses.
Arch Plast Surg. 2019;46(3):214-20.
24. Kim SH, Chang HW, Choi TH, Kim JH, Son D, Han K, et al. Cilostazol effectively reduces
the decrease of flow volume in a thrombotic anastomosis model in a rat: a novel application
of ultrasonography for evaluation. Ann Plast Surg. 2010;64(4):482-6.
25. Kronen G, Ferder M, Hunzicker K, Strauch B. The use of pentoxifylline in microvascular
surgery. J Reconstr Microsurg. 1994;10(1):17-20.
26. Nasiri M, Kardar MH. Effect of Ethanol on Micro-Vessels Diameter and Prevention of
Thrombosis. World J Plast Surg. 2019;8(2):249-53.
27. Fathi M, Fathi H, Mazloumi M, Khalilzadeh O, Amanpour S, Meysamie A, et al. Preventive
effect of botulinum toxin A in microanastomotic thrombosis: a rabbit model. J Plast
Reconstr Aesthet Surg. 2010;63(10):e720-4.
28. Janz BA, Thomas PR, Fanua SP, Dunn RE, Wilgis EF, Means KR Jr. Prevention of anastomotic
thrombosis by botulinum toxin B after acute injury in a rat model. J Hand Surg Am.
2011;36(10):1585-91.
29. Bilgin SS, Topalan M, Ip WY, Chow SP. Effect of torsion on microvenous anastomotic
patency in a rat model and early thrombolytic phenomenon. Microsurgery. 2003;23(4):381-6.
30. Salgarello M, Lahoud P, Selvaggi G, Gentileschi S, Sturla M, Farallo E. The effect
of twisting on microanastomotic patency of arteries and veins in a rat model. Ann
Plast Surg. 2001;47(6):643-6.
1. Hospital das Clínicas da Faculdade de Medicina de Botucatu, Botucatu, SP, Brazil
Corresponding author: Balduino Ferreira de Menezes Neto Rua Doutor Adolfo Pardini Filho, 1028, Chácara Recreio Vista Alegre, Botucatu, SP,
Brazil Zip Code: 18608-760, E-mail: balduinofmneto@gmail.com
Article received: November 22, 2023.
Article accepted: February 04, 2024.
Conflicts of interest: none.