



Original Article - Year 2017 - Volume 32 -
Pyriform plasty associated with open rhinoplasty
Piriformeplastia associada à rinoplastia aberta
ABSTRACT
INTRODUCTION: Mouth or mixed breathing since childhood that is due to allergy factors causing turbinate hypertrophy and adenoids, or traumatic septal deviation at childbirth or first trauma in childhood leads to the impairment of facial development, including ogival palate, excessive growth of the maxillary crest, changes in the dental arch, and small jawbone. Mouth or mixed breathing may be due to the lack of aeration of the paranasal sinuses. A septum with limited space for growing pushes the osteocartilaginous framework cranially, originating from the nasal hump with septal deviations and gibbus. Consequently, this hampers nasal breathing.
METHOD: Pyriform plasty by incision in the gingivolabial sulcus allows broad access to the maxillary crest and ogival palate. The maxillary crest is worn out with a drill, and the palate is modeled or may have its dome subperiosteally removed.
RESULTS: Open rhinoplasty facilitates the approach and fixation of graft reamers to treat changes in the internal valve and prevents scar reactions at the level of the cage cartilage grafts and structure of the columella to project and prevent a cartilaginous scar retraction at this level. The open approach also enables the symmetrization of nasal structures, which allows the treatment of bent nose at a single time, and correction of nasal valve by using external grafts. Moreover, pyriform plasty is a more comprehensive approach to nasal aesthetic and functional nasal alterations.
CONCLUSION: Our preferred techniques are open rhinoplasty, given the ease of graft fixation, and use of reamer grafts to treat changes in the internal valve to prevent future respiratory problems.
Keywords: Reconstructive surgical procedures; Rhinoplasty; Pyriform sinus.
RESUMO
INTRODUÇÃO: A respiração bucal ou mista desde a infância, por fatores alérgicos que causam hipertrofia de cornetos e adenoides ou desvio septal traumático no parto ou por traumas na primeira infância, provoca incorreto desenvolvimento da face com o palato ogival, crescimento excessivo da crista maxilar, alterações na arcada dentária e hipomaxilismo, por falta de aeração dos seios paranasais. O septo com limitado espaço para de crescer empurra o arcabouço osteocartilaginoso cranialmente, originando a giba nasal com desvios do septo, comprometendo a respiração nasal.
MÉTODO: A piriformeplastia mediante incisão no sulco gengivolabial permite amplo acesso à crista maxilar e ao palato ogival. A crista maxilar é desgastada com broca e o palato é modelado ou pode ter sua cúpula removida subperiostealmente.
RESULTADOS: A rinoplastia aberta facilita a abordagem e a fixação dos enxertos alargadores para tratar as alterações da válvula interna e prevenir retrações cicatriciais ao nível da gaiola cartilaginosa, além dos enxertos estruturais na columela para projeção e evitar retração cicatricial neste nível. A abordagem aberta permite também a simetrização das estruturas nasais, que possibilita o tratamento das laterorrinias num tempo único e a correção da válvula nasal externa por meio dos enxertos específicos. A piriformeplastia permite ainda a abordagem mais abrangente das alterações nasais estéticas e funcionais.
CONCLUSÃO: A rinoplastia aberta é por nós preferida dada a facilidade de fixação dos enxertos, bem como dos enxertos alargadores para tratamento das alterações da válvula interna com o objetivo de prevenir futuros problemas respiratórios.
Palavras-chave: Procedimentos cirúrgicos reconstrutivos; Rinoplastia; Seio piriforme.
In the opinion of most surgeons, rhinoplasty is the most difficult and challenging aesthetic cosmetic surgery. It is even considered as a game of chess in which the opponents are the surgeon and the nasal anatomy1.
The approach must be specific. Each case must be diagnosed correctly, and the surgeon must be able to determine the etiology of deformities to establish the surgical plan. Then, the surgeon must be direct and unequivocal to reconstruct the skeleton and achieve the desired aesthetic result. However, the unknown variable is the postoperative healing and its subsequent retraction by fibrosis.
Thus, the concept of structured rhinoplasty and the strategies used by the author to counter scar retraction, for which open rhinoplasty is the preferred technique for better fixation of structural grafts, have obtained greater predictability of results. This is due to an unpredictable factor, which is the process of scar retraction1-6.
The correct growth and development of the face depends on the passage of air through the nose. Mouth or mixed breathing since childhood due to allergic processes or nasal trauma contributes to the elevation of the palate and maxillary crest. The ogival palate exerts pressure on the septum and bends, transmitting the pressure to the nasal dorsum, causing its elevation1. Therefore, for the complete treatment of nasal respiratory dysfunctions, the dome of the palate must be removed when it enters the pyriform cavity, and its height should be reduced or the maxillary crest is removed to release the passage of air in a correct laminar flow7,8.
Therefore, the pyriform plasty becomes necessary in cases of stenosis of the pyriform cavity, either congenital (Figure 1A) or acquired throughout life because of mouth or mixed breathing (Figure 1B).
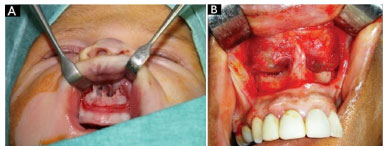
Figure 1. Hypertrophic crest. A: Congenital; B: Acquired in adulthood.
To treat the palate and maxillary crest, the author chooses access by an incision in the gingivolabial sulcus, which provides extensive exposure of the structures7-9.
OBJECTIVE
Pyriform plasty through the gingivolabial sulcus allows broad access for treatment of the ogival palate and maxillary crest, offering structural conditions of the anatomy, favoring nasal breathing, and avoiding the growth of a dorsal hump as from puberty.
METHODS
The preoperative photographs and computed tomography images that show changes in the maxillary crest, which are often asymmetrical (one side longer than the other); the palate moving into the pyriform cavity; septal deviations; conchae hypertrophy; bullous conchae; and permeability of drainage ostia of the sinuses (Figure 2) should be exposed in the operating room.

Figure 2. Computed tomography scan showing an ogival palate and hypertrophied maxillary crests; the larger one is to the left.
Surgery is performed under general anesthesia, with endotracheal intubation. The nose and gingivolabial sulcus are infiltrated with saline and adrenaline 1:100,000. The access path can be performed through the gingivolabial sulcus or exo-rhinoplasty.
Surgery is initiated by exo-rhinoplasty, followed by nasal and septal dissection bilaterally, maintaining the integrity of the septal cartilage. Then, an incision is made in the gingivolabial sulcus, and dissection of the maxillary crest is performed in the subperiosteal plane. The nasal spine is bypassed in the same subperiosteal plane, reaching the lower ridge of the septal cartilage. At that moment, the subperichondrial dissection of the septum begins bilaterally, which coincides with the previously dissected plane via exo-rhinoplasty. By advancing the dissection posteriorly to the maxillary crest, the floorboards of the pyriform cavity are reached, which is dissected in the subperiosteal plane7,8 (Figure 3).

Figure 3. Subperiosteal dissection of the floor of the pyriform cavity and subperichondrial septum.
After the junction of the dissected subperichondrial (septum) and subperiosteal (nasal floor) planes, the broad space obtained allows treatment of the septum, maxillary crest, and nasal floor, including removal of the dome of the ogival palate when needed7,8 (Figure 4A, B and Figure 5A, B).
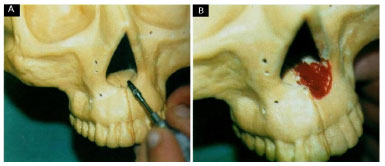
Figure 4. A and B: Scarification of the maxillary crest and floor of the pyriform cavity.
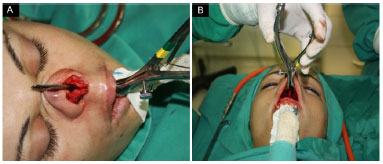
Figure 5. A and B: Communication between the two access routes.
Scarification of the maxillary crest and palate is attained with an electric drill. It stretches throughout the bony palate.
After the pyriform plasty, the intraoral access is sutured according to the planes as follows: nylon 3.0 for the muscular plane and catgut 5.0 for the oral mucosa. Finally, exo-rhinoplasty is resumed to complete the aesthetic surgery of the nose according to the modern concepts of rhinoplasty3,10 (Figure 6 A and B).
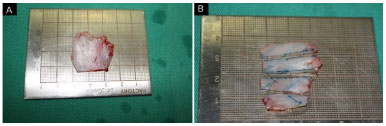
Figure 6. A and B: Removal of a portion of the septum and its division for manufacturing structural grafts.
Structured rhinoplasty is used to avoid the phenomena of scar retraction; consequently, this provides greater predictability of the surgical outcome. The grafts are fixed with a nylon 5.0 cylindrical needle (Figure 7).

Figure 7. Structural grafts positioned.
RESULTS
In the last 8 years, 68 patients were treated surgically. Of these patients, 38 were female and 30 were male. They were aged between 22 and 62 years. In the women, aesthetic complaints were prevalent; however, they had varying degrees of nasal obstruction. By contrast, the men had more functional complaints and the greatest degrees of nasal respiratory dysfunction.
Sixty of the 68 patients reported nasal respiratory improvement of 90% to 100%. Eight of the 60 patients reported improvement of 70% to 80%. This difference was interpreted by the author as being due to a greater degree of respiratory allergy present in the eight patients. Figure 8 shows a patient with a typical face of a mouth breather. She presented a bent nose, a deviated septum, an ogival palate, and a hypertrophied maxillary crest. She was submitted to pyriform plasty associated with open rhinoplasty. The structural grafts were withdrawn from the nasal septum.

Figure 8. A patient aged 32 years who underwent pyriform plasty during open rhinoplasty.
The author uses the Glatzel test only as an objective parameter for preoperative and postoperative comparisons. Nevertheless, the author considers that the subjective aspect reported by the patient is more significant11 (Figure 9).
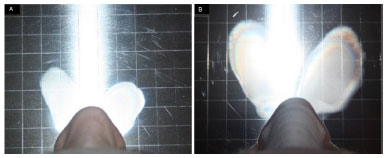
Figure 9. A patient aged 26 years who underwent pyriform plasty during open rhinoplasty. A: Preoperative Glatzel test (maximum forced expiration); B: Ten days after operation (maximum forced expiration).
DISCUSSION
The intraoral approach is necessary for the treatment of hypertrophic maxillary crests and the palate bone when its excessively enters the pyriform cavity, improving nasal airflow. The simple treatment of the septum and turbinates leads to transitory results, with a high rate of functional recurrences, as the functional improvement is due to the treatment of turbinates or nasal conchae in most cases. Nonetheless, as most cases of respiratory dysfunction occur throughout life since childhood, bone changes that should be treated together with the septum and turbinates will occur under functional recurrence in a short period.
CONCLUSION
The author understands that pyriform plasty should be performed in all cases of respiratory dysfunction that allow for broad and straight treatments of all the structures involved. Moreover, open rhinoplasty allows more control and predictability of aesthetic results, especially because it facilitates fixation of structural grafts that will counter the forces of scar retraction.
COLLABORATIONS
RSS Analysis and/or interpretation of data; completion of surgeries and/or experiments.
AMR Literature search; support for research paper writing.
RB Final approval of the manuscript; writing the manuscript or critical review of its contents.
REFERENCES
1. Sheen JH, Sheen A. Aesthetic Rhinoplasty, Volume I. St. Louis: Quality Medical Publishing; 1998. 174 p.
2. Cardim VLN. Crescimento ósseo e cartilaginoso da face. In: Avelar JM. Cirurgia Plástica na Infância. São Paulo: Hipócrates; 1989. p. 190-200.
3. Günter JP, Rhorrich RJ, Adams WP Jr. Dallas Rinoplastia - Cirurgia de nariz por mestres. Rio de Janeiro: Revinter; 2006. p. 726-729.
4. Costa LF, Muñoz AM, López D, Melo JC, Nahon MA. Exorrinoplastia para tratamento da ponta nasal bulbosa. Rev Bras Cir Plást. 2005;20(2):72-81.
5. Lintz JE. Análise comparativa das rinoplastias aberta e fechada no tratamento da ponta nasal. Rev Bras Cir Plást. 2009;24(3):286-95.
6. Pizarro GU, DeVuono IM, Moyses MG, Fujita RR. Rinoplastia aberta. Rev Bras Otorrinolaringol. 2002;68(3):332-5. DOI: http://dx.doi.org/10.1590/S0034-72992002000300007
7. Cardim VLN. Abordagem das alterações faciais do respirador bucal. In: XXXVII Congresso Brasileiro de Cirurgia Plástica; 2000 Nov 15; Porto Alegre, RS, Brasil.
8. Colombini NEP. Cirurgia da Face: Interpretação funcional e estética síndrome da apnéia do sono: enfoque maxilo-facial e otorrinolaringológico, Volume II. Rio de Janeiro: Revinter; 2002. p. 613-614.
9. Fortes FAB, Tostes F. Abordagem externa nas rinosseptoplastias. Rev Bras Cir Plast. 1997;12(1):33-40.
10. Sesenna E, Leporati M, Brevi B, Oretti G, Ferri A. Congenital nasal pyriform aperture stenosis: diagnosis and management. Ital J Pediatr. 2012;38:28. DOI: http://dx.doi.org/10.1186/1824-7288-38-28
11. Brescovici S, Roithmann R. A reprodutibilidade do espelho de Glatzel modificado na aferição da permeabilidade nasal. Rev Bras Otorrinolaringol. 2008;74(2):215-22. DOI: http://dx.doi.org/10.1590/S0034-72992008000200010
1. Sociedade Brasileira de Cirurgia Plástica, Uberaba, MG, Brazil
2. Faculdade de Medicina, Universidade de Uberaba, Uberaba, MG, Brazil
3. Sociedade Brasileira de Cirurgia Plástica, São Paulo, SP, Brazil
Institution: Universidade de Uberaba, Uberaba, MG, Brazil.
Corresponding author:
Renato Sivieri de Souza
Rua Vigário Silva, 750 - Centro
Uberaba, MG, Brazil Zip Code 38022-190
E-mail: rsivieri@terra.com.br
Article received: April 3, 2017.
Article accepted: May 8, 2017.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket