



Special Article - Year 2014 - Volume 29 -
Aesthetic treatment of retracted and hanging nasal columellas
Tratamento estético da columela nasal: columela oculta e columela pendente
ABSTRACT
This study discusses approaches for aesthetic correction of nasal columellas, i.e. retracted and hanging columellas, most commonly observed in clinical practice. We describe a chondral-mucoperichondrial nasal septal flap and direct or indirect approaches described by Randall as our preferred procedures to correct retracted and mild to moderate hanging columella, respectively. A combination of procedures is used in more severe cases, in addition to modified Armstrong and Joseph's approaches. These treatment options are compared to other literature reports on this specialty.
Keywords: Nose Surgery; Rhinoplaty Methods; Columella Aesthetics.
RESUMO
Os autores revelam, no presente trabalho, suas abordagens frente às alterações estéticas da columela nasal, mais observadas em sua prática clínica, a columela oculta e a columela pendente. Para a columela oculta os autores descrevem o uso de um retalho condro-mucopericondral do septo nasal como escolha preferencial. Para o tratamento da columela pendente os autores utilizam as abordagens, direta e indireta, descritas por Randall, nos casos leves a moderados, e para os casos mais acentuados utilizam uma associação de táticas além de uma modificação do que é descrito por Armstrong e Joseph. Suas opções de tratamento são confrontadas com o que há descrito na literatura da especialidade e seus resultados comparativos são apresentados.
Palavras-chave: Nariz Cirurgia; Rinoplastia Métodos; Columela Estética.
Descriptions of rhinoplasty procedures have been widely published in the literature1. Similarly, there is abundant literature for the correction of nasal columella deformities in cleft lip and palate as well as "negroid nose"2. However, few authors have reported their experiences in aesthetic alterations of nasal columella3-14. The aim of this study is to describe our approach for aesthetic alterations of the nasal columella most commonly observed in our clinical practice; i.e. retracted and hanging columellas. Our preferred treatment option is compared with other literature available on this specialty 3,15.
Perfect columella and treatment of columella disharmonies
Several authors have defined anatomical aspects of the perfect columella and its normal variations (2, 4-14, 16). Sheen reports that the perfect relationship between the columella and alar rims should not exceed 2-3 mm below a line parallel to their inferior border, on a profile view (4). Gunter proposed a systematic method of classification of ideal alar-columellar relationships (Figure 1) and their variations. The Gunter classification system includes six subtypes, from I to VI; the respective treatment options for each subtype are based on thorough analysis of actual images from hundreds of patients 5 (Figure 2).
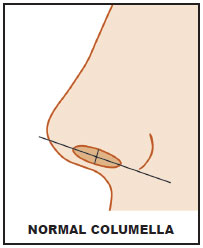
Figure 1. A normal columella Schematic representation of the ideal alar-columellar relationship
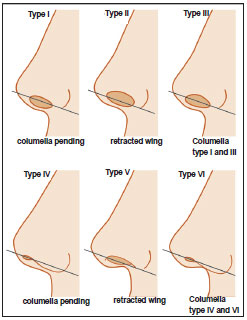
Figure 2. The Gunter classification of alar-columellar relationships The Gunter classification includes five subtypes. Type I, II, IV and V refer to primary deformities. Types III and VI refer to a combination of alterations observed in Types I and II, and Types IV and V, respectively.
The Gunter classification is accepted as the most complete system, although other authors have questioned the clinical feasibility of this classification method6. Hence, the Gunter classification is, for us, a didactic reference that allows comparison of normal patterns with morphological alterations of alar-columellar relationships.
We analyzed morphological alterations of nasal columellas whose anatomical characteristics were most commonly observed in our practice. We believe that hanging and retracted columella, as described by Gunter, represent the most frequent deformities. We refer to Gunter's "retracted columella" as "hidden columella." Alterations can be primary or secondary. Primary alterations are usually treated with aesthetic rhinoplasty or minor procedures that directly target the problem area. To correct outcomes that do not meet expectations, mostly in secondary cases, a combination of more than one procedure may be required, depending on the complexity of the case.
We describe our preferred options for treatment of aesthetic disharmony of hidden and hanging nasal columellas, and compare these options to other procedures described in the literature.
Hidden columellas
Hidden columellas (Gunter Type V) are one of the most commonly described columellar aesthetic disharmonies5 (Figure 2).
This condition usually manifests in elderly patients as acute columellar-labial angle and longer lip. Aging introduces new variables to rhinoplasty. The aged nose lacks suspensory ligament support, and it is characterized by soft tissue atrophy, caudal nasal tip rotation, sharpening of the columellar-labial angle, and divergent "footplates" that result in the appearance of columellar shortening. Bone absorption in the anterior nasal spine and jaw leads to retraction of posterior portions of the columella and redundant membranous septum (Figure 3)7.
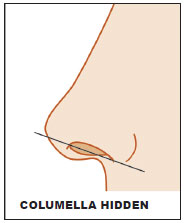
Figure 3. Hidden columella Schematic representation of hidden columella, known as retracted columella or Type V columella, according to the Gunter classification. It normally occurs in elderly patients with acute columellar-labial angles.
Flowers et al. describes creating a decorticated dermis flap from the nasal base area that is subsequently inserted through the columella and fixed to the nasal tip as an alternative to alloplastic implants, grafts, and hidden columellar fillings8. Haddad reported using a similar flap to correct acute columellar-labial angles9. Toriumi et al. describes the use of septal cartilage extension graft to correct hanging columellas10. (Figure 4)
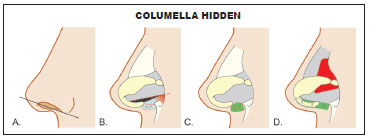
Figure 4. Treatment options for correcting hidden columella (A) Schematic representation of hidden columella. (B) Chondral-mucoperichondrial nasal septal flap is our preferred choice. (C) Cartilage graft on the anterior nasal spine. (D) Structural graft, "STRUT" type, in the crux medialis.
In our clinic, hidden columellas are treated with a chondral-mucoperichondrial flap created from the excess portion of the quadrangular cartilage. Positioning of the flap can be carried out in a single procedure or in combination with the different treatment options described above (Figure 5).
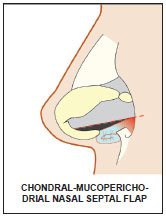
Figure 5. A chondral-mucoperichondrial nasal septal flap Schematic representation of a chondral-mucoperichondrial nasal septal flap positioned on the anterior nasal spine, according to nasal topography, restoring the columellar-lip angle within the standards established by treating hidden columellas.
Chondral-mucoperichondrial nasal septal flap
In cases with redundant septal cartilage also indicated for nose shortening, the resected caudal segment can be used to create a decorticated flap of the caudal septum mucosa. Before being discarded, excess cartilage is folded with relaxing incisions, thus adding volume to the anterior nasal spine area. This method is used for maintaining the intact perichondrium while preserving primary vascularization of this cartilage (Figure 6).
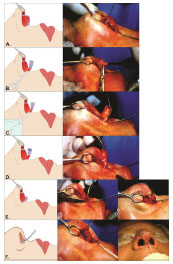
FIGURE 6. Surgical sequence of the chondral-mucoperichondrial flap (A) Demarcation of excess quadrangular cartilage portion. (B) The excess segment is cut up to the attachment of the maxillary crest. (C) The distal segment mucosa is carefully decorticated while maintaining perichondrium integrity. (D) Partial-thickness relaxing incisions are made on the cranial segment of the flap to facilitate its folding. (E) Once folded, the flap is molded with 5-0 nylon sutures. (F) Finally, the flap is positioned on the anterior nasal spine according to nasal topography and stabilized with externally fixed 6-0 nylon thread that is maintained for 7 days.
This procedure corrects closed columellar-labial angles and facilitates cranial rotation of the nasal tip, as desired. A 6-0 nylon thread stabilizes the flap, which is externalized and fixed around the nasal spine, and removed 7 days after surgery (Figure 7).
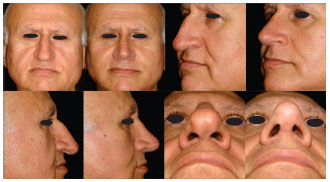
Figure 7. External fixation of a chondral-mucoperichondrial nasal septal flap The flap is stabilized using an external fixation suture with 6-0 nylon, externalized to the level of columellar-labial angle, and maintained for 7 days.
The chondral-mucoperichondrial nasal septal flap is our treatment of choice compared to grafts, as we observe a certain degree of volume absorption of grafted cartilage. Conversely, as the flap maintains primary vascularization, it provides stable and satisfactory outcomes. We use this flap for both open rhinoplasty and endonasal approaches (Figures 8 and 9).
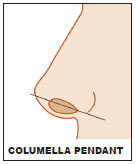
FIGURE 8. Pre and post-operative aspect of a patient treated with chondral-mucoperichondrial flap. Negroid nose with hidden columella was corrected with chondral-mucoperichondrial flap.
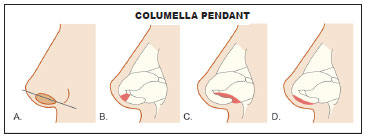
Figure 9. Pre and post-operative aspect of a patient treated with chondral-mucoperichondrial flap. Long nose with acute columellar-labial angle and subsequent hidden columella. Patient operated by open approach with chondral-mucoperichondrial flap, lowering the osteocartilaginous dorsum, columellar strut, and resection of the cephalic portion of the lower lateral cartilages.
Hanging columellas
Hanging columellas are a common aesthetic problem characterized by accentuated curvature of the caudal edge of the columella and subsequent skin exposure of the membranous septum11. Hanging columellas are Gunter Type I and may be associated with alar retraction; i.e. Type II. The combination of Type I and Type II characteristics in these cases corresponds to Type III classification5 (Figure 10).
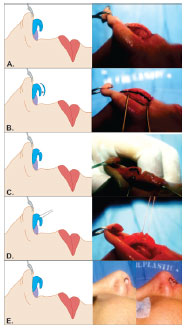
Figure 10. Schematic representation of a hanging columella A hanging columella classified as Type I according to the Gunter classification.
Matarasso simplifies the diagnosis by classifying hanging columellas as true or false6. This proposed classification takes into account four reference profile views: 1- the nasal septal mucosal area, 2- the alar rim border, 3- the mid-line portion of the columella, and 4- subnasal angle. True hanging columellas occur in the presence of lower projection of crux medialis cartilages and are usually congenital. Correction requires the removal of excess quadrangular cartilage, membranous septum, or, in extreme cases, crux medialis cartilages. False hanging columellas are characterized by iatrogenic alar rim retraction due to excessive resection of inferior lateral cartilages; correction of this deformity requires a direct approach to the alar rim.
Accurate diagnosis is essential to determine optimal treatment, as each deformity requires a different approach. However, in cases of false hanging columellas, a combination of treatments may be required6.
Randall describes two treatment options for hanging columellas. The "indirect" approach, in which excess septal cartilage or redundant membranous septum are removed, is used in mild to moderate cases, whereas a "direct" approach is recommended for more severe cases or those resulting from unsuccessful surgeries. This procedure removes distal segments of the crux medialis11, 12. Armstrong described an "aggressive" approach for hanging columellas, in which the crux medialis is completely removed as well as excess skin and mucosa of the membranous septum. He also reported that this procedure preserves nasal tip support12. Joseph et al. described a series of cases in which hanging columellas were corrected with open rhinoplasties with transection of the crux medialis and inferior and lateral reorientation of the domus-crux lateralis, which are often combined with columellar cutting grafts13 (Figure 11)

FIGURE 11. Treatment options for hanging columella (A) Schematic representation of hanging columella. (B) Diagram representing transcolumellar approaches described by Armstrong (aggressive) and Joseph (open rhinoplasty with reconstruction of the crux medialis through structural grafts stabilized by sutures). (C) "Indirect" and (D) "Direct" approaches described by Randall.
We prefer an "indirect' approach for primary or secondary (i.e., mild to moderate) cases of hanging columella, where excess portions of septal cartilage and membranous septum are removed via endonasal approaches or open rhinoplasty.
For more severe cases of hanging columella, we use the "direct" approach described by Randall11, in which distal portions of the crux medialis are removed; this procedure is combined with total or partial resections below the domus angle13 (Figures 12 and 13).

Figure 12. Surgical sequence for hanging columella (A) Lifting of the cutaneous flap allows observation of the excess crux medialis portion. (B) Demarcation of the area to be resected. (C) A wedge resection of the crux medialis is performed to correct the cartilage hyperconvexity commonly observed in this deformity. (D) The anatomy of the crux medialis was re-established by suturing the corrected area. (E) Schematic representation and pre-operative aspects before and after treatment.

Figure 13. Treatment outcome of a severe case of hanging columella Owing to the complexity of the case, treatment was based on the combination of procedures described above. "Direct and indirect" approaches described by Randall were used, and partial resection of the crux medialis was adapted with sutures to treat the convexity typical of hanging columella, modifying concepts described by Armstrong and Joseph.
DISCUSSION
Rhinoplasty is one of the most complex and challenging procedures in plastic surgery1. We believe that the best aesthetic and functional outcomes in rhinoplasty can only be achieved through a continuous search for knowledge and observance of established diagnostic criteria that guide the proper treatment of alterations and deformities17.
Gunter described the most comprehensive and systematic classification of aesthetic alterations of alar-columellar relationships5. Although there are concerns about its complexity and application in clinical practice6, there is no doubt that accurate diagnosis facilitates selection of the best treatment option3, 5-14. Treatment options for aesthetic alterations of nasal columella vary according to the degree of deformity and surgeon preference and expertise. Asymmetrical alterations increase correction complexity and require different procedures for each side.
Over the years, we have observed hanging and hidden columella to be the most common aesthetic nasal columella alterations.
Chondral-mucoperichondrial nasal septal flap is our preferred choice for hidden columella correction. However, alternative procedures described by other authors also offer acceptable solutions, as we have described above5, 7, 10, 16. We consider the approaches described by Flowers et al. and Haddad et al. to be good alternatives for correction of hidden columella; however, we have no clinical experience with these procedures 8, 9.
Our approach for correcting hanging columellas depends on the severity of the deformity. For milder cases, we use Randall's approaches, whereas more severe cases require Randall's maneuvers combined with a partial resection of the crux medialis, which is subsequently restored with stabilization sutures5, 6, 11-14.
We agree with Rees et al. that rhinoplasty consists of a series of treatments aimed to harmonize overall nasal aesthetics3. However, we believe that maintenance and restoration of function are fundamental requirements necessary for applying the principles established by Rees to the current concept of rhinoplasty.
The techniques and strategies presented here are usually described independently only for didactic purposes and are often applied in combination to provide optimal aesthetic and functional outcomes.
CONCLUSION
Over more than forty years, we have developed a systematic approach for treatment of nasal columellar deformities; i.e. hanging and hidden columellas most commonly observed in clinical practice. A thorough diagnostic analysis is essential to achieve desired outcomes, as an accurate diagnosis guides selection of the most appropriate technique to correct columellar alterations and deformities. Gunter classification offers the best tool for this purpose. The strategic options described here are safe, reproducible, and provide satisfactory outcomes. Moreover, these procedures may be applied individually or in combination, as part of the techniques commonly used in rhinoplasty.
REFERENCES
1. Dini GM, Ferreira LM. Rhinoplasty and PubMed. Plast Reconstr Surg. 2006;118(1):289.
2. Mottura AA. Short columella nasolabial complex in aesthetic rhinoplasty. Aesthetic Plast Surg. 2001;25(4):266-72.
3. Rees TD, Baker DC, Tabbal N. Rhinoplasty problems and controversies : a discussion with the experts. St. Louis: Mosby; 1988.
4. Sheen JH, Sheen AP. Aesthetic rhinoplasty. St. Louis: C. V. Mosby Co.; 1978.
5. Gunter JP, Rohrich RJ, Friedman RM. Classification and correction of alar-columellar discrepancies in rhinoplasty. Plast Reconstr Surg. 1996;97(3):643-8.
6. Matarasso A, Greer SE, Longaker MT. The true hanging columella: simplified diagnosis and treatment using a modified direct approach. Plast Reconstr Surg. 2000;106(2):469-74.
7. Guyuron B. The aging nose. Dermatol Clin. 1997;15(4):659-64.
8. Flowers RS, Smith EM, Jr. Technique for correction of the retracted columella, acute columellar-labial angle, and long upper lip. Aesthetic Plast Surg. 1999;23(4):243-6.
9. Haddad Filho DH, Alonso N, Oksman D, Wulkan M, Godoy P. Surgical treatment of the acute columellar-labial angle. Aesthet Surg J. 2008;28(6):627-30.
10. Toriumi DM, Checcone MA. New concepts in nasal tip contouring. Facial Plast Surg Clin North Am. 2009;17(1):55-90.
11. Randall P. The direct approach to the "hanging columella". Plast Reconstr Surg. 1974;53(5):544-7.
12. Armstrong DP. Aggressive management of the hanging columella. Plast Reconstr Surg. 1980;65(4):513-6.
13. Joseph EM, Glasgold AI. Anatomical considerations in the management of the hanging columella. Arch Facial Plast Surg. 2000;2(3):173-7.
14. Gryskiewicz JM. The "iatrogenic-hanging columella": preserving columellar contour after tip retroprojection. Plast Reconstr Surg. 2002;110(1):272-7.
15. Rees TD, Baker DC, Tabbal N, Manhattan Eye Ear and Throat Hospital. Department of Plastic Surgery. New York University. Medical Center. Institute of Reconstructive Plastic Surgery. Rhinoplasty : problems and controversies : a discussion with the experts. St. Louis: Mosby; 1988.
16. Rohrich RJ, Huynh B, Muzaffar AR, Adams WP, Jr, Robinson Jr. Importance of the depressor septi nasi muscle in rhinoplasty: anatomic study and clinical application. Plast Reconstr Surg. 2000;105(1):376-83; discussion 84-8.
17. Dini GM, Albuquerque LG, Ferreira LM. The future of rhinoplasty and the Dallas rhinoplasty symposium. Plast Reconstr Surg. 2009;123(2):64e-5e.
1-Former BSPS and ILAFPS President; Honorary Member of BSPS and ILAFPS; Member of ASAPS, ASPS, ISAPS; Member of the Academy. Fluminense of Medicine
2-Member of BSPS, ISAPS - Plastic surgery
3-Member of BSPS - Plastic surgery
Institution: Private hospital.
Corresponding author:
Liacyr Ribeiro
Rua Visconde Silva, 52, salas 903/904. Botafogo
Rio de Janeiro. - CEP: 22271-092
Tel: (21) 2539-4893
Article received: July 17,2013
Article accepted: October 30, 2013
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket