



Original Article - Year 2017 - Volume 32 -
Circumferential excisions in the trunk and associations in ex-obese patients
Excisões circunferenciais no tronco e associações em pacientes ex-obesos
ABSTRACT
INTRODUCTION: Currently, obesity is a major problem. Changes in dietary habits, regular exercise and bariatric surgery promote better quality of life. Massive weight loss may cause deformities in different body segments, which are normally corrected in multiple surgeries. We present a systematic way of treating these patients, which enable surgical procedures in different regions of the body in a single step.
METHODS: This was a retrospective observational longitudinal study. The surgical technique consisted of gull-wing type incision on the back with resection of fatty tissue associated with abdominoplasty that promoted improvements in the pubis, back, buttocks and lateral thighs via a single incision. The combination of satellite excision as the thigh lifting was associated in certain situations as well as treatment of the upper segment of the trunk in a second time.
RESULTS: The age of patients ranged from 24 to 52 years, average of 34 years old. The mean surgical time in the circumferential excisions was 4 hours and 8 minutes. Surgical complications observed were hematoma, flap necrosis and/or infection. There were three cases of small dehiscence and seroma and one case of pulmonary thromboembolism. In the outpatient follow-up, 85.7% of patients showed to be very satisfied with the final result and no complaints about the size and position of scars. Technical analysis showed a satisfaction level of 92.8% of cases.
CONCLUSION: Satisfactory results elucidated the safety and feasibility of the technique, and scars were acceptable due to significant improvement in body contouring.
Keywords: Obesity; Lipodystrophy; Weight loss.
RESUMO
INTRODUÇÃO: A obesidade é um problema importante na atualidade. Mudanças de hábitos dietéticos, exercícios físicos e a cirurgia bariátrica promovem melhor qualidade de vida. A redução ponderal excessiva ocasiona deformidades em diversos segmentos corporais que são corrigidas em múltiplos tempos operatórios. Apresentamos uma sistematização das maneiras de tratamento destes pacientes, que nos permitem atos operatórios envolvendo as várias regiões do corpo em uma mesma etapa.
MÉTODOS: Estudo observacional longitudinal retrospectivo. A técnica cirúrgica consistiu em incisão do tipo asa de gaivota em dorso, com ressecção do excedente dermogorduroso associada à abdominoplastia, promovendo melhorias no púbis, dorso, nádegas e face lateral das coxas apenas por esta única incisão. A associação de excisões satélites como o lifting de coxas ocorreu em determinadas situações, bem como o tratamento do segmento superior do tronco em um segundo momento.
RESULTADOS: A faixa etária dos pacientes variou de 24 a 52 anos, com média de 34 anos. O tempo médio do ato operatório nas excisões circunferenciais foi de 4 horas e 8 minutos. Não foram observadas complicações cirúrgicas como hematoma, necrose do retalho e/ou infecção. Três casos de pequenas deiscências e seroma, além de um caso de tromboembolismo pulmonar, foram observados. No seguimento ambulatorial, 85,7% dos pacientes mostraram-se muito satisfeitos quanto ao tamanho e posição das cicatrizes. A análise técnica apresentou um grau de satisfação de 92,8%.
CONCLUSÃO: Os resultados satisfatórios elucidam a segurança e praticabilidade da técnica, sendo as cicatrizes aceitáveis devido à melhora do contorno corporal.
Palavras-chave: Obesidade; Lipodistrofia; Perda de peso.
Obesity is a major public health problem in Brazil and in other countries. It is an endemic disease with worldwide incidence. It is estimated that over 50% of the population is overweight, or in the overweight range and obese1.
Changes in dietary habits, regular physical activity and bariatric surgery aim to provide a better quality of life and reduce risk factors to obesity. However, excessive weight loss can lead to a variety of body changes2.
The initial weight reduction of around 40% to 60% causes deformities in several body segments, including the abdominal region, which is characterized as an aesthetic-functional segment of important definition in body contouring3.
The body contouring surgery is defined as a reconstructive and functional surgery. The term "belt lipectomy" is used to define a combination of reconstructive surgery of the abdomen and "lifting" of thighs and buttocks4. Patients with excessive dermis-fat in the anterior abdomen, torso and flanks associated with ptosis of the gluteal region and pubis have significant benefits with circumferential excision5,6.
OBJECTIVE
This study presents the importance of large circumferential excisions, often associated with satellite incisions, which provide simultaneous treatment of different regions, shorten total treatment time and reduce the amount of surgical procedures.
METHODS
This is a retrospective longitudinal study developed in the Plastic Surgery Service of Daher Hospital in the city of Brasília - DF from March 2013 to March 2016.
The research project followed the legal procedures established by the National Health Council Resolution 196/96 with regard to research involving human subjects and in accordance with the principles of the Declaration of Helsinki. All patients who underwent the surgical procedure signed the informed consent (IC).
The sample was intentional and based on ex-obese patients who underwent reconstructive surgery with circumferential excision with or without satellite incisions in the trunk.
The variables were gender, age, weight loss, operative time, postoperative surgical complications, weight of the specimen, body mass index (BMI), hospital stay and satisfaction of the medical team and the patient with the scars and surgery.
The criteria for surgery were:
1) Ex-obese patients who had weight stable for a minimum of 6 months with BMI between 18.5 and 29.9 kg/m2;
2) Patients with excess skin and fat in the abdomen, flanks and back with ptosis of the buttocks and pubis;
3) Patients with excess skin and fat in thighs;
4) Patients classified according to American Society of Anesthesiology - ASA 1 and ASA 2.
Exclusion criteria were:
1) weight stability for a period of less than 6 months and/or BMI> 29.9 kg/m2;
2) ASA greater or equal to 3.
Surgical technique
The surgical team was composed by the senior surgeon and two medical assistants. All patients underwent surgery at surgical center under general anesthesia.
Preoperative marking of abdominoplasty was performed with the patient on standing, sitting and supine position - all markers were associated with "pinch test" (Figure 1).
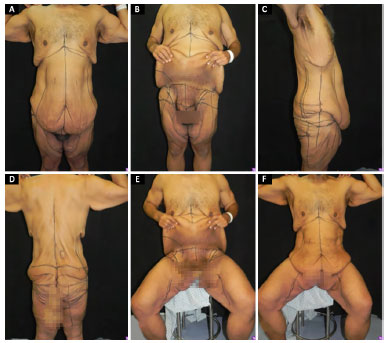
Figure 1. Marking before surgery with patient both stand (A, B, C and D) and sit (E and F).
Initially, we proceeded with anterior abdomen liposuction, back and sides with a solution composed of 0.9% saline and epinephrine at a 1: 500,000. Subsequently, with the patient in prone position a "gull wing" incision was done as defined in the previous marking (Figure 2). The procedure continued with detachment of dermis-fat suprafascial flap until the predetermined region by the "pinch test" with resection exceeding by areas from guiding lines made in the preoperative marking (Figure 3).
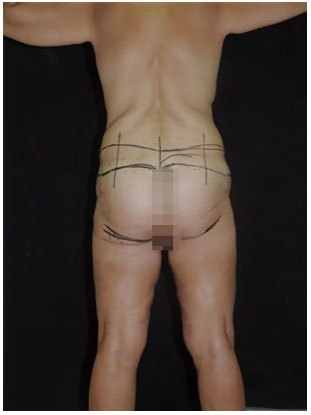
Figure 2. Marking before surgery of gull-wing type incision in dorsal region.
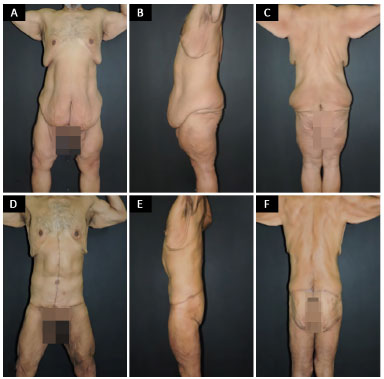
Figure 3. A 44-year-old patient who underwent circumferential excision with anchor abdominoplasty, lifting of things and pubic area. A, B and C: Before surgery; D, E and F: 1-year after surgery.
The synthesis was performed by layers with nylon 3-0 and 4-0. After, patient was placed on supine position for abdominoplasty, which could be both "classic" and "anchor" (dependent on the existing surplus tissue). The plication of the rectus abdominis muscles was performed in all cases. After that the umbilicoplasty was done using a mini-circle skin technique7, caudal traction of abdominal flap, flap was closed up using the Baroudi8 adhesion points and by resection of excessive fatty tissue.
The combination of satellite incisions as thighs lifting was performed in patients with sagging crus, and the marking of the skin was performed with the patient on stand position and confirmed with patient in supine position during the intraoperative, proceeding the incision in the groin and inner thigh with above-fascial detachment and resection of fatty tissue.
Patients undergoing treatment of the upper segment of the trunk with circumferential excisions, the associated surgical procedures were mammoplasty and brachioplasty in secondary time to treatment of lower segment.
Satisfaction level assessment
The evaluation of patients' satisfaction degree with the result was performed in the third, sixth and twelfth months after the surgery using the patient own evaluation, which assessed whether the patient was satisfied or not with the procedure as well as with position of the scar.
Technical evaluation of the results was made by a member of plastic surgeon of the Brazilian Society of Plastic Surgery (and who did not participate in surgical procedures) by using a comparative analysis of the preoperative images 3 months after the surgery.
Statistical analysis
The results were typed in Microsoft Excel 2008 spreadsheets and analyzed in Epi Info program, version 3.5.1. A descriptive analysis of the data was done and presentation of frequencies.
RESULTS
A total of 28 ex-obese patients underwent surgery by Circumferential excisions in the lower segment of the trunk. Seven patients were men and 21 women. Of these patients, 12 were associated with satellites incisions such as thighs lifting. Of these, three were men and nine women.
Of patients who underwent surgery of the lower segment, six patients (two males and four females) performed treatment of upper segment in a second time (Table 1).

Patients' age ranged from 24 to 52 years, a mean of 34 years.
The mean BMI of patients was 26.8 kg/m2.
The weight loss of patients ranged from 18 to 52 kilograms (kg), with an average of 35.5 kg.
The average surgical time in the circumferential excisions in the lower segment of the trunk was 4 hours and 8 minutes. In association with things lifting, the mean surgical time was 4 hours and 52 minutes. The mean surgical time in the upper segment of the trunk was 4 hours and 32 minutes.
The length of hospital stay in all cases was 24 hours.
The weight of the surgical parts of the abdomen and back ranged from 2.54 to 4.45 kg with an average of 4.06 kg. When associated with thighs lifting, the weight of the surgical specimens ranged from 2.98 to 5.42 kg, average of 4.93 kg. Treatment of upper segment of the trunk, associated with mammoplasty and brachioplasty, ranged from 1.98 to 2.66 kg, average of 2.34 kg.
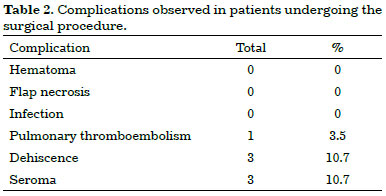
In our study, we observed three cases of small dehiscence (two cases in the back region and one in the thigh) and all were conservatively treated. There were also three cases of seroma (two cases and one case thigh in the abdomen) treated by punctures serial and lymphatic drainage and one case of pulmonary thromboembolism treated clinically.
No surgical complications were seen such as hematoma, flap necrosis and/or infection (Table 2).
In the ambulatorial follow-up 85.7% of patients reported to be very satisfied with the final result and no complaints were seen regarding the size and placement of the scars. Technical evaluation by the evaluator surgeon testified a degree of 92.8% of satisfaction with the result and the positioning of scars.
Figures 3 to 5 illustrate some cases this study.
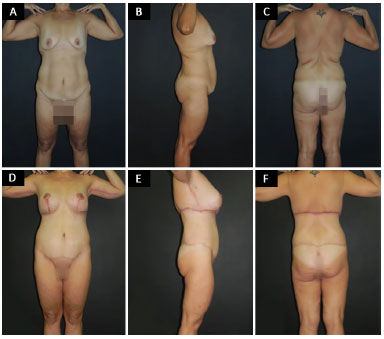
Figure 4. A 34-year-old patient who underwent circumferential excision with classical abdominoplasty in the first time followed by mammoplasty, and brachioplasty. A, B and C: Show result after surgery;. D, E and F: Show results 2-years after surgery.
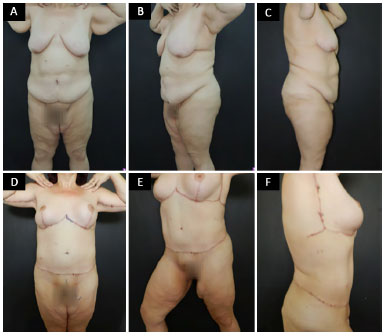
Figure 5. A 46-year old patient who underwent circumferential excision with classical abdominoplasty in a first time followed by mammoplasty, and brachioplasty. A, B and C: Show result after surgery. D, E and F: Show results 2-years after surgery.
DISCUSSION
The first report of abdominoplasty involving all abdominal circumference is dated from 1940 by Somalo. With the advent of bariatric surgery, there was an increase of interest in body contouring surgeries9-12.
The literature shows that many authors point to a concern for the harmonization of this segment. Gonzales-Ulloa characterized the "belt lipectomy" as treatment for abdominal segment with other body regions. In the 1980s Baroudi published several studies showing evidence with body contouring concern8,13,14.
The correct evaluation of deformities of the abdomen, chest, flanks, hips and thighs, allow a better approach in these regions, and significantly better results. Plastic surgery is intended to make the individuals feel better regarding their own expectations2,4.
Extensive associated circumferential excisions or non-satellite incisions provide patients with a considerable skin excess who had massive weight loss, the change of treating various body regions in one step.
Our experience reveals that large incisions, without prejudice concerning the extension, when well indicated, have advantages to treat excessive skin from the posterior region, elevate and better contouring of gluteal region, elevate the anterolateral thigh, besides treatment of the anterior abdomen.
The sample of our study was composed by 28 ex-obese patients who underwent circumferential excisions. Of these, 12 were associated with the thighs lifting and 8 to upper thoracic segment in a second time.
The study population included young men and women with a mean age of 34 years, and who had mean body mass index of 26.8 kg/m2. Our study data were similar to other studies reported in the literatura5,15,16.
The circumferential surgeries in the trunk segment may cause some postoperative complications. Arthurs et al.16 showed two types of complications in which patients who undergo this technique may develop minor and major complications. Main minor complications reported are seroma, hematoma, dehiscence and local infections. The major complications include large hematomas, deep venous thrombosis and pulmonary thromboembolism.
In our study minor complications were seroma and dehiscence. There were two cases of seroma in thighs and a case in the abdomen. Two cases had small dehiscence in the back region and one in the thigh, all cases were treated conservatively without compromise to final aesthetic result.
The most vulnerable point for occurrence of dehiscence in circumferential surgery of lower segment of trunk is located on the projection of the spine. A region that dermis-fat resections should be reduced. In our experience we had two small cases, which accounted for 7.14% of complications.
Regarding major complications, we had a case of pulmonary embolism in a patient diagnosed after sudden dyspnea. The patient underwent clinical treatment using low molecular weight heparin, and a significant improvement was seen.
The literature describes certain prophylactic methods for pulmonary thromboembolism, such as use of intermittent compression devices in lower limbs, early ambulation and use of low molecular weight heparin, which should be administered 12 hours after beginning of the surgery and fourth day after surgery17. Such methods are used at our service.
A crucial factor to be considered and respected in patients undergoing cosmetic surgery is the surgical time. Baroudi defined as limit for surgical time a period of 360 minutes. Surgical procedures that exceed this limit would cause major complications for patients in the postoperative period18.
In our study, average surgical time obtained in circumferential excisions, thighs lifting and treatment of upper segment of the trunk were 4 hours and 8 minutes, 4 hours and 52 minutes and 4 hours and 32 minutes, respectively.
The massive weight loss, 40-60% of weight loss, can cause deformities in different body segments. Such deformities are corrected by various surgical techniques and they generally require repeated surgeries depending on extent of the deformations affecting the entire body and trunk region.
Our experience with this type of technique provides reduction of surgical steps using systematizations that allow surgical procedures involving multiple body regions in less time and with certainty.
These systematizations enable treatment via extensive excisions of the circumferential type and associated satellites incisions. In addition, systematizations generate a reduction of future surgical procedures, represent less risk for patients, result in an improvement in patients' quality of life, and promote a reduction for costs to the society and health sector.
A lot of improvement has been achieved in terms of less prejudice and break paradigms concerning the extent of scars. A commitment has been done to provide better results in the format regardless the extent of the scar.
Large circumferences excisions allow the treatment of various body regions, provide greater harmonization, better aesthetical results to body segment. Results obtained in this study were similar to the Cintra Junior et al.15 that showed patient's satisfaction in 85.7% of cases, therefore, corroborating the fact that, when properly indicated, the extensive circumferential incision restores a harmonious appearance of the trunk segment regardless the size of the scar.
Despite the non-objective means were used to measure the results, this study had a high percentage of satisfaction both for patients (85.7% of cases) and for plastic surgeon evaluator (92.8% of cases). Our data were similar to those found in the literature that used similar techniques15.
The satisfactory results and low complication rates seen confirmed the applicability of this technique to ex-obese patients, mainly when indication is precise. The association of the correct surgical technique with adequate pre and postoperative care as well as trained surgical team are key to surgery success.
CONCLUSION
Extensive circumferential excisions and satellites provide to ex-obese patients an effective treatment to different body areas. This procedure also show low complication rate and acceptable scars due to the significant improvement in body contouring.
Satisfactory results of this study shed light on the safety and feasibility of the technique for correction of dermis-fat redundancies and the harmonization of the lower body segment.
COLLABORATIONS
JCD Final approval of the manuscript; completion of surgeries and/or experiments; writing the manuscript or critical review of its contents.
DASS Conception and design of the study; writing the manuscript or critical review of its contents.
CADCF Analysis and/or interpretation of data
BPE Writing the manuscript or critical review of its contents.
IRJ Conception and design of the study.
LGM Conception and design of the study.
LMCD Conception and design of the study.
MCAG Conception and design of the study.
REFERENCES
1. Moreno Esteban B, Zugasti Murillo A. Bariatric surgery: an update. Rev Med Univ Navarra. 2004;48(2):66-71. PMID: 15382616
2. Meira AAM, Andrade IF, Ferreira FPM. Cirurgia plástica após gastroplastia redutora: abordagem pré, per e pós-operatória. Rev Bras Cir Plást. 2008;23(1):15-21.
3. Rubin JP, Nguyen V, Schwentker A. Perioperative management of the post-gastric-bypass patient presenting for body contour surgery. Clin Plast Surg. 2004;31(4):601-10.
4. Vico PG, De Vooght A, Nokerman B. Circumferential body contouring in bariatric and non-bariatric patient. J Plast Reconstr Aesthet Surg. 2010;63(5):814-9. DOI: http://dx.doi.org/10.1016/j.bjps.2009.01.075
5. Modolin M, Cintra W Jr, Gobbi CI, Ferreira MC. Circumferential abdominoplasty for sequential treatment after morbid obesity. Obes Surg. 2003;13(1):95-100. DOI: http://dx.doi.org/10.1381/096089203321136665
6. Hurwitz DJ. Single-staged total body lift after massive weight loss. Ann Plast Surg. 2004;52(5):435-41. DOI: http://dx.doi.org/10.1097/01.sap.0000123361.14654.a5
7. Daher JC, Benedikt A, Faria CADC, Amaral JDG, Rodrigues Neto JN, Cosac OM, et al. Umbilicoplastia: experiência com a técnica do minicírculo de pele. Rev Bras Cir Plást. 2011;26(2):302-5.
8. Baroudi R, Ferreira CA. Seroma: how to avoid it and how to treat it. Aesthet Surg J. 1998;18(6):439-41. PMID: 19328174 DOI: http://dx.doi.org/10.1016/S1090-820X(98)70073-1
9. Baroudi R. Cirurgia do contorno corporal. Rio de Janeiro: Indexa Editora; 2009.
10. Somalo M. Dermolipectomia circular del tronco. Semana Med. 1940;47:1435.
11. Roxo CDP, Pinheiro O, Almeida D. Abdominoplastia Multifuncional. Rev Bras Cir Plást. 2004;19(3):64-74.
12. Roxo CDP, Roxo ACW, Roxo CW. Coxoplastia oblíqua em pacientes após grandes perdas ponderais. Rev Bras Cir Plást. 2012;27(1):119-23. DOI: http://dx.doi.org/10.1590/S1983-51752012000100020
13. Gonzales-Ulloa M. Circular lipectomy with transposition of the umbilicus and aponeurotic technique. Cirurgia. 1959;27:394-401.
14. Baroudi R. Flankplasty: a specific treatment to improve body contouring. Ann Plast Surg. 1991;27(5):404-20. PMID: 1746861 DOI: http://dx.doi.org/10.1097/00000637-199111000-00004
15. Cintra Junior W, Modolin M, Gobbi CIC, Gemperli R, Ferreira MC. Abdominoplastia circunferencial em pacientes após cirurgia bariátrica: avaliação da qualidade de vida pelo critério adaptativo. Rev Bras Cir Plást. 2009;24(1):52-6
16. Arthurs ZM, Cuadrado D, Sohn V, Wolcott K, Lesperance K, Carter P, et al. Post-bariatric panniculectomy: pre-panniculectomy body mass index impacts the complication profile. Am J Surg. 2007;193(5):567-70. DOI: http://dx.doi.org/10.1016/j.amjsurg.2007.01.006
17. Cintra Junior W. Abdominoplastia circunferencial simples e composta: evolução técnica, experiência de 10 anos e análise das complicações [Tese de doutorado]. São Paulo: Universidade de São Paulo; 2014.
18. Baroudi R. A segurança nas cirurgias estéticas combinadas. Rev Bras Cir Plást. 2010;25(4):581-2. DOI: http://dx.doi.org/10.1590/S1983-51752010000400002
1. Sociedade Brasileira de Cirurgia Plástica, São Paulo, SP, Brazil
2. Hospital Daher Lago Sul, Brasília, DF, Brazil
Institution: Hospital Daher Lago Sul, Brasília, DF, Brazil.
Corresponding author:
Daniel Augusto dos Santos Soares
CCSW 02, Lote 03, Ed. Unique Duplex, Apt 105, - Sudoeste
Brasília, DF, Brazil - Zip Code 70680-250
E-mail: daniel.soares@globo.com
Article received: September 17, 2016.
Article accepted: July 9, 2017.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket