INTRODUCTION
Breast cancer, except non-melanoma skin tumors, is the main cause of neoplasia in
women in Brazil, in much of the world, and also the one with the highest lethality.
Therefore, it is a public health problem1.
Estimates reveal that, in the 2020-2022 biennium, there would be an incidence of 66,280
new cases, corresponding to 29.7% of cancers in women, with survival and prognosis
closely related to access to the health system, early diagnosis, and adequate treatment1.
Treatment is based on local therapies (surgery and radiotherapy) and systemic therapies
(chemotherapy, hormone therapy, and biological therapy)2. The application of immediate breast reconstruction is increasingly recommended,
given the advancement of adenomastectomy, sparing the total or partial skin envelope
(nipple-sparing or skin-sparing, respectively), which guarantees better quality and
quantity of skin for reconstructions. with prostheses or even with autologous tissue,
at the same surgical time. Therefore, currently, the restoration of the shape, contour,
and volume of the breast concomitantly with mastectomy is a reality, as well as a
key point in the psychological recovery and quality of life, even if partial, in the
face of the disease3,4.
The most commonly used procedures in breast reconstruction use implants and/or autologous
tissue. These are the pedicled myocutaneous flap of the latissimus dorsi (LD), transverse
myocutaneous flap of the rectus abdominis muscle (TRAM), local muscular flap (LF),
and the use of alloplastic materials (expanders and silicone prostheses). Although
we know the benefits of their applicability in immediate breast reconstruction, these
techniques are not free from complications such as seromas, hematomas, surgical wound
infection, flap necrosis, prosthesis extrusion, and capsular contracture. And, sometimes,
they are related to comorbidities such as smoking, surgical technique in adenomastectomy
(especially care regarding the thickness and regularity of the skin flap), the expertise
of the team involved in breast reconstruction, and the application of radiotherapy
and chemotherapy5,6.
OBJECTIVE
The present work aims to demonstrate the team’s experience in post-mastectomy breast
reconstruction with prosthesis or with autologous tissue with or without a breast
implant, discuss operative techniques and complications concerning data from the world
literature to, finally, verify the applicability of the technique in the team’s clinical
practice.
METHOD
We analyzed, through a retrospective review of medical records, 791 female patients
who underwent mastectomy with immediate or delayed breast reconstruction from January
2010 to June 2020. The project was approved by the Research Ethics Committee (opinion
number 5,660,021 ). The techniques of TRAM, LD, LF (serratus anterior and pectoralis
major), expander, reverse expander, oncoplastic, lateral thoracic fasciocutaneous
flap (Hölmstrom), and reconstruction with prepectoral implant were used, techniques
associated or not with silicone implants. When used, breast implants were natural
or round in shape, had high or extra-high projection, and had a textured surface.
The reconstruction technique applied was decided together with the patients and by
analyzing some factors. Patients undergoing modified radical mastectomy with a donor
abdomen, non-smokers, and without impeding abdominal scars were candidates for reconstruction
with TRAM. Patients without these conditions and intending to become pregnant were
selected for reconstruction with LD. And those who requested minor surgery or with
important comorbidities such as lung disease and heart disease were indicated for
LF or Hölmstrom flap.
In cases of patients undergoing skin-sparing or nipple-sparing mastectomy, with total
or partial preservation of the skin envelope, reconstruction with a prepectoral prosthesis
was chosen, as long as the skin flap was of sufficient thickness. When the flap was
excessively thin, it was decided to use the implant in conjunction with an LF or partially
filled skin expander during surgery. Furthermore, some cases received a skin expander
for salvage surgeries and late reconstructions, in patients who did not have a donor
area or did not want another technique.
Factors such as age, laterality, comorbidities, smoking, mastectomy technique, types
of incisions, the timing of reconstruction (immediate or delayed), complications (seroma,
hematoma, infection, necrosis, dehiscence, and prosthesis exposure), and need for
a second surgery were analyzed. (change of prosthesis size, reconstruction of the
nipple-areolar complex - NAC, contralateral breast symmetrization, fat grafting, capsulotomy,
or capsulectomy).
RESULTS
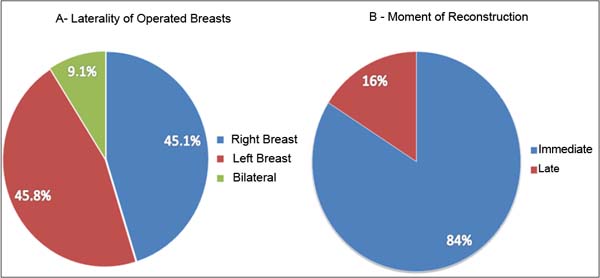
The number of patients operated on during the period was 791 cases, between 27 and
79 years old, with an average of 51 years old, with follow-up time varying between
five months and ten years and 11 months, which corresponded to a total of 860 reconstructed
breasts; 356 approaches to the right breast, 360 to the left breast and 72 bilateral
cases (Figure 1), 84% immediate reconstructions and 16% late reconstructions (Figure 1).
Figure 1 - A: Percentage of laterality of operated breasts; B: Percentage of the moment of reconstruction.
Figure 1 - A: Percentage of laterality of operated breasts; B: Percentage of the moment of reconstruction.
Regarding the access route to the breast tissue, 498 Stewart-type incisions were used;
217 extended inframammary incisions; 75 periareolar; 37 inverted T, and 33 incisions
in the upper external quadrant. 498 modified radical mastectomies were performed;
244 nipple-sparing; 95 skin-sparing; 15 prophylactic mastectomies and 8 quadrantectomies.
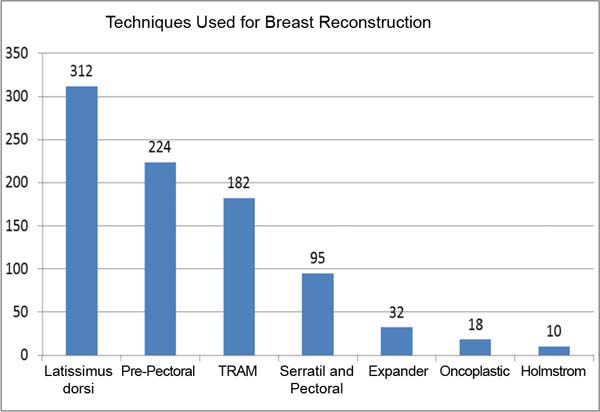
Regarding the breast reconstruction technique used, 35.7% were reconstructions with
LD, 25.6% with prepectoral prosthesis, 20.8% with TRAM, 10.9% with LF (serratus anterior
and pectoralis major), 3 .8% with expander; 2% oncoplastic; and 1.1% Hölmstrom flap
(Figure 2).
Figure 2 - Numbers of cases by type of breast reconstruction technique.
Figure 2 - Numbers of cases by type of breast reconstruction technique.
The reconstruction techniques with prepectoral prosthesis, LD, LF, and Hölmstrom flap
used a silicone prosthesis with a volume between 155 and 640ml (average of 351), 85%
with a natural profile, and 15% round.
The main comorbidities found in patients were hypertension, diabetes, hypothyroidism,
depression, and obesity. In 5% of patients (44 cases) smoking was active at the time
of reconstruction.
When it comes to complications related to the use of implants, the most notable is
the loss of the prosthesis in 70 patients (20 cases due to necrosis, 25 due to post-chemotherapy
seroma infection, and 25 due to surgical wound dehiscence) and contracture grades
II, III and Baker IV in 52 cases.
In TRAM reconstructions, there were six cases of abdominal bulging, two cases of abdominal
hernia, and three cases of seroma in the donor area.
In general complications, 45 cases of surgical wound dehiscence were identified, 32
cases of skin necrosis due to mastectomy, 30 cases of seroma in the recipient area,
and 12 cases in the donor area (three when TRAM and nine when LD), 27 cases of surgical
site infection, eight cases of hematoma, two cases of partial flap necrosis with good
evolution, four cases of total flap necrosis, two cases of large liponecrosis, one
case of post-mammogram prosthesis rupture, three cases of pain chronic and one case
of paraplegia due to extradural hematoma.
A second surgical procedure was necessary for 258 patients, distributed as follows:
17 prosthesis exchanges, 51 NAC reconstructions, 97 contralateral breast symmetrizations,
38 fat grafts, 27 capsulotomies or capsulectomies, 10 prosthesis repositionings, and
18 contralateral risk-reducing surgeries.
In the long term, 20 patients had tumor recurrences, 10 patients developed a second
primary tumor in the contralateral breast, 16 patients had metastases, five patients
underwent salvage reconstruction with an expander after loss of the prosthesis and
three patients required placement of a new prosthesis.
DISCUSSION
Breast reconstruction is currently not restricted to the concept of breast cone reconstruction.
The naturalness and similarity concerning the contralateral breast are highly valued
by the team and the patient and, in this context, advances in techniques and alloplastic
materials, when used, help with results3,7,8.
In the present study, the percentage of immediate reconstructions (84%) is in line
with the current preference for applying immediate breast reconstruction to adenomastectomy,
and the use of implants has grown in the same proportion. Studies show that 80% of
reconstructions are immediate with prosthesis9,10. Although it is considered safe, effective, reliable, and can be used especially
in women with various comorbidities, high rates of complications (capsular contracture
and infection) with the use of prostheses are seen, especially if followed by radiotherapy9. In our 10-year series, the rate of prosthesis loss (8%) is in line with values found
in the literature (7% - 9%), while the rates of seroma and capsular contractures are
considerably lower (6% and 5% against 12 - 21% and 19% respectively)6.
Meta-analyses by Toh et al.11 and Gurrado et al.10 showed that there was no statistical significance between the rates of infection,
seroma, hematoma, and capsular contracture between immediate reconstruction with prosthesis
and two-stage expander-prosthesis reconstruction. However, the incidence of necrosis,
reoperation, and loss of the prosthesis were higher in immediate reconstructions with
prostheses.
In a ten-year retrospective analysis, Mak & Kwong5 collected data from 243 patients who underwent immediate autologous and prosthetic
breast reconstructions with a follow-up of approximately two years. Patients undergoing
autologous reconstruction had lower complication rates (24.4%) than those undergoing
reconstruction with a prosthesis (50%). Among the most relevant complications, bulging
and abdominal hernia stand out (9.1%). In the present study, surgical site dehiscence
was the main complication of this type of reconstruction (5.2% of operated cases).
A great advantage of reconstruction with autologous tissue is that aesthetic damage
to the breast is less after radiotherapy3,4. In cases where immediate breast reconstruction is indicated, despite the certainty
of adjuvant radiotherapy, reconstruction options should be based on tissue characteristics
and blood supply and reconstruction options with autologous tissue should have priority
as they reflect superior vascularization, resistance to radiation, better sensory
recovery and lower failure rates4,6,8. However, factors such as team expertise, improvement in the target of the irradiated
breast, and thickness of the skin flap in mastectomy directly influence these results4,8.
CONCLUSION
Breast reconstruction with alloplastic material or autologous tissue with or without
a breast implant is an indispensable tool for a woman’s physical and emotional recovery.
And, with good team preparation, the techniques are consistent, reliable, low morbidity,
and with excellent aesthetic results when well indicated.
REFERENCES
1. Brasil. Ministério da Saúde. Instituto Nacional de Câncer José Alencar Gomes da Silva
(INCA). Estimativa 2020: incidência de câncer no Brasil. Rio de Janeiro: INCA; 2019.
2. Brasil. Ministério da Saúde. Instituto Nacional de Câncer José Alencar Gomes da Silva
(INCA). A situação do câncer de mama no Brasil: síntese de dados dos sistemas de informação.
Rio de Janeiro: INCA; 2019.
3. Toyserkani NM, Jørgensen MG, Tabatabaeifar S, Damsgaard T, Sørensen JA. Autologous
versus implant-based breast reconstruction: A systematic review and meta-analysis
of Breast-Q patient-reported outcomes. J Plast Reconstr Aesthet Surg. 2020;73(2):278-85.
4. Citgez B, Yigit B, Bas S.Oncoplastic and Reconstructive Breast Surgery: A Comprehensive
Review. Cureus. 2022;14(1):e21763.
5. Mak JC, Kwong A. Complications in Post-mastectomy Immediate Breast Reconstruction:
A Ten-year Analysis of Outcomes. Clin Breast Cancer. 2020;20(5):402-7.
6. Friedrich M, Krämer S, Friedrich D, Kraft C, Maass N, Rogmans C. Difficulties of Breast
Reconstruction - Problems That No One Likes to Face. Anticancer Res. 2021;41(11):5365-75.
7. Siqueira HFF, Teixeira J, Lessa Filho R, Brito EAC, Lima M, Moura AR, et al. Aesthetic
assessment of breast reconstruction in the eyes of plastic surgeons versus nonplastic
physicians. Rev Assoc Med Bras. 2022;68(1):13-8.
8. Choi M, Frey JD. Optimizing Aesthetic Outcomes in Breast Reconstruction After Nipple-Sparing
Mastectomy. Aesthet Surg J. 2020;40(Suppl 2):S13-21.
9. Ho TB, Wood WC, Mspt PDS. Breast Reconstruction in the Setting of Postmastectomy Radiotherapy:
Controversies and Disparities. Oncology (Williston Park). 2019;33(12):688845.
10. Gurrado A, Pasculli A, Toma A, Maruccia M, Elia R, Moschetta M, et al. Mastectomy
with one-stage or two-stage reconstruction in breast cancer: analysis of early outcomes
and patient’s satisfaction. Updates Surg. 2023;75(1):235-43.
11. Toh U, Takenaka M, Iwakuma N, Akagi Y. Clinical outcomes of patients after nipple-sparing
mastectomy and reconstruction based on the expander/implant technique. Surg Today.
2021;51(6):862-71.
1. Hospital Universitário da Universidade Federal de Juiz de Fora, Juiz de Fora, MG, Brazil
2. Sociedade Brasileira de Cirurgia Plástica, Juiz de Fora, MG, Brazil
Corresponding author: Larissa Silva Leitão Daroda Rua Catulo Breviglieri, s/nº, Bairro Santa Catarina, Juiz de Fora, MG, Brazil, Zip Code: 36036-110, E-mail: larissadaroda@gmail.com
Article received: July 3, 2023.
Article accepted: December 5, 2023.
Conflicts of interest: none.