



Special Article - Year 2017 - Volume 32 -
History of plastic surgery: Sir Harold Gillies, a pioneer of reconstructive plastic surgery
História da Cirurgia Plástica: Sir Harold Gillies, pioneiro da cirurgia plástica reconstrutiva
ABSTRACT
Historically, wars have been among the greatest catalysts for advances in medicine in general, and surgery in particular. Without doubt, the greatest practitioner of plastic surgery in the early decades of the twentieth century was Sir Harold Delf Gillies, a New Zealander living in England, who advocated the treatment of patients with facial injuries in the context of the First World War. This article examines Gillies' personal life and the legacy he left for modern plastic and reconstructive surgery; many of his teachings are timeless and serve as an inspiration for the surgeons of today.
Keywords: History of medicine; Surgical reconstructive procedures; Surgery, plastic; Warfare; Trauma.
RESUMO
Historicamente, as guerras foram um dos maiores catalisadores para o avanço da Medicina, e especialmente da cirurgia. Sem dúvida, a maior autoridade da Cirurgia Plástica nas primeiras décadas do século XX foi o neozelandês radicado na Inglaterra Sir Harold Delf Gillies, que se destacou pelo tratamento de pacientes com lesões faciais no contexto da I Guerra Mundial. Nosso artigo faz uma análise da vida pessoal e do legado que Gillies deixou para a cirurgia plástica e reconstrutiva moderna; muitos de seus ensinamentos são atemporais e servem de reflexão para cirurgiões da atualidade.
Palavras-chave: História da medicina; Procedimentos cirúrgicos reconstrutivos; Cirurgia plástica; Guerra; Trauma.
The interest of Sir Harold Gillies, Commander of the British Empire, Fellow of the Royal College of Surgeons (Figure 1), in the treatment of nasal deformities and other facial abnormalities led him to become one of the pioneers of facial plastic surgery at the beginning of the 20th century. Despite no formal training in Plastic Surgery, he distinguished himself by treating numerous patients with facial injuries during the First World War.

Figure 1. Sir Harold Gillies (right, sitting in the operating room, Queen's Hospital, Sidcup (courtesy of Dr. Andrew Bamji, Gillies Archivist, BAPRAS).
Gillies developed his interest in facial lesions using a dental approach. He later visited the French plastic surgeon Hippolyte Morestin, who was performing the most advanced reconstructive surgeries of the time at the Val de Grâce Hospital, Paris1. From these experiences, he became aware of the many jaw and cranioencephalic injuries that trench warfare had produced2,3.
To address the need to treat these injuries, Gillies used his persuasive skills to promote development of a multidisciplinary approach to facial injury treatment at Cambridge Military Hospital in 1916, and at Queen's Hospital the following year (Figures 2 and 3). This model was so successful that subunits were established to provide care for injured Commonwealth personnel in Canada, New Zealand, and Australia.

Figure 2. Plastic surgery operating room, Queen's Hospital, Sidcup (courtesy of Dr. Andrew Bamji, Gillies Archivist, BAPRAS).

Figure 3. Ward at Queen's Hospital (courtesy of Dr. Andrew Bamji, Gillies Archivist, BAPRAS).
Between 1917 and 1923, he and his team of surgeons and dentists operated on more than 5,000 patients. Some of the traumatic lesions had similarities to developmental clefts and other congenital deformities, and thus provided experience for corrective treatment. The files are stored in the Gillies Archives, Queen Mary's Hospital, Sidcup, located in the original hospital complex that included recovery and rehabilitation facilities4.
Severe traumatic facial deformities were corrected with surgical procedures that are now part of history (such as free bone grafts for mandibular reconstruction, rotational flaps, and pedicled tubular grafts). As noted by several authors, there is no doubt that the wounded of the Western Front of World War I were the subjects of experiments that allowed the development of modern Plastic Surgery5.
After World War I, Gillies was appointed to the clinical staff of St. Bartholomew's Hospital as one of the few British plastic surgeons of the time, emerging as the leader in his field5. He eventually became a consultant, a top position for a physician in the British health care system, to the Navy, Royal Air Force, Ministry of Health, and six other hospitals.
In contrast with the success of plastic surgeons in North America during the period between the wars, British plastic surgeons failed to promote the specialty in England. Despite his extensive surgical experience and reputation, Gillies was able to achieve very little during this period.
He had difficulty finding sufficient work to support his practice, let alone train new specialists. He also had difficulty maintaining his popularity, as his attempt to increase the number of surgical cases by performing purely cosmetic procedures led him to be falsely portrayed as a charlatan6,7.
With the beginning of the Second World War, Gillies converted the private wing of the Park Prewett hospital, Basingstoke, into a plastic surgery hospital with 120 beds. At that time, there were four plastic surgeons in the United Kingdom8, with around 60 in the United States9.
A lifelong smoker, Gillies remained active as a teacher until his death, and died suddenly in 1960, at 78 years of age, from coronary artery disease5.
OBJECTIVE
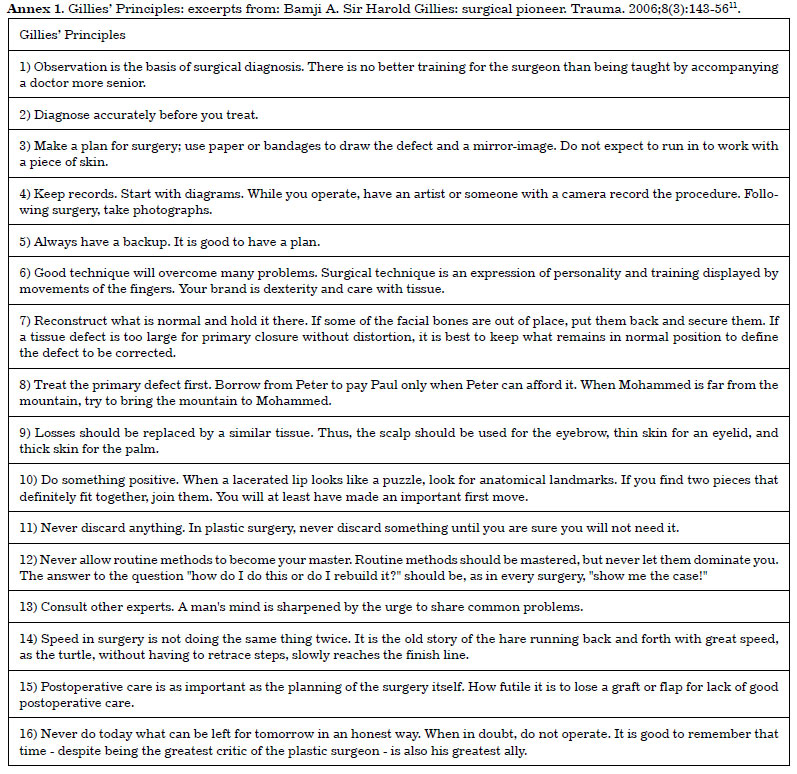
The aim is to discuss the contribution of Gillies to the emergence of plastic surgery as a specialty from a historic point of view. Gillies was described as a brilliant teacher. Many of his teachings were summarized in the famous "Principles of Gillies" (Annex 1). Those who were under his tutelage and had been trained to use their hands to feel or point out a defect in a patient were criticized and told: "Use your eyes first to assess the problem and keep those dirty fingers away from the patient!"10 As a master craftsman in the operating room, he emphasized the vital importance of meticulous hemostasis in flap reconstruction; one of his maxims was "a teaspoon of blood today is worth a bucket tomorrow."
METHODS
This review was based on online database searches in PubMed, SciELO, and LILACS, using ununified terms, for historical information relevant to the life of Harold Gillies and his contribution to the rise of plastic surgery as a specialty.
RESULTS
Legacy and contributions to modern plastic surgery
Born in Dunedin, New Zealand, in 1882, his father was a member of the New Zealand Parliament and his mother was from a prominent family (Figure 4). He was educated at Wanganui College, New Zealand, where he was captain of the cricket team. Later, he studied at Gonville and Caius College, and attended medical school at the University of Cambridge, England5,10,11.

Figure 4. Gillies at approximately 8 years of age (courtesy of Dr. Andrew Bamji, Gillies Archivist, BAPRAS).
He overcame the difficulties caused by a stiff elbow after a childhood accident and managed to row for Cambridge in the famous boat race against Oxford in 1904, as well as play for England against Scotland, winning at the Royal St George Grand Challenge Cup, in Sandwich, in 1913.
He graduated in Otorhinolaryngology at St Bartholomew's Hospital in 1906 and became a Fellow of the Royal College of Surgeons in 191011.
After the outbreak of the First World War, in 1914, he joined the Royal Army Medical Corps (entering as a captain and ended his career as a major). In 1915, he volunteered for the Red Cross in the French village of Wimereux, where he met a Franco-American dentist named Charles Valadier, who worked in a British field hospital. Gillies was surprised by Valadier's approach to treating jaw injuries. Inspired by this dental approach to facial lesions, Gillies decided to visit the French plastic surgeon Hippolyte Morestin, who was performing the most advanced reconstructive surgeries of the time at Val de Grâce Hospital, Paris1.
At the end of the war, American observers came to Sidcup; the most significant of these was Vilray Blair, who, together with Varaztad Kazanjian, the "miracle worker of the Western Front," worked as a dentist in French hospitals.12 Blair then returned to the United States to virtually found plastic and maxillofacial surgery in that country. Gillies, in his book « Principles and Art of Plastic Surgery, coauthored with Millard, contrasted the enthusiasm with which the American medical establishment embraced plastic surgery with the difficulties and obstacles it faced in the UK (without disguising some envy)6.
In 1917, he described a series of cases in which the temporal muscle was used as a transposition flap for deformities caused by zygomatic loss. His inspiration for this technique came from German surgeons who used temporal fascia flaps to treat facial paralysis. Many surgeons started to use this flap to support and reconstruct the orbit13.
Two anesthetists who worked with Gillies, Stanley Rowbotham and Ivan McGill, became leaders in their specialty, and were the originators of the nasotracheal intubation technique, which later became widespread12.
The working conditions in the initial period of development of his work were difficult, prior to the advent of antibiotics (sulfonamides became available in the late 1930s, and penicillin was introduced in 1943). Without knowledge of the need for adequate hygiene, several patients had multiple dental infections. Given this limited pharmacological environment, one of the precepts preached by Gillies and adopted by Cushing was early surgical debridement of craniofacial lesions, which helped reduce local infection and brain abscesses9.
The artist Henry Tonks, who began his career as a surgeon and was also a member of the Royal College of Surgeons, was recruited to record the cases by means of beautiful paintings and sketches (now on display in the Hunterian Museum at the Royal College of Surgeons, London), and to assist in the planning of repair work.
One of Gillies' pupils was his distant cousin, Sir Archibald McIndoe, who was one of his collaborators during the Second World War, and one of the proponents of British plastic surgery in this period. McIndoe was later recognized as Britain's leading burn authority for his treatment of aviators at the Royal Air Force Hospital in East Grinstead5,14, and was knighted in 1930.
Gillies was considered an excellent golfer (Figure 5), with a handicap of +2, having played three times for England against Scotland (including at St. Andrew's, the cradle of golf), which led him to be the object of a cartoon in The Daily Mail for his ability to tee off cleanly from a bottle of beer. His passion for the sport was such that he sometimes neglected his duties, even keeping members of the nobility waiting10. Gillies was also a great fisherman and promoted the benefits of outdoor living (Figure 6).

Figure 5. Harold Gillies card contained in packet of Wills cigarettes in series celebrating great British golfers (courtesy of Dr. Andrew Bamji, Gillies Archivist, BAPRAS).

Figure 6. Gillies on a fishing trip, practicing one of his favorite hobbies (courtesy of Dr. Andrew Bamji, Gillies Archivist, BAPRAS).
He reported and extensively demonstrated rhinoplasty techniques, which he applied in his private aesthetic practice15,16. In 1932, he described the use of direct pedicle flaps, rather than tubular flaps, which entailed only two surgical interventions17. He treated and described the management of congenital and traumatically acquired palatal clefts18 (Figure 7). In 1947, with the founding of the British Association of Plastic Surgeons, Gillies was chosen as its first president. He was awarded honorary degrees at multiple universities and plastic surgery associations all over the world, having travelled extensively throughout South America.

Figure 7. Seaman Vicarage. First tubular pedicle flap performed by Gillies (From Gillies: "Plastic Surgery of the Face", London, 1920).
As for his versatility, one can highlight significant activities, such as his collaboration with the American Harvey Cushing - a great pioneer of neurosurgery - in complex cases of combined facial and cranioencephalic lesions6,9,12.
In addition to his role in reconstructive facial surgery, Gillies is also considered a pioneer in reconstructive genital surgery, including genital reassignment. Jacques Joseph had already performed, in the interwar period, a sex change from male to female, but the opposite procedure had not yet been performed.
Gillies was persuaded to perform the procedure on Laura Dillon, a medical student at that time. She had already been submitted to a double mastectomy and the use of exogenous androgens, and changed her name to Michael. The initial surgery was in 1946, and achieved some degree of success, despite the imperfect form of the neo-penis11.
Of all the facial plastic surgeries, he considered rhinoplasty to be the most difficult, "except perhaps otoplasty, in which I do not have much experience," the reason being that these would be, in his opinion, "final organs" (body extremities). As in the current literature, he identified the three elements that needed to be reconstructed: 1) the outer layer, the skin; 2) cartilage and bone support; and 3) the inner lining mucous membrane. These principles are still applicable16,19. Nevertheless, when described as a pioneer in the field of plastic surgery, his humility forced him to argue that it was an ancient art14.
One of his best-known phrases is that "restorative surgery is an attempt to return the patient to normality; aesthetic surgery, an attempt to overcome normality"3.
DISCUSSION
Although focusing primarily on facial plastic surgery and repair, the interests of Gillies expanded to the use of flaps, microvascular surgery, and correction of limb amputations. Like other surgeons, Gillies acknowledged that science sometimes needs wars to evolve14. In addition, he was also interested in surgical treatment using pedicled grafts and flaps in patients who had undergone external radiotherapy, a modality that at the time was used for diverse pathologies, including cosmetic removal of axillary hair, exophthalmic goiter, lupus, psoriasis, and abdominal and gynecological tumors6,20.
He was a great proponent of the multidisciplinary approach in the pre- and postoperative care of patients. One of Gillies' best-known aphorisms is "never do today what can be honestly done tomorrow," that is, he reiterated the need for adequate preoperative preparation to optimize outcomes1. What may have been his most important advice was "keep records," including medical history, detailed and well-described physical examinations, and pre- and post-operative photographs, which were all relevant, especially for use in medical education, knowledge dissemination, and medicolegal matters11,19,21.
His maxim of "never throw away anything until you are sure you will not need it" is a doctrine that perpetuates itself in all areas of plastic surgery and repair. Gillies was constantly developing new techniques to deal with common problems. His technique for the treatment of eyelid ectropion integrated the Esser epithelial inlay, which was used to deepen the labiogingival groove, with Thiersch grafting. He used this technique in other cases, notably for burn-induced adhesions between the pinna and scalp10.
Several surgical instruments were also developed or improved by Gillies, among them forceps, the zygomatic elevator, skin hooks, needle holders and scissors, which remain in use today. It is speculated that his eponymous, more ergonomic needle holder is the result of the elbow fracture sustained in childhood, which limited his ability to pronate and supinate; however, parallels are drawn between the ergonomics of the needle holder and a golf club handle22.
From all the above and the countless reports on the life and works of Gillies, his contribution to plastic surgery is undeniable. He was a versatile and innovative surgeon and a pioneer in restorative surgery, providing a theoretical basis for the development of cosmetic surgery as we know it today.
His work in various fields of restorative surgery - pedicle flaps, genital alterations, craniofacial correction, microvascular repair - designates him as the complete surgeon, with extensive knowledge in overlapping areas that serve as the basis for the current training curriculum of a plastic surgeon.
CONCLUSION
In reviewing the life of Sir Harold Gillies, the enormous contribution he made to modern reconstructive plastic surgery becomes evident. His legacy comprises a diversity of techniques and concepts developed on the French battlefields in 1915 that proved their relevance to the principles in use today, a century later. The foundation of knowledge left by Gillies made it possible to achieve advances such as heterologous dermal matrices, magnetic resonance, and microsurgical reconstructions.
Finally, as in the famous quote by Sir Isaac Newton attributed to Bernard de Chartres - "If I have seen further, it is by standing on the shoulders of giants" - it is essential to bear in mind that future progress in surgery must build on the techniques developed by pioneers who preceded us.
ACKNOWLEDGEMENTS
We would like to thank Dr. Andrew Bamji, Gillies Archivist, BAPRAS, for kindly providing the images.
COLLABORATIONS
PSP Analysis and/or interpretation of data; final approval of the manuscript; conception and design of the study; writing the manuscript or critical review of its contents.
PG Final approval of the manuscript; conception and design of the study; writing the manuscript or critical review of its contents.
GFD Final approval of the manuscript; conception and design of the study; writing the manuscript or critical review of its contents.
GBC Conception and design of the study; writing the manuscript or critical review of its contents.
RFMR Analysis and/or interpretation of data; final approval of the manuscript; conception and design of the study.
COU Analysis and/or interpretation of data; final approval of the manuscript; conception and design of the study; writing the manuscript or critical review of its contents.
MPO Analysis and/or interpretation of data; final approval of the manuscript; conception and design of the study; writing the manuscript or critical review of its contents.
REFERENCES
1. Triana RJ Jr. Sir Harold Gillies. Arch Facial Plast Surg. 1999;1(2):142-3. DOI: http://dx.doi.org/10.1001/archfaci.1.2.142
2. Haiken E. Venus Envy. A History of Cosmetic Surgery. Baltimore: Johns Hopkins University Press; 1997.
3. Taschen A. La Sorprendente História de La Cirugía Estética. In: Taschen A. Cirugía Estética. Madrid: Taschen; 2005.
4. Gerike AE. World War I and my mother's jaw. JAMA Facial Plast Surg. 2013;15(1):9-10. DOI: http://dx.doi.org/10.1001/2013.jamafacial.6
5. Ellis H. Two pioneers of plastic surgery: Sir Harold Delf Gillies and Sir Archibald McIndoe. Br J Hosp Med (Lond). 2010;71(12):698. DOI: http://dx.doi.org/10.12968/hmed.2010.71.12.698
6. Simpson DA, David DJ. Herbert Moran Memorial Lecture. World War I: the genesis of craniomaxillofacial surgery? ANZ J Surg. 2004;74(1-2):71-7. DOI: http://dx.doi.org/10.1046/j.1445-1433.2003.02895.x
7. Chambers JA, Ray PD. Achieving growth and excellence in medicine: the case history of armed conflict and modern reconstructive surgery. Ann Plast Surg. 2009;63(5):473-8. DOI: http://dx.doi.org/10.1097/SAP.0b013e3181bc327a
8. Fraser JF, Hultman CS. America's fertile frontier: how America surpassed Britain in the development and growth of plastic surgery during the interwar years of 1920-1940. Ann Plast Surg. 2010;64(5):610-3. PMID: 20395812
9. Sykes PJ, Bamji AN. Plastic surgery during the interwar years and the development of the speciality in Britain. Ann Plast Surg. 2010;65(4):374-7. DOI: http://dx.doi.org/10.1097/SAP.0b013e3181f4a9dc
10. Pound R. Gillies: Surgeon Extraordinary. London: Michael Joseph; 1964.
11. Bamji A. Sir Harold Gillies: surgical pioneer. Trauma. 2006;8(3):143-56. DOI: http://dx.doi.org/10.1177/1460408606072329
12. Chambers JA, Davis MR, Rasmussen TE. A band of surgeons, a long healing line: development of craniofacial surgery in response to armed conflict. J Craniofac Surg. 2010;21(4):991-7. DOI: http://dx.doi.org/10.1097/SCS.0b013e3181e1e81e
13. Speculand B. The origin of the temporalis muscle flap. Br J Oral Maxillofac Surg. 1992;30(6):390-2. DOI: http://dx.doi.org/10.1016/0266-4356(92)90207-Y
14. Pitanguy I. Aprendiz do Tempo - Histórias Vividas. Rio de Janeiro: Nova Fronteira; 2007.
15. Gillies HD. Demonstration on Rhinoplasty. Proc Roy Soc Med. 1918;11:87-90. PMID: 19980168
16. Freshwater MF. A critical comparison of Davis' Principles of Plastic Surgery with Gillies' Plastic Surgery of the face. J Plast Reconstr Aesthet Surg. 2011;64(1):17-26. PMID: 20356811 DOI: http://dx.doi.org/10.1016/j.bjps.2010.03.009
17. Gillies HD. The Design Of Direct Pedicle Flaps. Br Med J. 1932;2(3752):1008. PMID: 20777210 DOI: http://dx.doi.org/10.1136/bmj.2.3752.1008
18. Gillies HD, Fry WK. A New Principle In The Surgical Treatment Of "Congenital Cleft Palate," and Its Mechanical Counterpart. Br Med J. 1921;1(3140):335-8. DOI: http://dx.doi.org/10.1136/bmj.1.3140.335
19. FitzGibbon GM. The Commandments of Gillies. Br J Plast Surg. 1968;21(3):226-39. DOI: http://dx.doi.org/10.1016/S0007-1226(68)80028-1
20. Gillies HD, McIndoe AH. The role of plastic surgery in burns due to roentgen rays and radium. Ann Surg. 1935;101(4):979-96. PMID: 17856547 DOI: http://dx.doi.org/10.1097/00000658-193504000-00001
21. Negus V. Sir Harold Gillies. Arch Otolaryngol. 1966;83(4):372-8. DOI: http://dx.doi.org/10.1001/archotol.1966.00760020374017
22. Karim RB, Hage JJ. History offhand: a golfer's needleholder. Plast Reconstr Surg. 2000;106(6):1346-7. PMID: 11083568 DOI: http://dx.doi.org/10.1097/00006534-200011000-00019
1. Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, RS, Brazil
2. Fundação Faculdade Federal de Ciências Médicas de Porto Alegre, Porto Alegre, RS, Brazil
3. Sociedade Brasileira de Cirurgia Plástica, Porto Alegre, RS, Brazil
Institution: Hospital São Lucas, Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, RS, Brazil.
Corresponding author:
Pedro Salomão Piccinini
Av. Ipiranga, 6690
Porto Alegre, RS, Brazil - Zip Code 90610-000
E-mail: pspiccinini@gmail.com
Article received: May 29, 2015.
Article accepted: September 23, 2017.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket