



Review Article - Year 2026 - Volume 41Issue 1
Epidemiology of Burns in Peru: A Systematic Review and Single-Arm Meta-Analysis
Epidemiologia das queimaduras no Peru: Uma revisão sistemática e metanálise de braço único
Wilson Falco1, ; Gabriel Sanchez Okida1; Luis Enrique Robles-Aquije3; Vilma Yamilet Rojas-Carranza4; Ana Clara de Laurentiz Banzato1; Milena Freitas Martins1; José Antônio Sanches1; Pedro Henrique Soubhia Sanches1
; Gabriel Sanchez Okida1; Luis Enrique Robles-Aquije3; Vilma Yamilet Rojas-Carranza4; Ana Clara de Laurentiz Banzato1; Milena Freitas Martins1; José Antônio Sanches1; Pedro Henrique Soubhia Sanches1
ABSTRACT
Introduction Materials and
Methods This systematic review used four databases (PubMed, Embase, Virtual Health Library [VHL], and Web of Science) and gray literature sources. Inclusion criteria encompassed observational studies on burn patients in Peru. Data extraction and quality assessment adhered to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement and the 9-item checklist from the Joanna Briggs Institute (JBI). Meta-analysis was performed in R software using a random-effects model with inverse variance and logit transformation.
Results A total of 12 studies involving 3,446 patients were included. Children were the most affected group, and men were more frequently impacted. Most burns occurred in a domestic setting, resulting from hot liquids or direct fire. The limbs were the most commonly involved areas. The overall infection rate was 31.7% (95%CI: 21.46-44.08%; I2 = 0%) in studies without laboratory testing. The pooled mortality rate was 1.88% (95%CI: 0.54-6.36%; I2 = 67.1%).
Conclusion The literature on burns in Peru is limited and concentrated in specific urban centers. Most cases affected male children in domestic settings due to scalding. As such, there is a need for multicenter studies with standardized protocols, especially in underserved regions. Survey-based research could complement hospital data and improve the understanding of burn epidemiology in this country.
Keywords: epidemiology; Peru, burns; burns, electric; burns, inhalation; burns, chemical; systematic review
RESUMO
Introdução As queimaduras continuam sendo um importante problema de saúde pública, especialmente em países de baixa e média renda. No Peru, o perfil epidemiológico dos pacientes queimados ainda é pouco explorado na literatura. Este estudo teve como objetivo descrever a epidemiologia dessa coorte por meio de uma revisão sistemática e meta-análise.
Materiais e Métodos Essa revisão sistemática usou quatro bases de dados (PubMed, Embase, BVS e Web of Science) e literatura cinzenta. Foram incluídos estudos observacionais sobre casos de queimaduras no Peru. A extração de dados e a avaliação da qualidade seguiram as diretrizes da declaração Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) e o checklist de 9 itens do Instituto Joanna Briggs (JBI). Ameta-análise foi feita no software R, usando ummodelo de efeitos aleatórios com variância inversa e transformação logit.
Resultados Um total de 12 estudos foram incluídos, totalizando 3.446 pacientes. Crianças foram o grupo mais afetado, com predominância do sexo masculino. A maioria das queimaduras ocorreu em ambiente doméstico, causadas por líquidos quentes ou fogo direto. As extremidades foram as áreas mais atingidas. A taxa de infecção combinada foi de 31,7% (IC95%: 21,46-44,08%; I2=0%) em estudos sem testes laboratoriais. A mortalidade combinada foi de 1,88% (IC95%: 0,54-6,36%; I2=67,1%).
Conclusão Ademais, a literatura sobre queimaduras no Peru é limitada e concentra-se em centros urbanos específicos. Predominamcasos de crianças do sexo masculino em ambiente doméstico. Desse modo, há necessidade de estudos multicêntricos com protocolos padronizados, principalmente em regiões carentes. Pesquisas do tipo questionário podem complementar esses dados para ampliar a compreensão nacional da epidemiologia das queimaduras.
Palavras-chave: epidemiologia; Peru; queimaduras; queimaduras por corrente elétrica; queimaduras por inalação; queimaduras químicas; revisão sistemática
Introduction
Burn injuries are a global public health problem, and their epidemiology presents regional variations.1 Burns can result from several etiological agents, such as direct exposure to fire, chemicals, electrical current, radiation, or friction.2 Additionally, these injuries are a significant cause of death worldwide.1,2
The World Health Organization estimates that burns account for approximately 180,000 deaths annually.3 Infant mortality from burns is higher in lowand middle-income countries, being about seven times higher than that observed in high-income countries.3 These injuries are a severe issue, as the possible sequelae include scarring, physical limitations, or permanent damage,4 including deficits in fine motor skills or contractures when occurring near joints.5
Although burns are a significant global problem, the literature about their occurrence in Peru is scarce.6 This is worrisome, as understanding the epidemiology of burns is fundamental for public health planning and the development of potential interventions for Peru and Latin America. Therefore, we aimed to locate studies, describe bibliometric data, and define the epidemiological profile of burn patients in Peru through a systematic review.
Objectives
The primary objective of this study was to investigate the epidemiology of burns in Peru. Specific objectives included describing bibliometric data, identifying the locations of each study, synthesizing clinical and demographic data, and determining areas for further research.
Materials and Methods
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA).7 The Population, Exposure, Comparator, and Outcomes (PECO)8 strategy employed ‘Peru’ as the population and ‘burns’ as exposure, not including comparators or outcomes.
Inclusion criteria were the following: studies describing burn patients in Peru at any time period; in any language; cross-sectional, cohort, and case-control studies; conference proceedings, articles, and theses.
Exclusion criteria included incomplete studies or those lacking data from Peru. Also, randomized clinical trials, case series, case reports, and reviews were not considered.
We assessed the following four databases on March 9, 2023: Web of Science (WOS), Medline (PubMed), Embase, and the Virtual Health Library (VHL). There was no restriction on the year of publication, and we considered all articles published up to the time of access for screening. After article selection and reading, we reviewed their references to include new papers, the process was not repeated. We included “gray literature” studies9 because we noted that a part of the relevant literature was in conference proceedings and theses. We used the following terms for each database: “Burns”, “Electrical Burns”, “Ocular Burns”, “Inhalation Burns”, “Burn Treatment Units”, and “Peru”.
We saved the data in the Rayyan (Qatar Foundation) platform,10 a reference manager designed for review studies.11 Two independent researchers reviewed the studies, through a blinded process. The consensus of all researchers solved any disagreements. We searched for complete texts of studies without abstracts or incomplete articles. Studies that did not meet the inclusion criteria were removed from the analysis.
Two independent researchers extracted and evaluated the data, solving any differences by consensus. Other researchers performed a second review of the extraction, which used the online spreadsheet software Google Sheets (Google LLC.).12
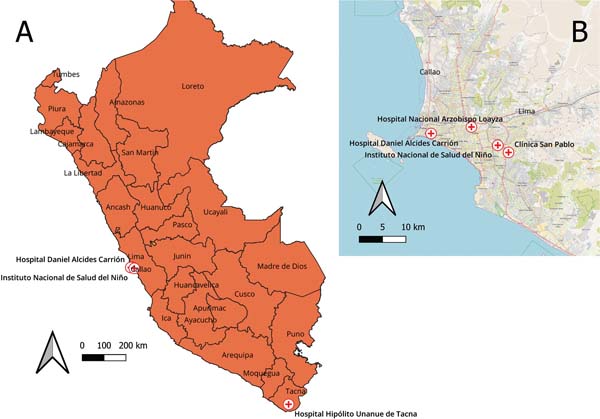
We obtained the coordinates of each hospital using the Google Maps (Google LLC.)13 and generated a map employing the QGIS (QGIS Development Team) software,14 which processed the locations of each study’s occurrence. These maps were based on OpenStreetMap (OSM Foundation)15 and the dataset from the United Nations Office for the Coordination of Humanitarian Affairs on the Humanitarian Data Exchange Database.16
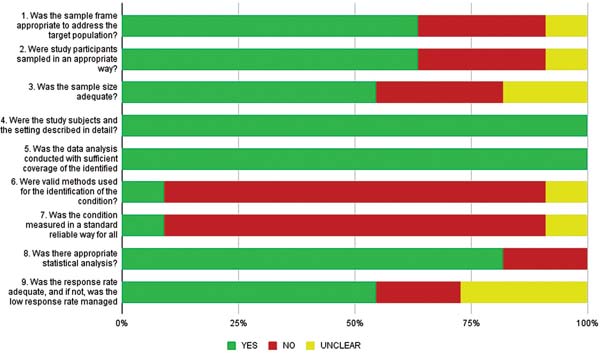
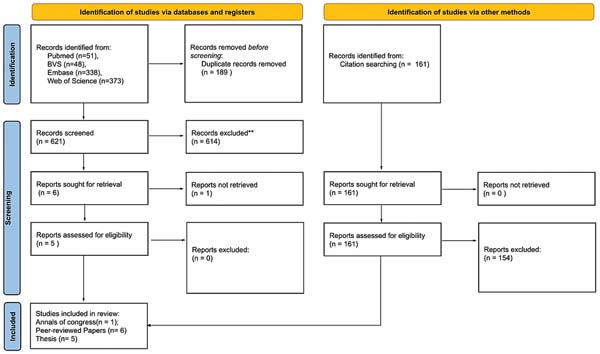
To assess the quality of the articles, two independent reviewers used the 9-item Joanna Briggs Institute (JBI) checklist.17 We did not apply the checklist to conference proceedings. We collected the infection criteria defined in each study. “Unclear” refers to information not provided or of a dubious nature.17 We created a flowchart following the PRISMA guidelines (►Fig. 1)7 and ►Fig. 2 summarizes the quality of the studies according to the JBI criteria.17


We performed the statistical analysis using the RStudio (Posit PBC) software’s18 meta19 and metafor20 packages. After extraction, we transposed data on the number of infections, deaths, and samples into the software to conduct the meta-analysis.21 We employed the inverse variance logit transformation (PLOGIT) method and a random-effects model. Using the Hartung-Knapp method, we adjusted the confidence intervals (CIs) of the combined effect to provide more conservative estimates.21
The I2 statistics assessed the heterogeneity between studies, and values above 50% indicated heterogeneity. We also calculated and evaluated the Tau-squared (τ2) values.21 We conducted subgroup analyses using Chi-squared (χ2) tests to assess whether there was a significant difference between subgroups (studies that did or did not perform laboratory testing for infections).21
Results
During the evaluation period, which extended up to March 9, 2023, we retrieved 971 records, including 810 from databases and 161 from citation searches. From the records retrieved from the databases, we excluded 189 duplicates. We screened the remaining 621 records, of which 614 were excluded for not meeting the inclusion criteria, resulting in 6 articles, of which 1 was not retrieved, and 5 underwent eligibility assessment. Among the records retrieved from citations, we included 7 in the analysis (►Fig. 1). The final sample consisted of 12 studies, including 1 conference abstract,6 peer-reviewed articles, and 5 theses (►Tables 1-3).1,6,22-31
| Study | Journal or repository | Study design | Year of publication | Peruvian journal (yes/no) | Hospital | City |
|---|---|---|---|---|---|---|
| Pediatric Burns at a Reference Burn Unit of a Middle-Income Country22 | Burn & Care Research | Cross-sectional | 2018 | Yes | Instituto Nacional de Salud del Niño | Lima |
| Risk factors for burns in children: crowding, poverty, and poor maternal education23 | Injury Prevention | Case-Control | 2002 | Yes | Instituto Nacional de Salud del Niño | Lima |
| Associated factors to the development of inhospital infections in adults with severe burns at a reference hospital in Peru. A five years study1 | Cirugía Plástica Ibero- Latinoamericana | Cohort | 2022 | Yes | Hospital Nacional Daniel Alcies Carrion, Callao | Lima |
| Factores asociados a la infección de las heridas por quemadura en pacientes quemados
mayores de 15 años en el Hospital Hipólito Unanue de Tacna periodo 2003- 2007 (Factors associated with the burn injury infection in burn patients over 15 years old
at Hospital Hipólito Unanue de Tacna from 2003 to 2007)24 |
Thesis (Repositorio Institucional UNJBG) | Case-Control | 2008 | NA | Hospital Hipólito Unanue de Tacna | Tacna |
| Asociación entre los factores de riesgo en quemaduras de III grado y la morbimortalidad
en pacientes gerontes en el Hospital Nacional Arzobispo Loayza en el año 2017 (Association between risk factors for thirddegree burns, morbidity, and mortality in
elderly patients at Hospital Nacional Arzobispo Loayza in 2017)25 |
Thesis (Repositorio Institucional de la Universidad Privada San Juan Bautista) | Cross-sectional | 2018 | NA | Hospital Nacional Arzobispo Loayza | Lima |
| Incidencia y factores asociados a la infección de heridas por quemadura en el Hospital
Hipólito Unanue de Tacna durante 2009-2013 (Incidence and factors associated with infection in burn wounds in the Hospital Hipólito
Unanue de Tacna from 2009 to 2013)26 |
Thesis (Repositorio Institucional UNJBG) | Cross-sectional | 2014 | NA | Hospital Hipólito Unanue de Tacna | Tacna |
| Prácticas seguras del cuidado de enfermería en los pacientes quemados en el servicio
de cirugía plástica y quemados - hospital Daniel Alcides Carrión - Callao 2015 / 2017
(Safe nursing care practices for burnt patients in the plastic and burn surgery service
- Daniel Alcides Carrión hospital, Callao, 2015 / 2017)27 |
Thesis (Repositorio Institucional UNAC) | Cross-sectional | 2018 | NA | Hospital Daniel Alcides Carrión | Callao |
| Relación entre la profundidad de la quemadura y la presencia de infecciones nosocomiales en los pacientes hospitalizados | Thesis (Repositorio Institucional UPC) | Cohort | 2019 | NA | Hospital Nacional Arzobispo Loayza | Lima |
| en el servicio de Quemados y Cirugía Plástica del Hospital Nacional Arzobispo Loayza,
periodo 2006-2016 (Relationship between the depth of the burn and the presence of nosocomial infections
in hospitalized patients in the Burn and Plastic Surgery service at Hospital Nacional
Arzobispo Loayza from 2006 to 2016) 28 |
||||||
| Caracteristicas Clinico-Epidemiologicas y patrones de prescpcion para quemaduras en
tres hospitales de Lima, Peru (Clinicalepidemiological characteristics and prescribing patterns for burns in three
hospitals in Lima, Peru)6 |
Revista Peruana de Medicina Experimental y Salud Pública | Cross-sectional | 2019 | No | Hospital Nacional Arzobispo Loayza; Hospital Nacional Daniel Alcides Carrión; Clínica San Pablo |
Lima |
| Características clínico epidemiológicas de los pacientes con quemaduras antes y durante
la pandemia por Covid-19 en el Instituto Nacional de Salud del Niño San Borja (Clinical epidemiological characteristics of patients with burns before and during
the covid 19 pandemic at the Instituto Nacional de Salud del Niño San Borja)29 |
Revista del Cuerpo Médico Hospital Nacional Almanzor Aguinaga Asenjo | Cross-sectional | 2023 | No | Instituto Nacional de Salud del Niño San Borja | Lima |
| Falls, poisonings, burns, and road traffic injuries in urban Peruvian children and adolescents: a community-based study30 | Injury Prevention | Cross-sectional | 2009 | Yes | Not applicable | Lima |
| Tratamiento del paciente quemado hospitalario durante las primeras 48 horas: análisis
de 36 casos en el Hospital Nacional Arzobispo Loayza (Treatment of the hospitallzed burned patient within the first 48 hours: analyses of 36 cases in the Hospital Nacional Arzobispo Loayza)31 |
Horizonte Médico | Cross-sectional | 2005 | No | Hospital Nacional Arzobispo Loayza | Lima |
Abbreviation: NA, not available.

| Study | Evaluated period | Participants (n) | Inclusion criteria | Burn Treatment Unit |
|---|---|---|---|---|
| Pediatric Burns at a Reference Burn Unit of a Middle-Income Country22 | September 2013 to August 2017 |
848 | Children ages 0-18 years admitted to a new pediatric intensive care unit in Lima, Peru | Yes |
| Risk factors for burns in children: crowding, poverty, and poor maternal education23 | 1998-2000 (14 months) | 720 | Subjects under 18-years-old who presented to the hospital with burns and underwent treatment from December 1998 to January 2000 | Yes |
| Associated factors to the development of in-hospital infections in adults with severe burns at a reference hospital in Peru. A five years study1 | 2014-2019 | 45 | Patients with severe burns whose medical records reported age, hypoalbuminemia, comorbidities, percentage of total body surface area burned, and location of the injury | NA |
| Factores asociados a la infección de las heridas por quemadura en pacientes quemados
mayores de 15 años en el Hospital Hipólito Unanue de Tacna periodo 2003-2007 (Factors associated with the burn injury infection in burn patients over 15 years old
at Hospital Hipólito Unanue de Tacna from 2003 to 2007)24 |
2003-2007 | 120 | Subjects from both sexes, over 15 years old, with any burn whose treatment required hospitalization in the Surgery Services and/or SERCIQUEM of the Hospital Hipólito Unanue in Tacna from 2003 to 2007; hospitalized patients discharged as recovered or deceased; burned patients with medical records containing all the data required for the study. | Yes |
| Asociación entre los factores de riesgo en quemaduras de III grado y la morbi-mortalidad
en pacientes gerontes en el Hospital Nacional Arzobispo Loayza en el año 2017 (Association between risk factors for third-degree burns, morbidity, and mortality
in elderly patients at Hospital Nacional Arzobispo Loayza in 2017)25 |
2017 | 48 | Patients receiving treatment at Hospital Arzobispo Loayza, whose medical records clearly reported the different variables mentioned in the study, aged 65 or older, and diagnosed with third-degree burns in 2017. | No |
| Incidencia y factores asociados a la infección de heridas por quemadura en el Hospital
Hipólito Unanue de Tacna durante 2009-2013 (Incidence and factors associated with infection in burn wounds in the Hospital Hipólito Unanue de Tacna from 2009 to 2013)26 |
January 2009 to December 2013 |
350 | Patients admitted to the SERCIQUEM Service due to burn injuries from January 1, 2009, to December 31, 2013. Patients of any age, of both sexes, with a diagnosis of burns and signs of burn wound infection, confirmed by secretion culture. | No |
| Prácticas seguras del cuidado de enfermería en los pacientes quemados en el servicio
de cirugía plástica y quemados - hospital Daniel Alcides Carrión - Callao 2015 / 2017
(Safe nursing care practices for burnt patients in the plastic and burn surgery service
- Daniel Alcides Carrión hospital, Callao, 2015 / 2017)27 |
2015-2017 | 99 | Patients admitted to the specialized surgery department at Daniel Alcides Carrión Hospital due to burns. | Yes |
| Relación entre la profundidad de la quemadura y la presencia de infecciones nosocomiales en los pacientes hospitalizados en el servicio de Quemados y Cirugía Plástica del Hospital Nacional Arzobispo Loayza, periodo 2006-2016 (Relationship | 2006-2016 | 131 | Patients with secondand third-degree burns occurring within 48 hours before hospitalization, with no signs of infection at admission. | Yes |
| between the depth of the burn and the presence of nosocomial infections in hospitalized patients in the Burn and Plastic Surgery service at Hospital Nacional Arzobispo Loayza from 2006 to 2016)28 | ||||
| Caracteristicas Clinico-epidemiologicas y patrones de prescpcion para quemaduras en tres hospitales de Lima, Peru (Clinical-epidemiological characteristics and prescribing patterns for burns in three hospitals in Lima, Peru)6 | March 2014 to April 2016 | 561 | Patients of both sexes, aged 18-80 years, with an initial diagnosis of firstor second-degree, or both burns, undergoing treatment in immediate care centers (including the emergency service of the same hospital or others, clinics, health centers, private practices, pharmacies, and home [self-medication]) and specialized burn units of the hospital centers participating in the study. | Yes |
| Características clínico Epidemiológicas de los pacientes con quemaduras antes y durante
la pandemia por Covid-19 en el Instituto Nacional de Salud del Niño San Borja (Clinical epidemiological characteristics of patients with burns before and during
the covid 19 pandemic at the Instituto Nacional de Salud del Niño San Borja)29 |
March 2019 to December 2020 |
278 | Patients with a diagnosis of burns undergoing treatment at INSNSB Patients under 17-years and 11-months-old |
No |
| Falls, poisonings, burns, and road traffic injuries in urban Peruvian children and adolescents: a community-based study30 | January to August 2005 | 210 | Eligibility for the study required a consenting adult and at least one child aged 18 years living in the household. | No |
| Tratamiento del paciente quemado hospitalario durante las primeras 48 horas: análisis
de 36 casos en el Hospital Nacional Arzobispo Loayza (Treatment of the hospitallzed burned patient within the first 48 hours: analyses of 36 cases in the Hospital Nacional Arzobispo Loayza)31 |
January to December 2001 | 36 | Admission to Hospital Nacional Arzobispo Loayza via the Emergency Service. Patients
with second-degree burns affecting 20% or more of the body surface with any location. Patients with second-degree and third-degree burns affecting 2 to 10% of the body surface in specific sites (face, hands, genitals and perineum). Patients with thirdor fourth-degree burns anywhere comprising more than 10% of the body surface. Patients with first-degree burns exceeding 90% of the body surface. Patients with inhalation injury; with burns resulting from specific agents (electricity, chemicals); with tetanus vaccination; and those aged over 14-years-old. |
Yes |
Abbreviation: NA, not available.

As shown in ►Fig. 2, while the descriptions of subjects and settings were strong (items 4 and 5), two studies lacked clarity regarding their sampling methods, as they relied on convenience samples or failed to calculate sizes correctly (items 1-3). Clinical assessments may differ among physicians, and the studies did not use clear guidelines for evaluation (items 6 and 7). Furthermore, some studies failed to specify the criteria used for evaluating burns and infections. Although most of them focused on data description, bivariate and multivariate analyses were adequate, and reported proportions. Only two studies investigating infections did not use multivariate adjustment (item 8). The response rate was not described or was inadequate in five studies, with a response rate below 80% (item 9). ►Table 4 shows the evaluation of each study.1,6,22-31
| Study | Most affected sex | Most affected age (years) | Most common etiology | Most common affected area | Most common place of burn occurrence |
|---|---|---|---|---|---|
| Pediatric Burns at a Reference Burn Unit of a Middle-Income Country22 | Male (n = 424) | 1-4(n = 509) | Hot fluids (n = 519) | NA | NA |
| Risk factors for burns in children: crowding, poverty, and poor maternal education23 | Male (n = 398) | 0-4(n = 502) | Hot fluids (n = 535) | NA | Home(n = 558) |
| Associated factors to the development of in-hospital infections in adults with severe burns at a reference hospital in Peru. A five years study1 | Male(n = 29) | NA | Direct fire (n = 32) | Limbs (n = 45) | NA |
| Factores asociados a la infección de las heridas por quemadura en pacientes quemados
mayores de 15 años en el Hospital Hipólito Unanue de Tacna periodo 2003-2007 (Factors associated with the burn injury infection in burn patients over 15 years old
at Hospital Hipólito Unanue de Tacna from 2003 to 2007)24 |
Male(n = 61) | 15-24 (n = 31) |
Hot fluids (n = 58) | Upper limbs (n = 55) | NA |
| Asociación entre los factores de riesgo en quemaduras de III grado y la morbimortalidad
en pacientes gerontes en el Hospital Nacional Arzobispo Loayza en el año 2017 (Association between risk factors for third-degree burns, morbidity, and mortality in elderly patients at Hospital Nacional Arzobispo Loayza in 2017)25 |
Male(n = 34) | NA | Hot fluids (n = 36) | Legs(n = 18) | Home (n = 38) |
| Incidencia y factores asociados a la infección de heridas por quemadura en el Hospital
Hipólito Unanue de Tacna durante 2009-2013 (Incidence and factors associated with infection in burn wounds in the Hospital Hipólito
Unanue de Tacna from 2009 to 2013)26 |
Male (n = 194) | < 10 (n = 190) | Hot fluids (n = 225) | Upper limbs (n = 146) | Home(n = 282) |
| Prácticas seguras del cuidado de enfermería en los pacientes quemados en el servicio
de cirugía plástica y quemados - hospital Daniel Alcides Carrión - Callao 2015 / 2017
(Safe nursing care practices for burnt patients in the plastic and burn surgery service
- Daniel Alcides Carrión hospital, Callao, 2015 / 2017)27 |
Male(n = 62) | NA | NA | Upper limbs (n = 08) | NA |
| Relación entre la profundidad de la quemadura y la presencia de infecciones nosocomiales
en los pacientes hospitalizados en el servicio de Quemados y Cirugía Plástica del
Hospital Nacional Arzobispo Loayza, periodo 2006-2016 (Relationship between the depth of the burn and the presence of nosocomial infections
in hospitalized patients in the Burn and Plastic Surgery service at Hospital Nacional Arzobispo Loayza from 2006 to 2016)28 |
Male(n = 84) | NA | Direct fire (n = 89) | Upper limbs (n = 105) | NA |
| Caracteristicas Clinico-Epidemiologicas y patrones de prescpcion para quemaduras en
tres hospitales de Lima, Peru (Clinicalepidemiological characteristics and prescribing patterns for burns in three hospitals in Lima, Peru)6 |
Female (n = 324) | NA | Hot fluids (n = 284) | Face (n = 161) | Home(n = 344) |
| Características clínico Epidemiológicas de los pacientes con quemaduras antes y durante
la pandemia por Covid-19 en el Instituto Nacional de Salud del Niño San Borja (Clinical epidemiological characteristics of patients with burns before and during
the covid 19 pandemic at the Instituto Nacional de Salud del Niño San Borja)29 |
Male (n = 168) | Infant(n = 110) | Hot fluids (n = 221) | Thorax (n = 131) | Home(n = 252) |
| Falls, poisonings, burns, and road traffic injuries in urban Peruvian children and adolescents: a community-based study30 | Male (n = 108) | 1-4(n = 120) | Hot fluids (n = 156) | NA | Home(n = 199) |
| Tratamiento del paciente quemado hospitalario durante las primeras 48 horas: análisis
de 36 casos en el Hospital Nacional Arzobispo Loayza (Treatment of the hospitallzed burned patient within the first 48 hours: analyses of 36 cases in the Hospital Nacional Arzobispo Loayza)31 |
Male(n = 21) | NA | Hot fluids (n = 9) | Lower limbs (n = 25) | NA |
Abbreviation: NA, not available.

| Study | Checklist from the JBI17 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| Factores asociados a la infección de las heridas por quemadura en pacientes quemados
mayores de 15 años en el Hospital Hipólito Unanue de Tacna periodo 2003- 2007 (Factors associated with the burn injury infection in burn patients over 15 years old
at Hospital Hipólito Unanue de Tacna from 2003 to 2007)24 |
Yes | Yes | Yes | Yes | Yes | No | No | No | Yes |
| Associated factors to the development of inhospital infections in adults with severe burns at a reference hospital in Peru. A five years study1 | No | No | No | Yes | Yes | No | No | No | No |
| Risk factors for burns in children: crowding, poverty, and poor maternal education23 | Yes | Yes | Unclear | Yes | Yes | No | No | Yes | Yes |
| Asociación entre los factores de riesgo en quemaduras de III grado y la morbimortalidad
en pacientes gerontes en el Hospital Nacional Arzobispo Loayza en el año 2017 (Association between risk factors for thirddegree burns, morbidity, and mortality in
elderly patients at Hospital Nacional Arzobispo Loayza in 2017)25 |
Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes |
| Incidencia y factores asociados a la infección de heridas por quemadura en el Hospital
Hipólito Unanue de Tacna durante 2009-2013 (Incidence and factors associated with infection in burn wounds in the Hospital Hipólito Unanue de Tacna from 2009 to 2013)26 |
Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes |
| Prácticas seguras del cuidado de enfermería en los pacientes quemados en el servicio
de cirugía plástica y quemados - hospital Daniel Alcides Carrión - Callao 2015 / 2017
(Safe nursing care practices for burnt patients in the plastic and burn surgery service
- Daniel Alcides Carrión hospital, Callao, 2015 / 2017)27 |
Unclear | Unclear | Unclear | Yes | Yes | Unclear | Unclear | Yes | Unclear |
| Relación entre la profundidad de la quemadura y la presencia de infecciones nosocomiales
en los pacientes hospitalizados en el servicio de Quemados y Cirugía Plástica del
Hospital Nacional Arzobispo (Relationship between the depth of the burn and the presence of nosocomial infections
in hospitalized patients in the Burn and Plastic Surgery service at Hospital Nacional Arzobispo Loayza from 2006 to 2016)28 |
Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes |
| Características clínico-epidemiológicas y patrones de prescripción para quemaduras
en tres hospitales de Lima, Perú (Clinicalepidemiological characteristics and prescribing patterns for burns in three hospitals in Lima, Peru)6 |
No | No | No | Yes | Yes | No | No | Yes | Yes |
| Características clínico Epidemiológicas de los pacientes con quemaduras antes y durante
la pandemia por Covid-19 en el Instituto Nacional de Salud del Niño San Borja (Clinical epidemiological characteristics of patients with burns before and during
the covid 19 pandemic at the Instituto Nacional de Salud del Niño San Borja)29 |
Yes | Yes | Yes | Yes | Yes | No | No | Yes | Unclear |
| Falls, poisonings, burns, and road traffic injuries in urban Peruvian children and adolescents: a community based study30 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No |
| Tratamiento del paciente quema do hospitalario durante las primeras 48 horas: análisis
de 36 casos en el Hospital Nacional Arzobispo Loayza (Treatment of the hospitallzed burned patient within the first 48 hours: analyses of 36 cases in the Hospital Nacional Arzobispo Loayza)31 |
No | No | No | Yes | Yes | No | No | Yes | Unclear |
Abbreviation: JBI, Joanna Briggs Institute.

The present review included a total of 3,446 patients from 12 studies, as detailed in ►Table 2. Sample sizes varied considerably across studies, ranging from 36 to 848 participants. The most prevalent age group differed among studies, as each adopted specific inclusion criteria. However, children were consistently identified as the group most affected by burns.
Regarding sex, men were the most affected, and the most common location for burn occurrence was in a domestic setting. As for etiology, the most common cause was contact with hot fluids, followed by direct fire. The limbs were the most frequently affected body parts. Only two studies29,31 reported the average percentage of body surface area burned: the lowest average was 10.23%29 and the highest, 17.7%.31
Most studies occurred in hospitals in Lima, and seven studies described burn units, with the primary hospital being Hospital Nacional Arzobispo Loayza. The mapin ►Fig. 3 shows the locations of the hospitals.

The pooled rate of infections was 31.7% (95%CI: 21.46- 44.08%; I2 = 0%) among studies that did not use laboratory tests,1,24,25 without significant heterogeneity. Among studies that used tests,26,28 the pooled rate of infections was lower (7.74%), with a significant heterogeneity (I2 = 94.2%). Studies using laboratory tests or not differed significantly (χ2 = 4.80, p < 0.03).
Only five studies described the number of deaths among patients. Two studies did not report deaths during the evaluation period.24,25 Cutipa et al.26 included 350 patients and recorded five deaths. Sam et al.29 analyzed 278 cases, with four deaths. In contrast, Chávez et al.28 despite presenting the smallest sample (131 patients), reported 8 deaths. The analysis of deaths revealed a pooled rate of 1.88% (95%CI: 0.54-6.36%; I2 = 67.1%), with significant heterogeneity.
We did not consider COVID-19 infections.29 Also, despite describing 26 deaths in 1999, Delgado et al.23 did not report the population at risk in the same year. As such, we did not include their study in this meta-analysis.
The publication of all studies, original articles, and theses occurred from 2002 to 2023 (►Table 2). Non-Peruvianjournals published half of the articles, with two in “Injury Prevention” and one in “Cirugía Plástica Ibero-Latinoamericana”. The theses were not subsequently published as articles.
Discussion
This study synthesized bibliometric and epidemiological characteristics and presented results consistent with those from other epidemiological studies regarding the etiology, location, and demographics of burns.32,33 Although age is an essential demographic data, its comparative analysis had limitations due to heterogeneous inclusion criteria, lack of uniform etiological stratification, and use of different age ranges among the included studies, suggesting a point of improvement.
A study involving 8 centers in Africa, Asia, and Latin America (n = 15,344) revealed that the most common etiology of burns was hot fluids and flames, most frequently occurring at home, and in males.32 A scoping review of 40 studies on burns in Africa showed that the key etiology was scalding, and most patients were males.33 However, these data diverge from the Global Burn Registry (n = 9,277), which showed that burns were more frequent in the domestic environment, with a greater number of female victims and flames as etiology.34
Some studies addressing infections did not report on the method used for their identification. The meta-analysis showed a higher infection rate in studies that did not use laboratory tests. Among the studies that used laboratory tests,infection criteria can explain thedifferences;one included only wound infections,26 while the other included any type.28 Culture methods are more reliable, should be used whenever possible. Different inclusion criteria and study designs can explain the heterogeneity in mortality rates.
The number of published studies is scarce, and most are in Peruvian journals. Moreover, there was no publication of theses as articles upon completion. This fact may suggest a low level of engagement among researchers in investigating the topic and a problem within publications, as global journals may not be interested in publishing data from the country. A literature review of burn studies on PubMed showed that Peru had no first or senior authors in global publications. Meanwhile, Brazil was the leading country in Latin America, and the United States was the leading country in the Americas.35 In this context, calls for papers targeting Latin American countries are critical for the development of studies in Peru and the greater visibility of regional data.
Overall, the analysis showed the scarcity of Peruvian literature. In terms of geographic distribution, studies generally focus on a single region, with only one survey study. Therefore, the accurate understanding of burn occurrence in Peru is complex, particularly because other areas differ in their economic development and population size. Additionally, these less developed regions have the highest risk of burns.35 Survey studies, involving questionnaires and multicenter designs, can offer a better understanding of regions lacking hospital data.
The studies included in this analysis are valuable sources for understanding the epidemiology of burns in the Peruvian context, as they explore and report relevant aspects of the local reality and integrate a body of literature that deserves global attention. However, since they are mainly observational studies, it is worth noting some methodological limitations: (1) most occurred in a single hospital center, with varying inclusion criteria and reporting methods, making direct comparisons difficult; (2) regarding data quality, collection based on clinical records is subject to information bias; (3) clinical assessment can vary among professionals, resulting in an heterogenous patient classification and management.
Therefore, future multicenter studies should prioritize the standardization of clinical and methodological criteria in their protocols to improve the comparability and robustness of the data generated. The use of previous studies as a starting point is essential.
Conclusion
Although heterogeneous, the studies reveal fundamental data consistent with the epidemiology described in the literature. Based on these data, subsequent stages of studies in Peru should prioritize cooperation between geographically close centers, to optimize logistics and facilitate multicenter research. Moreover, in peripheric areas, the application of survey research (questionnaires) can significantly contribute to a deeper understanding of local epidemiology.
References
1. Hernández-Patiño I, Blas-Mas S, Burgos J, De la Crus-Vargas J. Factores asociados a infección intrahospitalaria en adulto gran quemado en hospital de referencia peruano. Estudio de 5 años. Cir Plást Ibero-Latinoam 2022;48(03):347-354. Doi: 10.4321/s0376-78922022000300012
2. Jeschke MG, van Baar ME, Choudhry MA et al. Burn injury. Nat Rev Dis Primers 2020;6(11):.Doi:10.1038/s41572-020-0145-5
3. World Health Organization. Burns. Geneva: World Health Organization; 2023 [cited 2024 May 3]. Available from: https://www.who.int/news-room/fact-sheets/detail/burns
4. Barba P, Neubauer DC, Cossa M, et al. Prevalence and Severity of Burn Scars in Rural Mozambique. World J Surg 2022;46(11): 2561-2569. Doi: 10.1007/s00268-022-06682-y
5. Zhu Z, Kong W, Wang H, et al. Prevalence and predictors of scar contracture-associated re-hospitalisation among burn inpatients in China. Sci Rep 2021;11(01):14973. Doi: 10.1038/s41598-021-94432-w
6. Cecchi GMW, Hidalgo ER, Orrillo JVC, Muñoz JRL, Medina CA. [Clinical-epidemiological characteristics and prescribing patterns for burns in three hospitals in Lima, Peru]. Rev Peru Med Exp Salud Publica 2019;36(01):68-73. Doi: 10.17843/ rpmesp.2019.361.3649
7. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018;169(07):467-473. Doi: 10.7326/M18-0850
8. Morgan RL, Whaley P, Thayer KA, Schünemann HJ. Identifying the PECO: A framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ Int 2018;121(Pt 1):1027-1031. Doi: 10.1016/j. envint.2018.07.015
9. Lefebvre C, Glanville J, Briscoe S, et al; Cochrane Information Retrieval Methods GroupChapter 4: Searching for and selecting studies. In:Higgins JPT, Thomas J, Chandler J, et al. , editors. Cochrane Handbook for Systematic Reviews of Interventions, version 6.5.1. London: The Cochrane Collaboration; 2025 [cited 2025 May 26]. Available from: https://training.cochrane.org/handbook/current/chapter-04
10. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev 2016;5(01): 210. Doi: 10.1186/s13643-016-0384-4
11. Qatar Computing Research Institute. Rayyan - Intelligent Systematic Review. Rayyan, 2021 [cited 2024 May 3]. Available from: https://www.rayyan.ai/
12. Google LLC. Google Sheets. Mountain View: Google LLC;. 2024 [cited 2024 Jul 10]. Available from: https://workspace.google.com/products/sheets/
13. Google LLC. Google Maps. Mountain View: Google LLC,. 2024 [cited 2024 Jul 10]. Available from: https://www.google.com/maps
14. QGIS Development Team. QGIS Geographic Information System. Grüt, Switzerland: QGIS.ORG; 2024 [cited 2024 May 3]. Available from: https://www.qgis.org/es/site/
15. OpenStreetMap Foundation. OpenStreetMap database. Cambridge: OpenStreetMap Foundation; 2021. Available from: https://www.openstreetmap.org
16. Humanitarian Data Exchange. Peru - Subnational Administrative Boundaries. Humanitarian Data Exchange. Published2015, April 12. Updated 2023, July 24. [cited 2024 May 3]. Available from: https://data.humdata.org/dataset/cod-ab-per
17. Moola S, Munn Z, Tufanaru C, et al. Chapter 7: Systematic Reviews of Etiology and Risk. In: Aromataris E, Munn Z, editor. Joanna Briggs Institute Reviewer’s Manual. Adelaide: Joanna Briggs Institute; 2017. Doi: 10.46658/jbirm-17-06
18. Posit PBC. RStudio IDE - The most trusted IDE for open source data science. Boston: Posit Software PBC; 2025. Available from: https://posit.co/products/open-source/rstudio/
19. Balduzzi S, Rücker G, Schwarzer G. How to perform a metaanalysis with R: a practical tutorial. Evid Based Ment Health 2019;22(04):153-160. Doi: 10.1136/ebmental-2019-300117
20. Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Softw 2010;36(03):1-48. Doi: 10.18637/jss.v036. i03
21. Deeks JJ, Higgins JPT, Altman DG, McKenzie JE, Veroniki AA; Cochrane Statistical Methods Group. Chapter 10: Analysing data and undertaking meta-analyses. In: Higgins JPT, Thomas J, Chandler J, et al. , editors. Cochrane Handbook for Systematic Reviews of Interventions, version 6.4 (updated August 2023). London: The Cochrane Collaboration; 2023. Available from: https://training.cochrane.org/handbook/current/chapter-10
22. Huby M, Medina-Pflucker M. 285 Pediatric Burns at a Reference Burn Unit of a Middle Income Country. J Burn Care Res 2018;39 (Suppl 1):S111. Doi: 10.1093/jbcr/iry006.207
23. Delgado J, Ramírez-Cardich ME, Gilman RH, et al. Risk factors for burns in children: crowding, poverty, and poor maternal education. Inj Prev 2002;8(01):38-41. Doi: 10.1136/ip.8.1.38
24. Centeno JC. Factores asociados a la infección de las heridas por quemadura en pacientes quemados mayores de 15 años en el Hospital Hipólito Unanue de Tacna periodo 2003-2007. [thesis (Escuela Académico Profesional de Medicina Humana)] Tacna: Facultad de Ciencias Médicas, Universidad Nacional Jorge Basadre Grohmann; 2008
25. Montalvo V, Jhonatan S. Asociación entre los factores de riesgo en quemaduras de III grado y la morbi-mortalidad en pacientes gerontes en el Hospital Nacional Arzobispo Loayza en el año 2017. [thesis (Escuela Profesional de Medicina Humana)] Lima: Facultad de Ciencias de la Salud, Universidad Privada San Juan Bautista; 2017
26. Cutipa H, María A. Incidencia y factores asociados a la infección de heridas por quemadura en el Hospital Hipólito Unanue de Tacna durante 2009-2013. [thesis (Escuela Académico Profesional De Medicina Humana)] Tacna: Facultad de Ciencias de la Salud, Universidad Nacional Jorge Basadre Grohmann; 2014
27. Salas S, Giovanna L. Prácticas seguras del cuidado de enfermería en los pacientes quemados en el servicio de cirugía plástica y quemados - Hospital Daniel Alcides Carrión - Callao 2015/2017. [thesis (Escuela Profesional de Enfermería)] Callao: Facultad de Ciencias de la Salud, Universidad Nacional del Callao; 2018
28. Chávez KPT, Alcántara AT. Relación entre la profundidad de la quemadura y la presencia de infecciones nosocomiales en los pacientes hospitalizados en el servicio de Quemados y Cirugía Plástica del Hospital Nacional Arzobispo Loayza, período 2006-2016. [thesis, Programa Académico de Medicina] Lima: Facultad de Ciencias de la Salud, Universidad Peruana de Ciencias Aplicadas; 2019
29. Sam AVY, Padilla EB, Sedano CS. Características clínico Epidemiológicas de los pacientes con quemaduras antes y durante la pandemia por Covid-19 en el Instituto Nacional de Salud del Niño San Borja. Rev Cuerpo Med HNAAA 2024;16(01):78-82. Doi: 10.35434/rcmhnaaa.2023.161.1661
30. Donroe J, Gilman RH, Brugge D, Mwamburi M, Moore DAJ. Falls, poisonings, burns, and road traffic injuries in urban Peruvian children and adolescents: a community based study. Inj Prev 2009;15(06):390-396. Doi: 10.1136/ip.2008.019893
31. Heresi OP. Tratamiento del paciente quemado hospitalario durante las primeras 48 horas: análisis de 36 casos en el Hospital Nacional Arzobispo Loayza . Horiz Méd 2005;5(02):1-11 Available from: https://www.redalyc.org/articulo.oa?id=371637113005
32. Quinn L, Ahmed T, Falk H, et al. Burn Admissions Across Lowand Middle-income Countries: A Repeated Cross-sectional Survey. J Burn Care Res 2023;44(02):320-328. Doi: 10.1093/jbcr/irac096
33. Mukagaju F, Velin L, Miranda E, et al. What is Known About Burns in East Africa? A Scoping Review. J Surg Res 2021;266:113-124. Doi: 10.1016/j.jss.2021.03.055
34. Ladhani HA, Yowler CJ, Claridge JA. Burn Wound Colonization, Infection, and Sepsis. Surg Infect (Larchmt) 2021;22(01):44-48. Doi: 10.1089/sur.2020.346
35. Wall SL, Velin L, Abbas A, et al. Who tells the story of burns in lowand-middle income countries? - A bibliometric study. Burns 2023;49(04):854-860. Doi: 10.1016/j.burns.2022.06.003
36. Bahnsawy NSM, Mohammed AR, Ibrahim H, Younis RAA. Risk Factors Associated with Wound Infections in Burned Children. Malays J Nurs MJN. 2023;14(04):100-109. Doi: 10.31674/ mjn.2023.v14i04.011
1. Faculdade de Medicina de Catanduva (FAMECA), Centro Universitário Padre Albino,
Catanduva, SP, Brazil
2. Research Group in Plastic Surgery, Faculdade de Medicina de Catanduva (FAMECA),
Centro Universitário Padre Albino, Catanduva, SP, Brazil
3. Escuela de Medicina Humana, Facultad de Ciencias de la Salud, Universidad San Martín
de Porres, Lima, Peru
4. Escuela de Medicina Humana, Facultad de Ciencias de la Salud, Universidad Científica
del Sur, Lima, Peru
5. Department of Plastic Surgery, Faculdade de Medicina de Catanduva (FAMECA), Centro
Universitário Padre Albino, Catanduva, SP, Brazil
Address for correspondence Wilson Falco Neto, Faculdade de Medicina de Catanduva (FAMECA), Centro Universitário Padre Albino, Catanduva, São Paulo, 15809-144, Brazil (e-mail: wilson.academic.mail@gmail.com).
Artigo submetido: 27/03/2025.
Artigo aceito: 14/07/2025.
Conflict of Interests
The authors have no conflict of interests to declare.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket