INTRODUCTION
Correction of the nasal radix dorsum relationship has been carried out for several
years using the most varied techniques such as auricular, septal, or costal cartilage
graft, filling with hyaluronic acid, use of fascia and grafts, and use of diced cartilage,
silicone, and hyaluronic acid1-4.
The use of chopped cartilage in the dorsal region began shortly after the Second World
War with the work of Gordon & Warren1 and Peer2. Soon after this period, the difficulty in establishing safe criteria to reduce local
complications resulted in little use of this resource, and only in the 1990s, the
technique was taken up by the work of Erol3-5, with “Turkish delight”, and reproduction by Guerrerosantos et al.6 and Daniel & Calvert7.
With the possibility of reproducibility of the technique described in several studies8-14, there is a description of chopped cartilage placed in planes on the nasal surface,
whether or not using muscular fascia.
Cartilage graft is commonly used to augment the nasal dorsum, either as full cartilage
or with chopped cartilage. The radix region is one of the main beneficiaries of the
use of cartilage in this region, which allows for a back with greater harmony and
visual beauty. According to McKinney & Sweis15, the ideal radix height is three-quarters of the nasal length or nasal projection.
According to Taş13, the use of chopped cartilage graft in the dorsal region is a way to establish a
beautiful and smooth back.
OBJECTIVE
In this study, we analyzed the use of a minced cartilage graft to increase the height
of the nasal radix. The use of fragmented cartilage is described in the literature
and this technique has gained followers in recent years. The objective is to describe
our experience with the use of fragmented cartilage graft to augment the back, comparing
visual and tactile perception with patient satisfaction.
METHOD
The study was carried out on patients undergoing rhinoplasty from January 2018 to
June 2022, at the Hospital Centro Estadual de Reabilitação e Readaptação Dr. Henrique
Santillo, in Goiânia, GO, in surgeries in which the radix was increased with the use
of minced cartilage graft, with patients being evaluated 6 months postoperatively.
As exclusion criteria, patients under 18 years of age, with rheumatological comorbidities,
and diseases that destroy cartilage such as leishmaniasis, leprosy, and Wegener’s
granulomatosis were established.
The study was approved by the hospital’s internal ethics committee and platform Brasil
CAEE 30798120.6.0000.5082 and the data were tabulated in Excel 23 (Microsoft®), collecting the following information: age, sex, Fitzpatrick classification, skin
thickness, the origin of the graft, complications, tactile perception of the graft
and visual perception of the graft and satisfaction with the result.
RESULTS
Forty-seven patients who underwent radix augmentation with minced cartilage were studied.
Of these, 35 (74.4%) were female and 12 (25.6%) were male, with a mean age of 34.6
years (18-44).
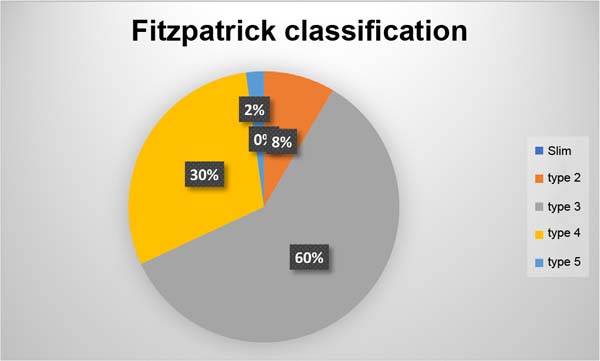
Regarding Fitzpatrick skin type, they were type 2 (n=4, 8.5%), type 3 (n=28, 59.5%),
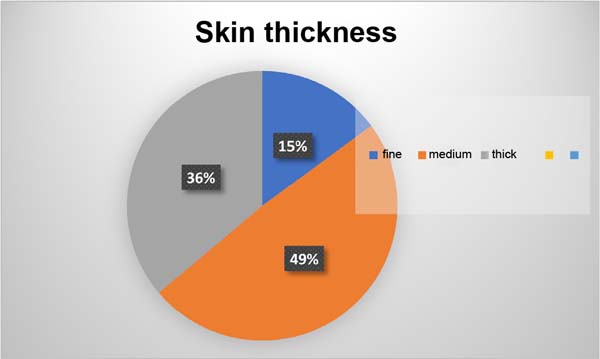
type 4 (n=14, 29.8%) and type 5 (n =1, 2.2%), with thin skin (n=7, 14.9%), medium
skin (n=23, 48.9%) and thick skin (n=17, 36.2%) (Figures 1 and 2).
Figure 1 - Fitzpatrick classification.
Figure 1 - Fitzpatrick classification.
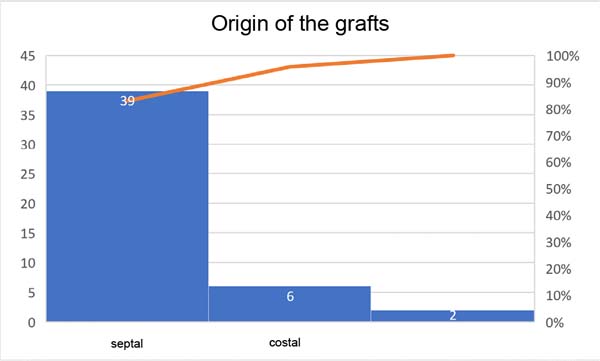
Figure 2 - Origin of the grafts.
Figure 2 - Origin of the grafts.
The origin of most grafts was from septal cartilage (n=39, 83%), costal cartilage
(n=6, 12.8%), and auricular cartilage (n=2, 4.2%) (Figure 3).
Figure 3 - Skin thickness.
Figure 3 - Skin thickness.
Complications present were infection (1 case), migration of chopped cartilage (3 cases),
and partial resorption (1 case).
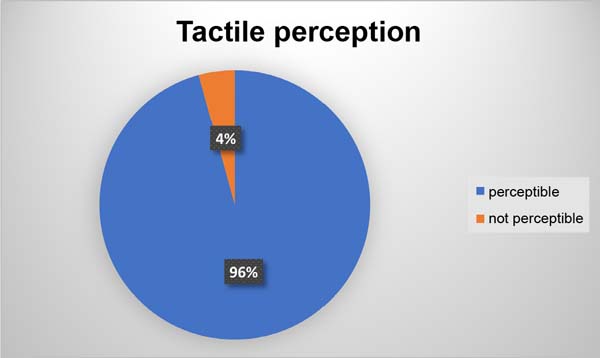
In the assessment of tactile perception, 42 patients (89.3%) noticed cartilaginous
prominences on palpation, but this did not bother them (Figure 4).
Figure 4 - Visual perception.
Figure 4 - Visual perception.
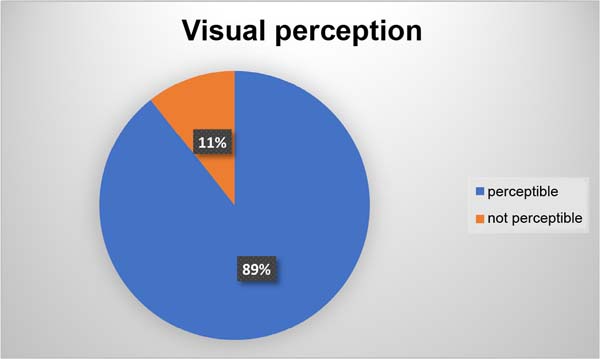
In the visual assessment, only 2 patients noticed the irregularity and local scraping
was performed with resolution (Figure 5).
Figure 5 - Tactile perception.
Figure 5 - Tactile perception.
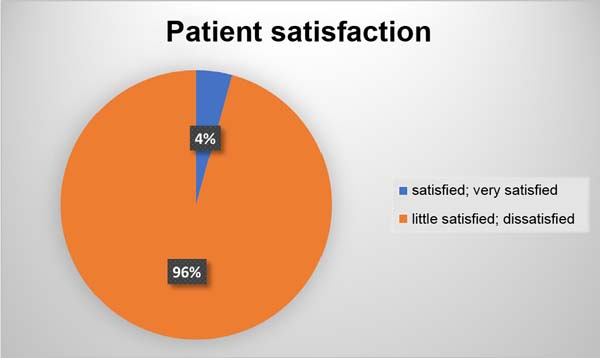
Of the patients studied 45 reported satisfaction with the result (very satisfied and
satisfied) (Figure 6).
Figure 6 - Patient satisfaction.
Figure 6 - Patient satisfaction.
Figures 7 to 13, demonstrate the procedures for preparing the cartilage, its introduction into the
radix, and visualization of the result.
Figure 8 - Application of fragmented cartilage to the radix.
Figure 8 - Application of fragmented cartilage to the radix.
Figure 9 - Measurements in the immediate preoperative period.
Figure 9 - Measurements in the immediate preoperative period.
Figure 10 - Immediate post-operative period.
Figure 10 - Immediate post-operative period.
Figure 11 - Preoperative with rhinomanometer.
Figure 11 - Preoperative with rhinomanometer.
Figure 12 - Immediate postoperative period after the introduction of cartilage into the radix.
Figure 12 - Immediate postoperative period after the introduction of cartilage into the radix.
Figure 13 - Late postoperative period: 1 year.
Figure 13 - Late postoperative period: 1 year.
DISCUSSION
The first experiments described by Gordon & Warren1 served to validate the technique, showing that the cartilage survived by occupying
the space in which it was inserted. From this, several uses were initiated in hernioplasty16, reconstruction of the costal wall17, nose and face18,19 and hip20. The difficulty in reproducing the technique with mastery ended up leaving it forgotten,
only being rescued by Erol decades later.
The initial work described by Erol used Surgicel or fascia to house chopped cartilage
grafts, in what is known as Turkish delight3. The versatility of sizes and thickness, as well as its use in primary and secondary
surgeries, allowed the dissemination of this technique21.
Grafts in the nasal region are part of modern rhinoplasty, being part of reorganizing
the structure and improving the shape. The ease of including chopped cartilage without
the need for a more rigid fixation such as a Kirschner wire or screw facilitates its
use and the possibility of shaping the back due to the malleability of the graft is
a superior advantage to the use of an onlay graft.
Vidal et al.12 describe the importance of using chopped cartilage graft in the point, back, and
radix relationship, highlighting the importance of using an appropriate technique
by detaching an area restricted only to the volume to be grafted, introducing the
graft through a syringe 1ml with the tip removed and microporation immediately upon
insertion of the graft for adequate molding. In our experience, we agree with these
statements and that we can use the syringe developed by Erol instead of the 1ml syringe
without harm, in addition to the possibility of a tunnel above the periosteum or perichondrium
for insertion of the chopped cartilage.
The perception of cartilage irregularity to the touch is described in other studies21,22, however, this study found that it is not visually perceptible and presents interesting
results. Ma et al.23 describe that fragmentation with pieces of cartilage smaller than 0.5 mm reduces
the visibility of irregularities, corroborating the results of this study.
The use of onlay cartilage on the radix region may present curves that distort the
symmetry of the region or even be perceived as asymmetry and mobilization on palpation.
The use of chopped cartilage presents tactile perception, but generally without visual
changes. Currently, the use of chopped cartilage can be associated with the use of
platelet-rich plasma that creates a continuous and unified structure, which can be
a solution for both tactile perception and avoiding migration.
The study has limitations such as the follow-up being only 6 months, which can invariably
present a higher rate of local resorption in the long term. The region studied is
limited to the radix. Being an observational study, it presents biases related to
its elaboration such as selection or information, as well as the possible presence
of confounding factors.
CONCLUSION
The study demonstrated that free minced cartilage can be used in the radix region
with satisfactory results, presenting a low rate of visual perception when compared
to tactile perception, without negatively influencing the satisfaction of the result.
REFERENCES
1. Gordon SD, Warren RF. Autogenous Diced Cartilage Transplants to Bone: An Experimental
Study. Ann Surg. 1947;125(2):237-40.
2. Peer LA. Diced cartilage grafts. Arch Otolaryngol. 1943;38(2):156-65.
3. Erol OO. The Turkish delight: a pliable graft for rhinoplasty. Plast Reconstr Surg.
2000;105(6):2229-41.
4. Erol ÖO. Chopped cartilage graft wrapped with Surgicel in nose surgery (plasticine-like
graft). In: Third European Association of Plastic Surgeons (EURAPS) Meeting; 1992
May 14-16; Pisa, Italy.
5. Erol ÖO. Chopped Cartilage Graft Wrapped with Surgicel in Nose Surgery (Plasticine-like
Graft). In: 11th Biennal Congress of the International Society of Aesthetic Plastic
Surgery. 1992 Feb 29-Mar 4; Guadalajara, Mexico.
6. Guerrerosantos J, Trabanino C, Guerrerosantos F. Multifragmented cartilage wrapped
with fascia in augmentation rhinoplasty. Plast Reconstr Surg. 2006;117(3):804-12.
DOI: 10.1097/01.prs.0000200068.73092.5d
7. Daniel RK, Calvert JW. Diced cartilage grafts in rhinoplasty surgery. Plast Reconstr
Surg. 2004;113(7):2156-71.
8. Guerrerosantos J. Temporoparietal free fascia grafts in rhinoplasty. Plast Reconstr
Surg. 1984;74(4):465-75.
9. Elahi MM, Jackson IT, Moreira-Gonzalez A, Yamini D Nasal augmentation with Surgicel-wrapped
diced cartilage: a review of 67 consecutive cases. Plast Reconstr Surg. 2003;111(3):1309-18.
10. Daniel RK. Diced cartilage grafts in rhinoplasty surgery: current techniques and applications.
Plast Reconstr Surg. 2008;122(6):1883-91.
11. Daniel RK. The role of diced cartilage grafts in rhinoplasty. Aesthet Surg J. 2006;26(2):209-13.
12. Vidal MA, Kokiso D, Vidal BP, Andrade Filho AML. Cartilagem fragmentada para aumento
do radix nasal. Rev Bras Cir Plást. 2015;30(1):2-7.
13. Taş S. Ultra Diced Cartilage Graft in Rhinoplasty: A Fine Tool. Plast Reconstr Surg.
2021;147(4):600e-6e. DOI: 10.1097/PRS.0000000000007794
14. Kreutzer C, Hoehne J, Gubisch W, Rezaeian F, Haack S. Free Diced Cartilage: A New
Application of Diced Cartilage Grafts in Primary and Secondary Rhinoplasty. Plast
Reconstr Surg. 2017;140(3):461-70. DOI: 10.1097/PRS.0000000000003622
15. McKinney P, Sweis I. A clinical definition of an ideal nasal radix. Plast Reconstr
Surg. 2002;109(4):1416-8; discussion 1419-20. DOI: 10.1097/00006534-200204010-00033
16. Simms GF, Irwin RC. Diced heomologous cartilage in hernioplasty. J Med Soc N J. 1952;49(9):406-7.
17. Brodkin HA, Peer LA. Diced cartilage for chest wall defects. J Thorac Surg. 1954;28(1):97-102.
18. Erdelyi R. Diced cartilage in plastic surgery. Acta Chir Orthop Traumatol Cech. 1960;27:521-8.
19. Limberg AA Jr. The use of diced cartilage by injection with a needle. 1. Clinical
investigations. Plast Reconstr Surg Transplant Bull. 1961;28:523-36.
20. Lemperg R. Studies of autologous diced costal cartilage transplant. II. With special
regard to morphological changes and 35S-sulphate uptake in vitro after transplantation
to the hip joint. Acta Soc Med Ups. 1967;72(3):141-72.
21. Erol OO. Long-Term Results and Refinement of the Turkish Delight Technique for Primary
and Secondary Rhinoplasty: 25 Years of Experience. Plast Reconstr Surg. 2016;137(2):423-37.
DOI: 10.1097/01.prs.0000475755.71333.bf
22. Souza GMC, Costa SM, Penna WCNB. Enxerto de cartilagem picada injetável para rinoplastia:
método e experiência do Hospital Felício Rocho. Rev Bras Cir Craniomaxilofac. 2012;15(1):17-20.
23. Ma JG, Wang KM, Zhao XH, Cai L, Li X. Diced Costal Cartilage for Augmentation Rhinoplasty.
Chin Med J (Engl). 2015;128(19):2679-81.
1. CRER - Centro Estadual de Reabilitação e Readaptação, Goiânia, GO, Brazil
2. Instituto Arruda Cirurgia Plástica, Goiânia, GO, Brazil
Corresponding author: Fabiano Calixto Fortes Arruda Rua T50 n 723 Setor Bueno Goiânia, GO, Brazil, Zip Code: 74215-200, E-mail: arrudafabiano@hotmail.com
Article received: April 4, 2023.
Article accepted: December 5, 2023.
Conflicts of interest: none.