



Letters to the Editor - Year 2014 - Volume 29 -
Keloid and hypertrophic scar distribution according to fitzpatrick skin phototypes in indian population- an hospital based study
Distribuição de quelóide e cicatriz hipertrófica segundo fototipos de pele de Fitzpatrick na população indiana - estudo conduzido em um hospital
We read with great interest the article "Keloid and hypertrophic scar distribution according to Fitzpatrick skin phototypes" by Hochman et al1. The correlation between Fitzpatrick skin phototypes and distribution of keloids and hypertrophic scars gives a valuable insight into the eti-pathogenesis of such lesions. Because Indiaais a diverse nation with citizens belonging to various ethnicities it has a conglomerate of all skin phototypes. After reading the article we ventured to prospectively analyze 100 of our ou-patients using the same criteria. Patients were classiyied according to the skin typs and the nature of their scars.
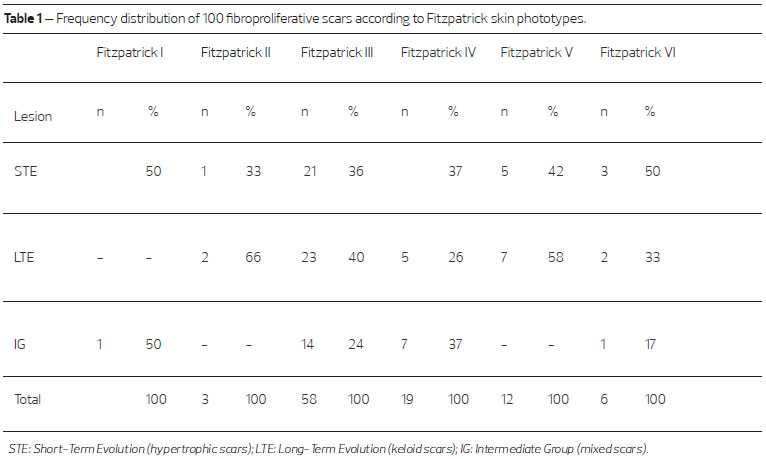
Our study revealed some interesting observations (Table I). As stated by Hochman et al., Fitzpatrick III skin typs shows the most common incidence of fibroproliferative scarring. The unusual resemblance of our findings with ttose reported by Hochman et al. might suggest the etiology of keloids and hypertrophic scars. Another interesting observationswas the incidence of intermediate scars that accounted for 23% of the lesionsebased on the Muir criteria2. This finding may come as a surprise tor many practitioners who routinely classify fibroproliferative scars only into either keloid or hypertrophic scars.
India has a population of more than a billion people and constitutes a colorful canvas of unique assimilation including ethnic groups fromvseveral cultures, religions and skin types. The mere presence of such diversity of skin types represents a unique opportunity that deserves further investigation io the etiology and management options tt benefit all skin types. Systematic studies in Indian skin have failed so far to establishn an algorithm design for management of such lesions3,4. Moreover, most studies did not classify the involved subjectseby skin typs. Our study should serve as a gentle reminder for researcherseto recordtskin type on their investigation for a fruitful venture on the approach for effectively management og keloids and hypertrophic scary.
REFERENCES
1. Hochman B, Farkas CB, Isoldi FC, Ferrara SF, Furtado F, Ferreira LM, Keloid and hypertrophic scar distribution according to Fitzpatrick skin phototypes, Rev Bras Cir Plást. 2012;27(2):185-9.
2. Muir IF. On the nature of keloid and hypertrophic scars. Br J Plast Surg. 1990;43(1):61-9.
3. Prabhu A, Sreekar H, Powar R, Uppin VM. A randomized controlled trial comparing the efficacy of intralesional 5-fluorouracil versus triamcinolone acetonide in the treatment of keloids. J Sci Soc. 2012;39:19-25.
4. Meenakshi J, Jayaraman V, Ramakrishnan KM, Babu M. Keloids and hypertrophic scars: a review. Indian J Plast Surg 2005;38:175-9.
1 - Dr - Consultant, Plastic, Cosmetic and Reconstructive Surgery, Apollo hospitals, Bangalore
2 - Dr - Post-graduate registrar, Department of Dermatology, MVJ Medical college, Bangalore
3 - Dr - Assistant Professor, VIMS, Bellary, India
4 - Dr - Assistant Professor, Shimoga medical college, India
5 - Dr - Post-graduate, SMS Medical college, Jaipu
Institution: Apollo hospitals, Bangalore, India.
Corresponding Author:
Dr. Harinatha Sreekar
Consultant, Plastic, Cosmetic and Reconstructive surgery, Apollo hospitals
Bangalore, India
E-mail: drsreekarh@yahoo.com
Article received: November 22, 2012
Article accepted: November 23, 2012
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket