



Case Report - Year 2026 - Volume 41Issue 1
Madelung's Disease and Treatment through Plastic Surgery: A Case Report with a Literature Review
Doença de Madelung e tratamento por cirurgia plástica: Um relato de caso com revisão da literatura
Thaylandiê Basílio Cavalcante Cruz1 ; João Luiz Bezerra de Menezes Saraiva2,; Bruna Viana Teles Rebouças2; Anik Moraes Marangoni2; Isabela Franco Freire2; Raíra Marques Oliveira2; Salustiano Gomes de Pinho Pessoa1; Márcio Ribeiro Studart da Fonseca3
; João Luiz Bezerra de Menezes Saraiva2,; Bruna Viana Teles Rebouças2; Anik Moraes Marangoni2; Isabela Franco Freire2; Raíra Marques Oliveira2; Salustiano Gomes de Pinho Pessoa1; Márcio Ribeiro Studart da Fonseca3
ABSTRACT
Madelung's disease (MD) is a rare adipose-tissue condition characterized by multiple symmetrical lipomatous accumulations in the maxillofacial and cervical regions, the trunk, and the limbs. It sporadically affects individuals and is associated with a history of alcoholism. The aesthetic and functional impairments caused by this syndrome involve various aspects that justify the need for a Plastic Surgery approach. This paper reports the case of a male patient diagnosed with MD and treated with the aim of rehabilitation. A serial resection of the cervical lesions was chosen, with the performance of dermolipectomies and local flaps for reconstruction, along with resection of the submandibular glands and preservation of the adjacent nerve structures. The patient will later undergo further evaluation for treatment of the remaining lesions. The etiology of MD is unclear, but some factors are associated with its development, such as alcoholism, HIV infection, and metabolic disorders, including excessive insulin secretion, hyperuricemia, renal tubular acidosis, dyslipidemia, hypertriglyceridemia, as well as thyroid, adrenal, pituitary, and testicular function alterations. Despite its benign course, MD leads to significant psychosocial consequences, and surgical intervention aims to mitigate the effects of the deformities to restore the health of the affected patient.
Keywords: case reports; lipectomy; multiple symmetrical lipomatosis; plastic surgery; reconstructive surgery
RESUMO
A doença de Madelung (DM) é uma afecção rara do tecido adiposo que causa múltiplos acúmulos lipomatosos simétricos nas regiões maxilofacial e cervical, no tronco e nos membros. Acomete indivíduos de forma esporádica, e tem relação com o histórico de etilismo. O prejuízo estético e funcional da DM representa diversas facetas que justificam a necessidade de abordagem por cirurgia plástica. O presente trabalho relata o caso de um paciente do sexo masculino diagnosticado com DM e submetido a intervenções comfinalidade de reabilitação. Optou-se pela ressecção seriada das lesões cervicais, com a realização de dermolipectomias e uso de retalhos locais para a reconstrução, com ressecção das glândulas submandibulares e preservação da inervação adjacente. No futuro, o paciente será submetido a novas intervenções para abordagens das demais lesões. A etiologia da DM não foi esclarecida, mas alguns fatores foram associados ao seu desenvolvimento, como etilismo, infecção pelo HIV e distúrbios metabólicos, entre os quais se destacam a secreção excessiva de insulina, hiperuricemia, acidose tubular renal, dislipidemia, hipertrigliceridemia e alterações na função tireoidiana, adrenal, hipofisária e testicular. Apesar de ter curso benigno, a DM tem enormes consequências psicossociais, e a abordagem cirúrgica busca mitigar os efeitos das deformidades para o restabelecimento da saúde do paciente acometido.
Palavras-chave: cirurgia plástica; cirurgia reconstrutiva; lipectomia; lipomatose simétrica múltipla; relatos de casos
Introduction
Madelung’s disease (MD), also known as Madelung’s syn-drome, is a rare adipose-tissue disorder characterized by multiple diffuse lipomatous accumulations, whose patho-physiology remains largely unclear. It is typically identified sporadically, although there is an epidemiological associa-tion with a history of alcoholism. Diagnostic confirmation can be obtained through imaging and histological studies. The masses are most commonly located in the maxillofacial and cervical regions, trunk, and limbs. Patients seek medical attention due to aesthetic-functional limitations and periph-eral nerve involvement caused by the tumors. Symptoms resulting from the extrinsic compression effect exerted by the mass include dysphagia, dysphonia, restricted move-ment, and autonomic and/or somatic neuropathy.1,2
We herein report the case of a male patient diagnosed with MD who underwent plastic surgery for aesthetic and functional rehabilitation.
Case Report
A 56-year-old male patient was referred to the Plastic Surgery Department after consulting an endocrinologist. In 2015, he began to notice the development of expansive masses in his breasts, face, and neck, with no history of dysphagia or dyspnea, which led him to seek medical atten-tion. Subsequently, he noticed the appearence of masses in the testicular region. These lesions were lipomatous and expansile, increasing in size over the years. In terms of his medical history, the patient had a diagnosis of systemic arterial hypertension but was not undergoing treatment. Additionally, he had a history of pellagra associated with chronic alcohol use, previously treated. The patient denied any history of surgeries or of smoking. He reported alcohol use since the age of 18 years, consuming Brazilian Cachaça daily, with an estimated intake of approximately 20 g of ethanol per day. In his work, he reported constant exposure to ammonia.
Upon physical examination, he was in good general condition: acyanotic, anicteric, afebrile, and eupneic. Bilat-eral large gynecomastia was observed (►Fig. 1), along with lipomatous nodules on the shoulders, back, neck, and sub-mandibular region. A large adipose mass was palpable in the abdomen.


A computed tomography (CT) of the neck revealed an extensive, diffuse lipomatous mass involving the entire cervical region. The mass was situated deep to the platysma, involving the submental region and extending posteriorly to surround the sternocleidomastoid muscles. It extended through the deep cervical chain (Levels II, III, IV), the poste-rior triangle (Level V), and the anterior compartment (Level VI), continuing inferiorly into the supraclavicular regions. Furthermore, the mass involved the superficial tissues over-lying the trapezius muscles. The findings are highly consis-tent with a diagnosis of MD.
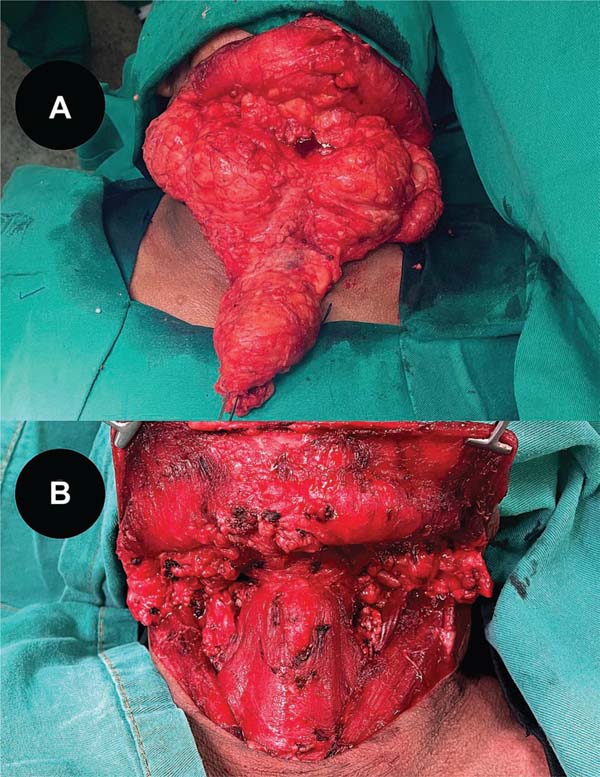
Following hospital admission and preoperative evalua-tions, the surgical plan consisted of staged resections with reconstruction via dermolipectomies and local flaps (►Figs. 2-3). The initial stage targeted the cervical region, the primary source of the patient’s discomfort. During the procedure, dissection was carried through the cervical layers, including the platysma muscle, to resect a mass found to have partially infiltrated the parotid glands, predominant-ly on the left. The hypoglossal nerve was preserved during the submandibular gland dissection, while the marginal mandibular nerve was protected through a meticulous dis-section of the inferior poles of the parotid glands, guided by its known anatomical course. This process was aided by intraoperative nerve monitoring, which enabled the precise identification and mapping of the nerve’s trajectory, ensur-ing its preservation along its entire length.



After meticulous hemostasis was confirmed, closure was achieved with a cervical myocutaneous flap, under which a Portovac drain was placed. The patient’s postoperative course was uneventful. Clinical examination revealed a well-perfused flap with no evidence of hematoma. The surgical wound healed well, showing no signs of infection or dehiscence (►Fig. 4).


The current study was approved by the Ethics Committee of Hospital Universitário Walter Cantídio, Universidade Fed-eral do Ceará (under CAAE: 81344924.9.0000.5045; # 7.013.588). The patient signed the free and informed consent form.
Discussion
Madelung’s disease, also known as multiple symmetrical lipomatosis or Launois-Bensaude syndrome,3 is a rare disease, with a limited number of cases described in the literature. It is characterized by the accumulation of multiple non-en-capsulated fatty masses in different parts of the body.1,2 The disease has an estimated incidence of 1:25,000, predomi-nantly affecting men between 30 and 60 years of age, with a male-to-female ratio ranging from 15:1 to 25:1. A strong association with chronic alcoholism is reported, as 60% to 90% of patients have a history of heavy alcohol use.1,4,5 However, the condition can also occur in non-alcoholic individuals and children.3
MD is a slowly progressive and benign condition, not typically associated with malignancy.1 While its etiology is not fully understood, its development has been linked to several factors. These include alcohol abuse, HIV, and a range of metabolic disorders such as dyslipidemia, hypertriglycer-idemia, hyperuricemia, renal tubular acidosis, and excessive insulin secretion, as well as endocrine dysfunctions affecting the thyroid, adrenal, pituitary, and testicular glands.1-3
The pathophysiology of the disease has not yet been fully understood, but it is thought to be related to a decrease in lipolysis stimulated by catecholamines and defects in mito-chondrial regulation in brown fat.1,2 Alcohol consumption is a relevant cofactor, due to its direct impact on mitochondrial metabolism, increased oxidative stress, and liver damage. In addition, it seems to reduce both the quantity and activity of beta-adrenergic receptors, which are necessary for lipolysis, reducing lipolysis and increasing lipogenesis.1,5 The patient in this case has a history of alcohol abuse since the age of 18, corroborating the association of alcohol as a cofactor in the pathophysiology of MD.
In a study of 31 patients with Madelung’s disease, Enzi et al.6 reported that compressive symptoms - such as dys-pnea, dysphagia, obstructive sleep apnea, and superior vena cava syndrome - could result from lipomas compressing or displacing mediastinal and upper airway structures, occa-sionally necessitating tracheostomy. Symptom severity often decreased following surgical resection of the mass. The most prevalent findings were related to somatic neuropathy, primarily upper and lower limb paresthesia, affecting over half of the patients studied. Electromyography confirmed a high prevalence of neuropathy, revealing motor neuropathy in 83.9% of patients and signs of autonomic impairment in 74.2%. Alterations in liver function tests correlated strongly with daily ethanol intake, and these levels improved in patients who reduced their consumption during follow-up. Notably, among the 8 patient deaths, 3 were from sudden death unrelated to coronary artery disease or other acute cardiac events; all 3 of these patients had severe autonomic neuropathy [6].
The clinical presentation of MD is characterized by a symmetrical distribution of lipomatous lesions, which can affect different parts of the body.1 Lipomas mainly affect the cervical region (“horse collar”), deltoid (pseudoathletic ap-pearance) and back (pseudocyphosis of the spine), but they can also appear in more caudal regions.3 The Enzi et al.6 classification is used to divide the disease into two types, according to the anatomical distribution of the lipomas. In type 1, the deposits are located in the neck, shoulders, supraclavicular triangle, and upper limbs. In type 2, the deposits occur in the abdomen and thighs.2 More recently, Donhauser et al.’s7 classification divided the disease into 4 types: type I (“horse collar”), type II (pseudoathletic appear-ance), type III (gynecoid) and type IV (abdominal). It is important to note that some patients may present more than one type of distribution.8 The patient in this report initially developed masses in the facial and cervical regions, which subsequently progressed to the chest, back, and scrotal region. This presentation is consistent with a mixed-type phenotype, encompassing features of multiple classifications.
The diagnosis is mainly based on clinical features and physical examination, and imaging and pathology tests can be used to complement it. Imaging tests show non-encapsu-lated fat deposits distributed symmetrically in the subcuta-neous tissue or in the spaces between muscles.1 The exam of choice is CT, which is used for diagnosis, preoperative staging and follow-up after surgery.3 Ultrasound and magnetic resonance imaging can also help with the diagnosis. Other diseases such as neurofibroma, liposarcoma, lipoblastoma-tosis, lipodystrophy, lymphoma, and neurofibromatosis should also be ruled out for proper management.8
Cessation of alcohol consumption is recommended for all patients with a history of alcohol abuse.3 However, the surgical treatment is the main therapeutic choice, with lipectomy and liposuction being the most effective options. The main aim of the treatment is to restore function and improve appearance, and, for this purpose, lipectomy is more effective, as it provides complete removal of the lipomatous lesions. However, the infiltrative nature of the masses can make this technique challenging, especially when adjacent anatomical structures are involved. More-over, lipectomy carries a higher risk of surgical complica-tions when compared to liposuction.9 The latter, although less invasive, has significant limitations when it comes to accessing deep and delicate regions, as well as a higher chance of recurrence compared to lipectomy, with rates of 20% and 14.1% respectively.2,10 Multiple surgeries are usually performed due to the difficulty in removing a large amount of adipose tissue in a single procedure. The use of tumescent solutions is a safe adjunct that can help reduce intraoperative bleeding and prolong anesthesia, facilitating the surgery.9,11 In this case, we initially decided to perform lipectomy in the cervical region, due to its proximity to important anatomical structures and the extent of the lesion.
Alternative local therapies, such as injection lipolysis, have also been described to reduce adipose tissue. These treatments involve injecting substances like phosphatidyl-choline, pentoxifylline, aminophylline, hyaluronic acid, yo-himbine, and collagenase directly into the lipomas.3 However, these methods have significant limitations. They may slow the progression of the masses without reducing the size of pre-existing ones, and achieving even moderate, temporary results requires numerous applications.10
Furthermore, the resulting local fibrosis can complicate subsequent surgical procedures like liposuction.3 Given these drawbacks, injection therapies are not considered an effective primary treatment, and surgical intervention remains the standard of care for all eligible cases.10
Conclusion
Although MD typically follows a benign clinical course with few systemic complications, it can have a profound impact on the patient’s quality of life due to significant aesthetic disfigurement and functional impairment. Therefore, surgi-cal intervention, utilizing techniques such as lipectomy and liposuction, remains the cornerstone of treatment. The primary goal of surgery is the functional and aesthetic rehabilitation of the patient, reaffirming its role as the definitive therapeutic approach for MD.
REFERENCES
1. Li R, Wang C, Bu Q, et al. Madelung’s Disease: Analysis of Clinical Characteristics, Fatty Mass Distribution, Comorbidities and Treatment of 54 Patients in China. Diabetes Metab Syndr Obes 2022;15:2365-2375. Doi: 10.2147/DMSO.S363836
2. Lee BH, Lee YM, Park SO, Chang LS, Kim YH. A Case Report of Madelung’s Disease. Arch Plast Surg 2023;50(05):463-467. Doi: 10.1055/a-2122-6121
3. Herbst KL. Subcutaneous Adipose Tissue Diseases: Dercum Disease, Lipedema, Familial Multiple Lipomatosis, and Madelung Disease. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth, MA: MDText.com, Inc. Available from: https://www.ncbi.nlm.nih.gov/books/NBK552156/
4. Vidal MdGC, Haygert CJP, Zagoury AR, Adaime SBR, Carrion RP, Londero TM. Doença de Madelung: relato de caso e revisão da literatura. Radiol Bras 2010;43(04):275-276. Doi: 10.1590/S0100-39842010000400014
5. Vassallo GA, Mirijello A, Tarli C, et al. Madelung’s disease and acute alcoholic hepatitis: case report and review of literature. Eur Rev Med Pharmacol Sci 2019;23(14):6272-6276. Doi: 10.26355/eurrev_201907_18448
6. Enzi G, Busetto L, Ceschin E, Coin A, Digito M, Pigozzo S. Multiple symmetric lipomatosis: clinical aspects and outcome in a long-term longitudinal study. Int J Obes Relat Metab Disord 2002;26(02):253-261. Doi: 10.1038/sj.ijo.0801867
7. Donhauser G, Vieluf D, Ruzicka T, Braun-Falco O. [Benign symme-tric Launois-Bensaude type III lipomatosis and Bureau-Barrière syndrome]. Hautarzt 1991;42(05):311-314
8. Jang N, Shin HW, Kim J, Yoon KC. A case report of Madelung’s disease. Arch Craniofac Surg 2020;21(05):305-308. Doi: 10.7181/acfs.2020.00304
9. Duc NQ, Tien NP, Tu NT, Huynh HN, Linh LD. Lipectomy for madelung disease using tumescent technique: a cross-sectional study. Ann Med Surg (Lond) 2023;85(06):2550-2558. Doi: 10.1097/MS9.0000000000000806
10. Frąk W, Gocel O, Sieniawski K, Sieniawska J, Włodarczyk M, Dziki L. Multiple symmetrical lipomatosis: A literature review and case report of a patient with Madelung’s disease. Pol Przegl Chir 2023; 96(00):130-134. Doi: 10.5604/01.3001.0053.5997
11. Wollina U, Heinig B. Madelung’s Disease - Case Series and Treatment by Tumescent Liposuction or Lipectomy. Open Access Maced J Med Sci 2017;5(04):427-431. Doi: 10.3889/oamjms.2017.114
1. Plastic Surgery and Microsurgery Service, Hospital Universitário Walter Cantídio,
Universidade Federal do Ceará, Fortaleza, CE, Brazil
2. Medicine Program, Centro de Ciências da Saúde, Universidade de Fortaleza, Fortaleza,
CE, Brazil
3. Head and Neck Surgery Service, Hospital Universitário Walter Cantídio, Universidade
Federal do Ceará, Fortaleza, CE, Brazil
Address for correspondence João Luiz Bezerra de Menezes Saraiva, Curso de Medicina, Centro de Ciências da Saúde, Universidade de Fortaleza, Avenida Washington Soares 1321, Edson Queiroz, Fortaleza, CE, CEP: 60811-905, Brazil (e-mail: joaoluizbmsaraiva@edu.unifor.br).
Article received: April 21, 2025.
Article accepted: August 12, 2025.
Conflict of Interests
The authors have no conflict of interests to declare.7
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket