



Case Report - Year 2015 - Volume 30 -
Bilabial double lip
Lábio duplo bilabial
ABSTRACT
There are few published reports on double lip, a rare entity that usually affects the upper lip, and that is easily diagnosed clinically. It may be congenital or acquired. Surgical treatment is indicated for aesthetic or functional complaints, and is simple to implement. This report describes a case of bilabial double lip in a 14-year-old male patient, in whom surgical correction was carried out for aesthetic reasons, with excellent aesthetic and functional results.
Keywords: Lip; Lip abnormalities; Salivary glands; Reconstructive surgical procedures.
RESUMO
O lábio duplo é uma entidade rara, com poucos relatos, que geralmente afeta o lábio superior, sendo de fácil diagnóstico clínico. Pode ter origem congênita ou adquirida. O tratamento cirúrgico é indicado por queixa estética ou funcional, de simples execução. Este relato refere-se a um caso de lábio duplo bilabial em paciente do sexo masculino de 14 anos, em que foi realizada correção cirúrgica por motivação estética do paciente, com ótimo resultado dos pontos de vista estético e funcional.
Palavras-chave: Lábio; Lábio/anormalidades; Glândulas salivares; Procedimentos cirúrgicos reconstrutivos.
There are few published reports on the deformity of double lip. The altered labial mucosa is characterized by hypertrophy of the minor salivary glands, accompanied by a redundancy of mucosa, without muscular involvement. It is most frequently observed in the upper lip (10:1), generally affects only one lip, and is rarely bilabial1.
Its origin can be congenital or acquired. There are no reports of hereditary, consanguinity, race, or gender factors2. The alteration is barely noticeable before dental eruption or with the lips at rest, but an exuberant mass is observed when the lips are stretched3, as when the patient smiles.
OBJECTIVE
To report a rare case of bilabial double lip, discuss the deformity, and describe the surgical technique used for its correction and the outcome obtained with the treatment.
MATERIALS AND METHODS
A 14-year-old male presented with an altered lip, with the complaint of increased volume in both lips at the beginning of puberty. The patient had no family history of deformity or local trauma. Findings consistent with Ascher's syndrome were not identified.
Examination with the lips at rest showed an increase in lip volume, without a precisely defined double lip. With the contraction of the lips, projections of the labial mucosa of the upper and lower lips became evident, with a narrowing in the middle region (Figure 1 and 2). The mucosa showed no change in color or consistency, or signs of previous trauma.

Figure 1. Preoperative aspect. Upper and lower double lip.
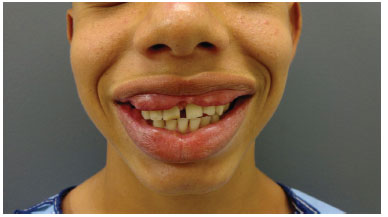
Figure 2. Details of the lips, with greater exposure when smiling.
Correction in two surgical stages was indicated. The procedures were performed in an outpatient setting under local anesthesia and sedation. The mucosal area to be resected was marked, due to the risk of distortion after infiltration with local anesthetic solution. Prophylactic antibiotics were infused during the intraoperative period. After anesthetic infiltration, two elliptical incisions were made with a scalpel, involving the areas of mucosal hypertrophy on the upper lip, without involving the philtrum, and resection was performed with an electric scalpel. Local hemostasis was performed with compression and an electric scalpel. Suturing was completed with simple catgut 4.0, in deep and superficial layers. The same procedure was performed on the lower lip 47 days later (Figure 3 and 4).

Figure 3. Intraoperative aspect. Resection of excess tissue and hypertrophic glands.

Figure 4. Intraoperative aspect. Result at the end of surgery.
RESULTS
The resected tissue was sent for histopathological analysis, which reported salivary glands and a chronic nonspecific inflammatory reaction, with acanthosis and hyperkeratosis in the mucosa.
We observed excellent results at the postoperative follow up, with an appearance of normal lips, no functional loss, and complete patient satisfaction (Figure 5).

Figure 5. Postoperative period. After 2 months.
DISCUSSION
Double lip consists of a congenital or acquired fold of mucous membrane, more often on the upper lip, which may be due to trauma, or have unknown causes. Some authors suggest that the habit of sucking the lips or bad dental occlusion can be causes of repeated trauma to the labial mucosa, causing the double lip. This case was a bilabial double lip, which has rarely been reported in the literature4-6. It is more visible than unilabial double lip, and causes greater embarrassment for the patient.
Differential diagnoses of double lip include inflammatory fibrous hyperplasia, fibroma, lipoma, hemangioma, lymphangioma, localized angioedema, and Melkersson-Rosenthal syndrome7.
Ascher's syndrome, which presents with the triad of double lip, blepharochalasis, and nontoxic goiter, but is not always present in its complete form, must also be considered4. Generally, the labial alterations appear simultaneously with blepharochalasis, with a late onset of goiter in 10% to 50% of the patients. In 80% of cases, the syndrome manifests before age 20. Treatment can be initiated with dapsone to slow the progression of the syndrome4. Its etiology is unknown, but there is evidence for a defect in elastic fibers. Possible etiological hypotheses described are autosomal dominant inheritance and hormonal and allergic dysfunction8.
The recommended treatment is surgical, with few techniques described, but all with satisfactory results. The most frequently used technique is the double elliptical incision, due to ease of implementation and excellent results1, and was chosen for this patient. There is a need for a careful assessment of the amount of tissue to be removed, to prevent a very thin lip in the postoperative period. One can also perform a W-plasty, advocated by some for a better result, even if an excessive amount of tissue is removed, for better control of the anatomy and the aesthetics of the lip5. Another technique is the isosceles triangle resection, which is less often used, with parallel incisions on the labial frenum; it allows good identification of the tissue to be resected and the preservation of the frenum5.
There are reports of recurrence after surgical treatment.
Consistent with the literature, there was no involvement of the orbicularis oris muscle in the case described, only mucous tissue; there may be presentation with normal or hypertrophied minor salivary glands1.
CONCLUSION
Double lip is a rare deformity, especially with involvement of the upper and lower lips (bilabial). Histologically, it consists of hyperplasia of the salivary glands and labial mucosa. The treatment is surgical resection of the excess tissue, with excellent results.
The importance of the recognition of this entity is based on the need to avoid costly and extended investigation of an easily recognized anomaly upon clinical examination, which has a simple treatment.
REFERENCES
1. Azenha MR, Marzola C, Pereira lC, Brandt Filho SHO. Lábio duplo de origem congênita: relato de caso e técnica cirúrgica. Rev Bras Odontol. 2007;64(3-4):152-4.
2. Reddy KA, Roa AK. Congenital double lip: a review of seven cases. Plast Reconstr Surg. 1989;84(3):420-3. PMID: 2762400
3. Flores JA, Krüger FL. Lábio duplo. Rev Gauch Odontol. 2002;50(3):172-4.
4. Santos PP, Alves PM, Freitas VS, Souza LB. Double lip surgical correction in Ascher's syndrome: diagnosis and treatment of a rare condition. Clinics (Sao Paulo). 2008;63(5):709-12. DOI: http://dx.doi.org/10.1590/S1807-59322008000500022
5. Bourguignon Filho AM, Pandolfi S, Cypriano RV, Cançado RP, Puppin AAC, Rezende RA, et al. Lábio duplo: relato de caso. Rev Int Cir Traumatol Bucomaxilofacial. 2005;3(9):21-5.
6. Friedhofer H, Tuma Junior P, Bonamichi GT, Goldenberg DC, Ferreira MC. Associação de lábio duplo congênito superior e inferior. Rev Hosp Clin Fac Med Univ São Paulo. 1991;46(3):126-7.
7. Brinhole MCP, Real DG, Giovani EM, Costa C, Armonia PC, Melo JAJ, et al. Lábio duplo congênito. Rev Inst Ciênc Saúde. 2006;24(4):327-30.
8. Carraro RRIV, Pacheco AS, Zanardi D, Souza Filho JJ. Você conhece esta síndrome? An Bras Dermatol. 2006;81(3):287-9.
1. Hospital Alemão Oswaldo Cruz. São Paulo, SP, Brazil
2. Sociedade Brasileira de Cirurgia Plástica. São Paulo, SP, Brazil
Institution: Conjunto Hospitalar do Mandaqui, São Paulo, SP, Brazil.
Corresponding author:
Gustavo Felipe Pasqual
Rua Voluntários da Pátria, 4110 - Santana
São Paulo, SP, Brazil Zip code 02402-500
E-mail: pasqual.gu@ig.com.br
Article received: January 7, 2012.
Article accepted: April 21, 2012.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket