



Original Article - Year 2020 - Volume 35 -
Trend in hospitalization for burns in Santa Catarina in the Single Health System, Brazil, in the period 2008-2018
Tendência de internação hospitalar por queimadura em Santa Catarina no Sistema Único de Saúde, Brasil, no período entre 2008 e 2018
Felipe Oliveira Duarte1,* ; Stefany Goudzenko Hernandez2; Marcos Oliveira Machado2; Jorge Bins Ely3
; Stefany Goudzenko Hernandez2; Marcos Oliveira Machado2; Jorge Bins Ely3
ABSTRACT
Introduction: Burns are defined as important lesions to the skin or organic tissue caused by electricity, chemical, radioactive agents, friction or friction, exposure, or contact with extreme heat or cold.
Methods: Ecological study of time series, with data obtained in the state of Santa Catarina, using the Hospital Information System of the Unified Health System database, from 2008 to 2018. For each year of the studied period, the hospitalization rates for burns were calculated, grossly and specifically, according to the dependent variables of interest: age group and sex. It was used the simple linear regression method for the analysis of temporal trends and standardized morbidity coefficients.
Results: There were 9,158 hospitalizations in the studied period. At the beginning of the period, the hospital admission rate was 12.06/100,000 inhabitants, ending the period with an increase to 17.07/100,000 inhabitants. In males, the rate started with 14.52/100,000, ending the historical series with 22.51/100,000 inhabitants. For women, the initial rate was 9.52/100,000 and, at the end of the period, increased to 11.72/100,000. The age group most affected in both sexes was 0 to 4 years.
Conclusion: There was an increase in the general hospitalization rate. The male sex presented higher rates in the period, but both sexes tended to increase. The age group from 0 to 4 years old stood out as the most affected in the state of Santa Catarina.
Keywords: Burns; Hospitalization; Epidemiology; Morbidity; Surgery, Plastic.
RESUMO
Introdução: Queimaduras são definidas como importantes lesões da pele ou tecido
orgânico, causadas por eletricidade, agentes químicos, radioativos, atrito
ou fricção, exposição ou contato com calor ou frio extremo.
Métodos: Estudo ecológico de séries temporais, com dados obtidos no estado de Santa
Catarina, utilizando o banco de dados do Sistema de Informações Hospitalares
do Sistema Único de Saúde, no período de 2008 a 2018. Para cada ano do
período estudado, foram calculadas as taxas de internação por queimadura,
bruta e específicas, de acordo com as variáveis dependentes de interesse:
faixa etária e sexo. Para análise das tendências temporais, foram utilizados
os coeficientes de morbidade padronizados e o método de regressão linear
simples.
Resultados: Ocorreram 9.158 internações no período estudado. A taxa de internação
hospitalar no início do período, foi de 12,06/100.000 habitantes;
finalizando o período com aumento para 17,07/100.000 habitantes. No sexo
masculino, a taxa iniciou com 14,52/100.000, finalizando a série histórica
com 22,51/100.000 habitantes. Já no sexo feminino, a taxa inicial foi de
9,52/100.000 e, ao final do período, aumentou para 11,72/100.000. A faixa
etária mais acometida em ambos os sexos foi a de 0 a 4 anos.
Conclusão: Houve aumento na taxa de internação geral. O sexo masculino apresentou taxas
superiores no período, mas ambos os sexos tenderam ao aumento. Destacou-se a
faixa etária dos 0 a 4 anos como a mais acometida no estado de Santa
Catarina.
Palavras-chave: Queimaduras; Hospitalização; Epidemiologia; Morbidade; Cirurgia plástica
INTRODUCTION
Burns are defined as important lesions to the skin or organic tissue caused by electricity, chemical, radioactive agents, friction or friction, exposure or contact with extreme heat or cold. They can be classified, in terms of depth, as first-degree, when the lesions reach only the epidermal layer; second-degree, when there is the involvement of the epidermis and the superficial or deep dermis layer; and, third-degree, when there are lesions of all the skin appendages1.
Factors associated with burn injuries are considered: low income, urban area, home environment, and the handling of hot liquids2. Among children, the age of one to three years is more prevalent in accidents associated with neuropsychomotor development and greater freedom of movement3. In elderly patients, in addition to injuries that occur in the kitchen, they also happen in the bathroom, related to excessively hot bath4.
Several complications can occur in burn patients, including infection of the lesion, pneumonia, acute renal failure, shock, and sepsis5. Among the hospitalized patients, 35.8% develop skin infections and 24.4% respiratory infections, with the elderly being the most affected6.
Treatment of burn victims is costly for the state and the patient. The average stay of major burns in a hospital environment is 41.5 days, with the body surface burned directly related to gravity, causing a great economic and emotional impact7. The final average cost of this type of patient can reach R$ 26,386.22, including grafts, debridement, and time spent in the Single Health System (SUS in Portuguese)8.
Patients face many challenges after hospital discharge, such as social stigmas due to the injury, which reduces the possibility of the patient returning to his economic potential. Another difficulty is that the mobility of the affected area, as the surface of the burned area can cause mobility difficulties in the affected region with permanent sequelae9.
Currently, there is a trend in the world to decrease the incidence of burn cases, the degree of mortality, the duration of hospital stays, and the severity10. In Brazil, the epidemiological profile of the adult patient who suffers burns is predominantly male, with an average age of 25 to 26 years, injured by flammable products in their own home. The majority of incidents occur in the upper extremities, and most are either first degree only or first and second degree combined. Second- and third-degree scald burns predominate on children, mainly on the trunk and upper limbs11.
In the south of Brazil, there have been small variations in the rates of hospitalization of burns in recent years (13.11 to 14.6/100,000 inhabitants), being higher in males and the 0-19 age group (Favassa et al., in 2017)12. The state of Paraná stands out in the region, which has higher rates compared to other states12. In Santa Catarina (SC), from 2006 to 2012, there was a significant decrease in the rate (from 15 to 10/100,000 inhabitants). The group most affected in the state is one to four years of age, with the hospitalization rate inversely proportional to age13.
The accomplishment of a higher number of national scientific, technical studies on the epidemiology of burns is necessary and desired14. The provision of new data, even public knowledge, but through research, is essential for the responsible agencies to develop effective prevention methods, based on the studied local population15. Therefore, this study’s objective was to analyze the time series of hospitalization rates for burns in the state of SC, according to sex and age group, in order to provide peculiar and relevant information for the design of public policies. The purpose is to promote and protect collective health concerning burns that are a significant cause of morbidity and mortality in the Brazilian population.
OBJECTIVE
This study’s general objective is to analyze the time trend for hospitalization due to burns in Santa Catarina from 2008 to 2018. The specific objectives are: to identify the general rate of hospitalization due to burns and to evaluate the tendency of the time series according to sex and range age by sex.
METHODS
An ecological time-series study was carried out using data obtained in the state of Santa Catarina in the public domain database of the Hospital Information System of the Unified Health System (SIH-SUS)16.
The study population was extracted from SIH-SUS hospital admissions data for burns in the state of Santa Catarina, which occurred from 2008 to 2018. Data inclusion was performed considering the International Classification of Disease ICD-10 in the case of burns and corrosion: T20 to T32. Hospitalization data with ignored sex or age were excluded. During the study period, the estimated population of burns was 4,480,073, according to SIH-SUS17.
Data collection was performed based on information in the public domain database on the DATASUS website, from the SUS Hospital Information System (SIH-SUS), available at http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sih/cnv/niuf.def. Hospital units affiliated with SUS sent data on admissions made through the Hospitalization Authorization (AIH) to municipal and state managers. The data were exported in Comma Separated Values (CVC) format and saved in an Excel spreadsheet.
Population demographic information was taken from the Instituto Brasileiro de Geografia e Estatística (IBGE) website, using the 2000 and 2010 censuses, and its inter-census estimates. The study’s dependent variables referred to the rates according to male and female sex and age group (0-4 years, 5-9 years, 10-19 years, 20-39 years, 40-59 years, 60 years or more) by gender. The independent variable was the year 2008 to 2018
For each year of the studied period, the hospitalization rates for burns, grossly and specifically, were calculated according to the dependent variables of interest: age group and sex, calculated for every 100,000 inhabitants using the total number of hospitalizations, divided by the general population of the period (general, by sex and age group by sex). Standardized morbidity coefficients and the simple linear regression method were used with the Statistical Package for the Social Sciences (SPSS) version 18.0 to analyze the temporal trends in burn morbidity. In this method, the standardized hospitalization rates were considered as dependent variables, and the years of the study calendar as independent variables, thus obtaining the model estimated according to the formula Y = b0 + bI X, where y = standardized coefficient, b0 = average coefficient for the period, Bi = average annual increase and X = year. The results were presented in rates, r = correlation coefficient, b = slope, and p-value. P <0.05 was considered statistically significant.
RESULTS
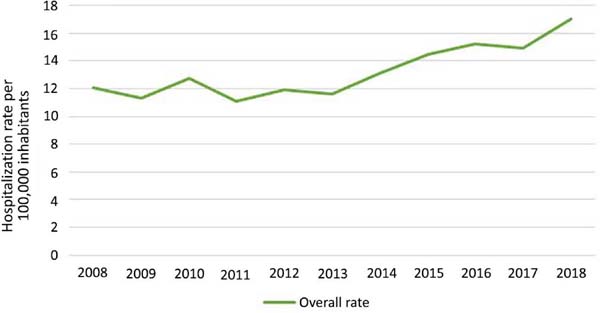
In the period analyzed (2008-2018), there were 9,158 hospitalizations for burns registered in public hospitals in Santa Catarina. The trend in the general rate of hospitalization for burns is shown in Figure 1. The rate of hospitalization in 2008, at the beginning of the period, was 12.06 hospitalizations per 100,000 inhabitants, ending the period (2018), with the rate increasing to 17.07 hospitalizations per 100,000 inhabitants.
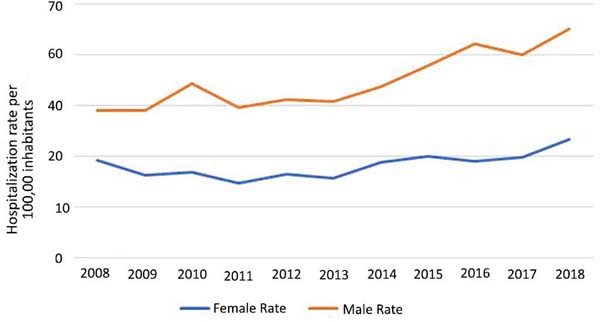
When stratifying the hospitalization rate by sex, it was noticed that in males, it is higher (Figure 2). The male hospitalization rate started at 14.52, ending the historical series with 22.51/100,000 inhabitants. In females, the initial rate was 9.52 hospitalizations per 100,000 inhabitants and, at the end of the period, increased to 11.72 per 100,000 inhabitants. There were more variations in the trend in males in the period, with a significant increase from 2013.

Figures 3 and 4 show the trend of the time series according to the age group by sex. In Figure 3, which shows the time trend for hospitalization due to burns in females, it can be seen that the most affected group is 0-4 years old, with rates of 28, 86 at the beginning of the period, and 69.40 per 100,000 at the end of the historical series. Besides, there is an increase in the rate in the age group of 5 to 9 years in 2016 from 11.44 to 26.01 per 100,000 inhabitants.
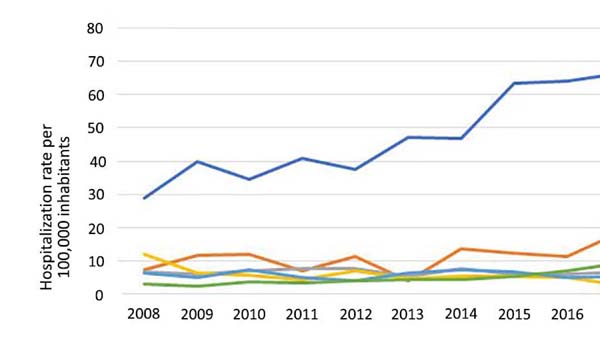

The rate of hospitalization for burns in males by age group is shown in Figure 4. During the entire period, there is an increase in the age group from 0 to 4 years, from 44.75 (100,000 inhabitants) to 115.37 (100,000 inhabitants).
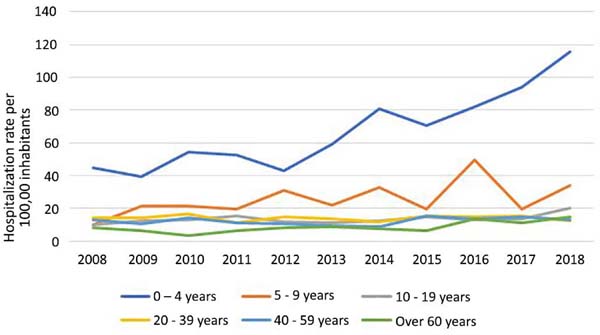

Table 1 shows the annual percentage change, coefficient of determination (R2), the average annual change (β), the p-value, and the trend stratified by sex and age group.
| Annual Percentage Variation (%) | R2 | Average Annual Variation (β) | p-value | Trend | |
|---|---|---|---|---|---|
| General hospitalization rate Hospitalization rate by sex | 29.34 | 0.735 | 0.499 | 0.001 | Increase |
| Female | 17.91 | 0.44 | 0.248 | 0.026 | Increase |
| Male | 35.49 | 0.794 | 0.756 | 0 | Increase |
| Hospitalization rate by age group | |||||
| Female | |||||
| 0-4 years | 58.41 | 0.902 | 4.112 | 0 | Increase |
| 5-9 years | 71.22 | 0.447 | 1.201 | 0.024 | Increase |
| 10-19 years | 28.12 | 0.089 | 0.103 | 0.373 | Stable |
| 20-39 years | -97.71 | 0.346 | -0.416 | 0.057 | Stable |
| 40-59 years | -39.15 | 0.042 | -0.072 | 0.546 | Stable |
| More than 60 years | 55.53 | 0.785 | 0.542 | 0 | Increase |
| Male | |||||
| 0-4 years | 61.21 | 0.858 | 6.788 | 0 | Increase |
| 5-9 years | 70.38 | 0.311 | 1.795 | 0.074 | Stable |
| 10-19 years | 50.54 | 0.372 | 0.498 | 0.046 | Increase |
| 20-39 years | -15.64 | 0.007 | -0.042 | 0.802 | Stable |
| 40-59 years | 1.01 | 0.093 | 0.202 | 0.362 | Stable |
| More than 60 years | 42.5 | 0.526 | 0.737 | 0.012 | Increase |

There was a 29.34% increase in the overall burn rate over the study period (2008 to 2018). Concerning sex, there is a significant upward trend for both men and women, with an annual percentage change of 35.49% and 17.91%, respectively. When analyzed by age group, there was a tendency to increase in ages between 0-4, 5-9, and over 60 years old in females. In males, there was a tendency to increase in ages between 0-4, 10-19, and over 60 years
DISCUSSION
In the world, burns represent a significant cause of morbidity and mortality and can lead to considerable economic and social impact7. These injuries are in fourth place as the most prevalent type of trauma in the world, after traffic accidents, falls, and interpersonal violence and they represent one of the biggest problems in global public health due to the impact represented by the severity of their injuries18.
The data obtained in the present study demonstrated a time trend of increase in the number of hospitalizations due to burns in the state of Santa Catarina in the studied period (2008-2018). However, a similar study in the same state between 1998 and 2012 showed a decrease in the number of cases13. The morbidity rate in 1998 was close to 16 hospitalizations per 100,000 inhabitants, decreasing in 2012 to less than 14 hospitalizations/100,000 and remaining constant14. Another study carried out in the southern region of Brazil, between 2008 and 2016, found that the hospitalization rate for burns at the beginning of the period was 13.11 per 100,000 inhabitants, ending in 2016 with 14.60/100,000 inhabitants and remaining constant14. When we analyzed these results, it was noticed that both are in a temporal agreement since the hospitalization rates increased sharply from the year 2015.
In Brazil in the period from 2000 to 2014 the general hospitalization rate was 14.56 per 100,000 inhabitants and, when comparing hospitalization rates in Brazil by states, this longitudinal study found that the state of Goiás had the highest overall hospitalization rate due to burns, reaching 28.8 per 100,000 inhabitants, a number significantly higher than that observed in the southern states of Brazil19. This difference found was not explained by the author of the work. It is relevant to note that this type of epidemiological, ecological study does not often present enough information to justify individual issues.
As for the sex of victims of burn hospitalization in Brazil, the present study observed an increase in both sexes, and the highest rate of victims hospitalized for burns was male patients. These data agree with results obtained in other international studies, where countries such as Finland and Germany also have a predominance of male hospitalizations20,21. Even compared with other studies in the national territory, it was observed that there is a predominance of males8,11.
The triggering factor for the predominance of the male profile in hospitalization rates, although not explicitly demonstrated, may be associated with the way men relate to the work they do because epidemiologically, men are occupants of professions with greater danger and that require more significant physical effort and would subject them to more risk of accidents. The high hiring of male professionals in chemical and oil industries in activities that require the handling of mechanical and welding equipment, and professions that require contact with flammable fuels, would be responsible for the increase in these rates. As for the female sex, burn accidents would be most associated with domestic accidents, domestic violence, and self-harm, as in suicide attempts22.
The group that includes individuals from 0 to 4 years old stood out as the most affected age group in both sexes. This finding agrees with other countries such as Portugal, which presented a rate of 54.6 per 100,000 inhabitants in the same age group, where scalding in the home environment was characterized as a significant cause of burn23. Because they are still without the cognitive integrity of discerning risk situations, younger children are more exposed to accidents, intrinsically related to their parents’ knowledge about preventing burns, and first aid24.
Children, aged between 5 and 9 years old, tended to increase hospitalizations in women and stability in men. The possible accomplishment of housework can explain this predominance as an assistant in the kitchen, the most commonplace of accidents in schoolchildren and preschoolers3.
In the 10-19 age group, there was an increase in the trend in males and stability in females. There was a scarcity of studies in the literature covering adolescents. Serra et al., in 201225, carried out a study with hospitalizations for burns between 12 and 18 years old, in the period from 2007 to 2011, and the authors found that 33.33% of hospitalizations were caused by alcohol and the most prevalent age was 17 years. This fact can be justified by the ambivalence of interacting with the external world in a freer way, without apparently having to assume the responsibilities of adult life25. Besides, the male gender in this age group starts to consume alcohol and drugs, leading to higher suicide attempts and burn accidents. Concerning the age group of adults, in this study between 20-59 years, there was a tendency towards stability.
The elderly, contained in the age group above 60 years, showed an increase in both sexes during the period, suggesting a relationship with the increase in longevity in recent years. This increase in hospitalizations can be explained by changes inherent to age, such as decreased sensory and cognitive functions, predisposing a deficit in the preventing accidents and increasing the possibility of thermal trauma. In the literature that male domestic accidents are the most prevalent, this age group is related to worse clinical evolution, weak recovery, and a higher number of days of hospitalization and hospital cost4,26,27.
A recent study performed in the country showed that health professionals have unsatisfactory knowledge with the first assistance to the burned individual28, which can cause a higher number of complications and a more significant number of hospitalizations due to negligence in the first care. Besides, the state of Santa Catarina has a high level of notification concerning the rest of Brazil and a higher number of notifications in recent years.
All scientific studies are subject to bias and limitations. As limitations in this study, the fact that the data source was exclusively the DATASUS database, thus excluding data from hospitalizations of private patients or financed by health insurance, for this reason, there may be underreporting of hospitalizations due to external causes29. In addition to the limitations, the possibility that hospitals that are not accredited as being of high complexity can use codes other than burns when issuing hospitalization to raise more resources for care, decreasing the numbers in this study data. Despite this, DATASUS is still considered a good source by WHO. It should be noted that more regionalized studies are needed to observe better the factors associated with burns.
CONCLUSION
During the period studied, there were 9,158 hospitalizations due to burns, corresponding to the rate of 14.52 hospitalizations per 100,000 inhabitants at the beginning of the period and 22.51 hospitalizations per 100,000 inhabitants at the end of the historical series.
When analyzing the general hospitalization rate, there is an increase of 29.34% in the period. Both rates of hospitalization due to burns tended to increase, with males being the highest throughout the study.
When observing the different age groups, the group that includes individuals from 0 to 4 years old stands out as the most affected in the state of Santa Catarina.
REFERENCES
1. Piccolo NS, Serra MCVF, Leonardi DF, Lima Júnior EM, Novaes FN, Correa MD, et al. Projeto e Diretrizes. Queimaduras: diagnóstico e tratamento inicial. São Paulo (SP): Associação Médica Brasileira (AMB)/Conselho Federal de Medicina (CFM); 2008.
2. Queiroz PR, Lima KC, Alcântara IC. Prevalência e fatores associados a queimaduras de terceiro grau no município de Natal, RN. Rev Bras Queimaduras. 2013;12(3):169-76.
3. Meschial WC, Sales CF, Oliveira MLF. Fatores de risco e medidas de prevenção das queimaduras infantis: revisão integrativa da literatura. Rev Bras Queimaduras. 2014;15(4):267-73.
4. Silva RV, Rita CMS, Novaes MRCG. Fatores de risco e métodos de prevenção de queimaduras em idosos. Rev Bras Cir Plást. 2015;30(3):461-7.
5. Nestor A, Turra K. Perfil epidemiológico dos pacientes internados vítimas de queimaduras por agentes inflamáveis. Rev Bras Queimaduras. 2014;13(1):44-50.
6. Strassle PD, Williams FN, Weber DJ, Sickbert-Bennett EE, Lachiewicz AM, Napravnik S, et al. Risk factors for healthcare-associated infections in adult burn patients. Infect Control Hosp Epidemiol. 2017 Dez;38(12):1441-8.
7. Adorno Filho ET, Almeida KG, Reis GC, Costa GR, Kracik AS, Tuluche LHF, et al. Análise dos custos de pacientes internados na Santa Casa Misericórdia de Campo Grande, tratados com e sem auxílio de oxigenoterapia hiperbárica. Rer Bras Cir Plást. 2014;29(4):562-6.
8. Pereira Júnior S, Ely JB, Sakae TM, Nolla A, Mendes FD. Estudo de pacientes vítimas de queimaduras internados no Hospital Nossa Senhora Da Conceição em Tubarão - SC. Arq Catarin Med. 2007;36(2):22-7.
9. Rowan MP, Cancio LC, Elster EA, Burmeister DM, Rose LF, Natesan S, et al. Burn wound healing and treatment: review and advancements. Crit Care. 2015 Jun;19(1):243.
10. Smolle C, Cambiaso-Daniel J, Forbes AA, Wurzer P, Hundeshagen G, Branski LK. Recent trends in burn epidemiology worldwide: a systematic review. Burns. 2017;43(2):249-57.
11. Cruz BF, Cordovil PBL, Batista KNM. Perfil epidemiológico de pacientes que sofreram queimaduras no Brasil: revisão de literatura. Rev Bras Queimaduras. 2012;11(4):246-50.
12. Favassa MT, Vietta GG, Nazário NO. Tendência temporal de internação por queimadura no Sul do Brasil. Rev Bras Queimaduras. 2017 Set/Dez;16(3):163-8.
13. Gervasi LC, Tibola J, Scheneider IJC. Tendência de morbidade hospitalar por queimaduras em Santa Catarina. Rev Bras Queimaduras. 2014;13(1):31-7.
14. Gragnani A, Ferreira LM. Pesquisa em queimadura. Rev Bras Queimaduras. 2009;8(3):91-6.
15. Gimenes GA, Alferes FCBA, Dorsa PP, Barros ACP, Gonella HA. Estudo epidemiológico de pacientes internados no Centro de Tratamento de Queimados do Conjunto Hospitalar de Sorocaba. Rev Bras Queimaduras. 2009;8(1):14-7.
16. Ministério da Saúde (BR). Departamento de Informática do SUS (DATASUS). SIHSUS [Internet]. Brasília (DF): DATASUS; 2008; [acesso em 2018 Set 17]. Disponível em: http://datasus.saude.gov.br/sistemas-eaplicativos/hospitalares/sihsus
17. Ministério da Saúde (BR). Departamento de Informática do SUS (DATASUS). Tecnologia da Informação a serviço do SUS. TABNET (Informações em Saúde) - SIHSUS [Internet]. Brasília (DF): DATASUS; 2016; [acesso em 2018 Set 17]. Disponível em: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sih/cnv/niuf.def
18. Hernández CMC, Núnez VP, Suárez FAP, Banqueris RF, Gil SRL, Machado AAB. Mortalidade por queimaduras em pacientes hospitalizados em Manzanillo-Cuba em 2015-2017. Rev Bras Queimaduras. 2018;17(2):76-80.
19. Santos JV, Souza J, Amarante J, Freitas A. Burden of burns in Brazil from 2000 to 2014: a Nationwide Hospital-Based Study. World J Surg. 2017 Ago;41(8):2006-12.
20. Tanttula K, Haikonen K, Vuola J. Hospitalized burns in Finland: 36305 casos from 1980- 2010. Burns. 2018 Mai;44(3):651-7.
21. Theodorou P, Xu W, Weinand C, Perbix W, Maegele M, Lefering R, et al. Incidence and treatment of burns: a twenty-year experience from a single center in Germany. Burns. 2013;39 49-54.
22. Lacerda LA, Carneiro AC, Oliveira AF Gragnani A, Ferreira LM. Estudo epidemiológico da Unidade de Tratamento de Queimaduras da Universidade Federal de São Paulo. Rev Bras Queimaduras. 2010;9(3):82-8.
23. Santos JV, Viana V, Oliveira A, Ramalho A, Sousa-Teixeira J, Duke J, et al. Hospitalisations with burns in children younger than five years in Portugal, 2011-2015. Burns. 2019 Ago;45(5):1223-30.
24. Cox SG, Burahee A, Albertyn R, Makahabane J, Rode H. Parent knowledge on pediatric burn prevention related to the home environment. Burns. 2016 Dez;42(8):1854-60.
25. Serra MC, Queiroz ME, Silva VP, Bufada M, Araújo N, Macieira L, et al. Perfil das queimaduras em adolescentes. Rev Bras Queimaduras. 2012;11(1):20-2.
26. Abu-Sittah GS, Chahine FM, Janom H. Manegement of burns in the elderly. Ann Burns Fire Disasters. 2016 Dez;29(4):249-5.
27. Giuli AE, Itakussu EY, Valenciano PJ, Fujisawa DS, Trelha CS. Caracterização de idosos vítimas de queimaduras internados em um centro de tratamento de queimados. Rev Bras Queimaduras. 2015;14(4):253-6.
28. Pan R, Silva MTR, Fidelis TLN, Vilela LS, Silveira-Monteiro CA, Nascimento LC. Conhecimento de profissionais de saúde acerca do atendimento inicial intra-hospitalar ao paciente vítima de queimaduras. Rev Gaúcha Enferm. 2018 Set;39:2017-79.
29. Tomimatsu MFAI, Andrade SM, Soares DA, Mathias TAF, Sapata MPM, Soares DFPP, et al. Qualidade da informação sobre causas externas no Sistema de Informações Hospitalares. Rev Saúde Pública. 2009;43(3):413-20.
1. University Hospital, Florianópolis, SC,
Brazil.
2. Universidade do Sul de Santa Catarina, Palhoça,
SC, Brazil.
3. Federal University of Santa Catarina,
Florianópolis, SC, Brazil.
FOD Conception and design study, Conceptualization, Final manuscript approval, Methodology, Project Administration, Supervision, Visualization, Writing - Original Draft Preparation, Writing - Review & Editing
SGH Analysis and/or data interpretation, Conception and design study, Data Curation, Formal Analysis, Investigation, Methodology, Project Administration, Writing - Original Draft Preparation
MOM Analysis and/or data interpretation, Conception and design study, Final manuscript approval, Formal Analysis, Methodology, Project Administration, Supervision, Writing - Review & Editing
JBE Analysis and/or data interpretation, Conceptualization, Data Curation, Investigation, Methodology, Supervision
Corresponding author: Felipe Oliveira Duarte, Avenida Professor Othon Gama D’Eça 900, Centro, Florianópolis, Santa Catarina, Brazil. Zip Code: 88015-240, E-mail: duarte.cirurgiaplastica@gmail.com
Article received: February 29, 2020.
Article accepted: July 15, 2020.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket