



Reviw Article - Year 2013 - Volume 28 -
Use of stereophotogrammetry for evaluating craniofacial deformities: a systematic review
Uso da estereofotogrametria nas deformidades craniofaciais: revisão sistemática
ABSTRACT
Three-dimensional digital models of the face were developed to circumvent the limitations of the traditional assessment of soft tissue. Currently, a method reported to have a high clinical applicability is digital stereophotogrammetry. This systematic review aims to address the use of this technique in evaluating craniofacial abnormalities, with a focus on its practical application. The subject was searched in the Medline, Cochrane Library, LILACS, and SciELO databases. From preestablished inclusion criteria, 19 articles were selected. The data extracted were as follows: systems used, year of publication, diseases addressed, reference points used for each disease, advantages and disadvantages of the stereophotogrammetry system used, and quality of articles. The 3dMD® system was used in 11 articles. The most common publication year was 2010, with 6 studies. Twelve studies addressed cleft lip and palate, and 17 studies used anthropometric landmarks. Noninvasiveness, fast image acquisition, and accuracy were the advantages mentioned in 70% of the articles that used the 3dMD® system. The most frequently mentioned disadvantage of such equipment was the high cost. Twelve items had good level of scientific evidence. Digital stereophotogrammetry is a technology aimed to improve the evaluation of treatments and quantification of craniofacial deformities. However, there is a need for more studies with long-term monitoring and on the association of a wider variety of systems.
Keywords: Photogrammetry. Craniofacial abnormalities. Imaging, three-dimensional. Photography. Review.
RESUMO
O desenvolvimento de modelos tridimensionais digitais da face foi uma das formas de contornar as limitações dos métodos tradicionais de avaliação de tecidos moles. Para tanto, o método com maior aplicabilidade clínica atualmente é a estereofotogrametria digital. Esta revisão sistemática objetiva abordar o uso dessa técnica em anormalidades craniofaciais, com foco em sua aplicação prática. Foram realizadas buscas sobre o tema nas bases de dados Medline, Cochrane Library, LILACS e SciELO. A partir de critérios de inclusão preestabelecidos, 19 artigos foram selecionados. Extraíram-se dados sobre: sistemas utilizados, ano de publicação, doenças abordadas, pontos de referência usados para cada doença, vantagens e desvantagens da estereofotogrametria por sistema utilizado e qualidade dos artigos. O sistema 3dMD® foi o equipamento empregado em 11 artigos. O ano de publicação mais frequente foi 2010, com 6 trabalhos. Doze estudos abordaram fissuras labiopalatinas e 17 trabalhos utilizaram pontos de referência antropométricos. O caráter não-invasivo, a rápida aquisição de imagens e a acurácia foram as vantagens referidas em 70% dos artigos que aplicaram o sistema 3dMD®. A desvantagem desse mesmo equipamento apontada com maior frequência foi o alto custo. Doze artigos possuíam bom nível de evidência científica. A estereofotogrametria digital é uma tecnologia capaz de aperfeiçoar o modo de avaliação dos tratamentos e quantificação das deformidades craniofaciais. Entretanto, há necessidade de realização de mais estudos com acompanhamento a longo prazo e associação de maior variedade de sistemas.
Palavras-chave: Fotogrametria. Anormalidades craniofaciais. Imagem tridimensional. Fotografia. Revisão.
The success of craniomaxillofacial surgery depends not only on the technical aspects of the operation but also on comprehensive surgical planning. Traditionally, this plan consists of 5 steps: data collection, diagnosis and quantification of the condition, establishing a preliminary surgical plan, surgical simulation, establishment of the final surgical plan, and transfer of the patient during the actual procedure 1.
To perform all these steps and evaluate the results of surgery, medical professionals commonly use methods such as physical examination, radiographs (cephalometric and panoramic radiographs), medical-dimensional photographs, gutters, clinical anthropometry, dental models, and predictive tracings from radiographic cephalometry. However, with these approaches, the three-dimensional visualization of the process is limited to the imagination of each person involved, causing communication problems. Moreover, as cephalometry and traditional photographs provide two-dimensional views, the management of patients with asymmetrical deformities (34% of teeth and facial deformities 1) is only grossly shown. Other obstacles are the planning for the transfer to the operating room for patients without dental abnormalities, and the use of different po sitioning of the patient in the evaluation methods cited, reducing the quality of the prediction 1-3.
One of the ways to improve the process described is the development of three-dimensional digital models of facial morphology 2. Systems with several different approaches were designed to generate a three-dimensional surface, and digital stereophotogrammetry is a method with a high clinical applicability reported 4,5. This technique consists in acquiring a three-dimensional image from 1 or more pairs of stereophotographs, with the term "photogrammetry" being related to the possibility of conducting measurements by using three-dimensional pictures 6, and if associated with the CT scan of the patient, using the structure of the underlying bone 4.
The analysis of three-dimensional models of stereophot ogrammetry can be made by means of linear, volume, angular, or area measurements, and/or by comparison of pattern reference points or whole faces. The more relevant the issues addressed in a model, the better the quality of the study results7,8.
This systematic review aims to address the use of stereophotogrammetry in evaluating craniofacial deformities, focusing on its practical application.
METHODS
We searched for articles and possible systematic reviews on the use of stereophotogrammetry in craniofacial deformities, on December 17, 2011, in the Medline, Cochrane Library, LILACS, and SciELO databases. In Medline, the keywords used were "photogrammetry" and "craniofacial abnormalities" (search details: "Photogrammetry" [MeSH] AND "Craniofacial Abnormalities" [MeSH]). In Cochrane Library, the MeSH term "photogrammetry" was used in the search. In searching LILACS and SciELO, we used the word "photogrammetry" in the simple search.
From the abstracts of the articles found, we manually selected those that met the following inclusion criteria: used digital stereophotogrammetry in craniomaxillofacial surgery and/or orthodontics; published in English, Spanish, or Portuguese; with trial, full version available online through the portal of CAPES journals (www.periodicos.capes.gov.br), or have free access.
From Medline, 70 articles were initially retrieved. After the selection using the criteria described, 17 articles were identified for further analysis. The Cochrane Library provided 68 clinical trials and 1 technical note (classified as "economic evaluation"), which, after exclusion, resulted in 3 articles, one of which was already among the 17 recovered from Medline. No articles that met the established criteria were found in LILACS and SciELO, which showed 60 and 26 initial results, respectively. We found no systematic review of digital stereophotogrammetry.
In the 19 selected articles, the following data were collected: systems used, year of publication, diseases addressed, reference points used for each disease, advantages and disadvantages of stereophotogrammetry according to the system used, and the quality of the studies. This review aims to understand the advances, applicability, and limitations of using this technology in craniofacial abnormalities.
RESULTS
Systems Used
In the 19 articles selected, the following systems were used:
Publication Year3dMD® system[I] - used in 11 articles (3 articles: 3dMD Cranial®[II]; 5 articles: 3dMD Face®[III]; 2 articles: 3dMD DSP 400®[IV]; 1 article: 3dMD® not specified)3,7-16; C3D® system[V] - used in 3 articles17-19; 2 semimetric cameras (Rollei 6006 Réseau®[VI]) - used in 3 articles20-22; 2 professional photo cameras (Nikon FM2®[VII]) - used in 2 articles23,24; Genex FaceCam 250®[VIII] - used in 1 article that additionally used the 3dMD® system13. The C3D® system is not commercially available and originates from the University of Glasgow (UK)25.
The selected articles were published from 1994 to 2011:
Figure 1 shows the article distribution according to publication year.2011: 1 article published9; 2010: 6 articles published3,7,8,10-12; 2009: 2 articles published13,14; 2007: 2 articles published15,17; 2006: 1 article published16; 2004: 1 article published18; 2003: 1 article published19; 1997: 1 article published23; 1996: 1 article published24; 1995: 1 article published20; 1994: 2 articles published21,22.

Figure 1 - Distribution of the articles according to publication year.
Diseases Approached
Figure 2 shows the disease distribution according to the number of articles that addressed each condition, as follows:

Figure 2 - Distribution of diseases according to the number of articles that addressed them.
Reference Points Used by DiseaseCleft lipandpalate-addressedby 12articles3,9,12,13,15-22; Nonsynostotic cranial deformity - addressed by 3 articles7,8,10; Extraction of the third lower molar - addressed by 2 articles23,24; 22qll.2 deletion syndrome - addressed by 1 article14; Class III occlusion - addressed by 1 article, additionally referring to cleft lip and palate12; Nonspecific - 1 article does not address any specific disease11.
We identified the reference points used in each of the articles and in accordance with the condition addressed. When there was correspondence, we used the nomenclature proposed by Farkas & Munro26 or Kolar & Salter27 for identification of the reference points in each article. Some of the items made use of nonanthropometric/constructed reference points without connection to a specific anatomical structure7,9,12,15,23,24.
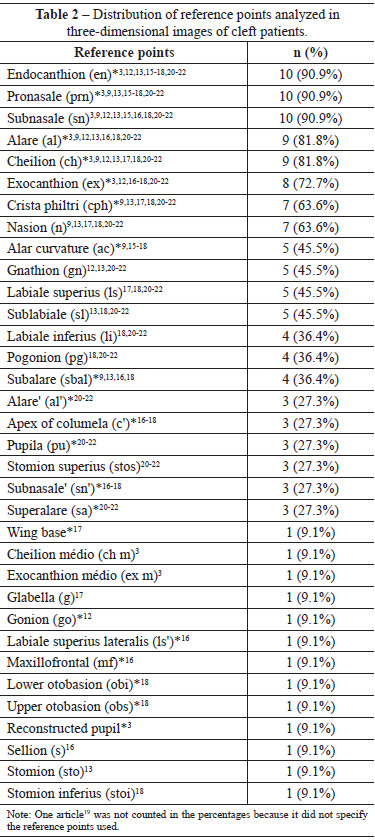
Tables 1 and 2 list, respectively, the reference points of the 2 conditions addressed more often - nonsynostotic cranial deformities, and cleft lip and palate. Bilateral points on the face were analyzed as a single entity, since all the studies used the left and right sides in the analysis; when they are mentioned, the items have been marked with an asterisk.

Studies that have addressed extraction of the mandibular third molar used only nonanthropometric points in their analysis23,24.
Advantages and Disadvantages
Mentioned by the Authors
The advantages and disadvantages of stereophotogrammetry and methods of three-dimensional imaging, as indicated by the authors, were analyzed according to the system used.
Tables 3 and 4 list, respectively, the advantages and disadvantages mentioned in the articles that used the 3dMD® system.
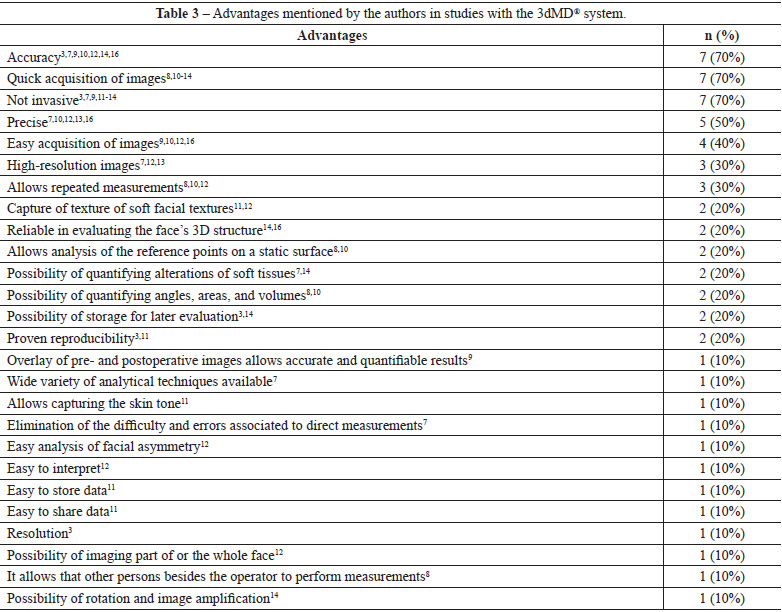

The study that used the FaceCam 250 Genex® system13 was considered along with those that used the 3dMD®, as these systems are considered equivalent. A percentile analysis was made for the advantages of 3dMD®.
Quality of the Articles
To assess the quality of the articles, they were categorized by study design, presence of a control group, sample size, group composition analysis, evaluation of intra- and interoperator reliability, and time tracking.
Study Design
Concerning study design, the following results were obtained:
Control GroupClinical trials - 10 articles3,7,9,10,15,17-19,23,24; Observational studies - 5 articles13,16,20-22; Technical notes - 2 articles11,12; Diagnostic accuracy studies - 2 articles8,14.
Seven articles had no control group3,8-11,17,24, whereas 12 articles included a control group7,12-16,18-23.
Sample Size
In studies with a control group, the sample size was established by the total number of patients analyzed, subtracting those belonging to the control group. The studies had samples between 10 and 181 individuals (Figure 3).

Figure 3 - Distribution of references of the 19 articles selected according to sample size.
Composition of the Analysis Groups
When extracting data on the composition of the groups formed in each study, there was heterogeneity in 2 articles:
Evaluation of Intra- and Interoperator Reliability"Facial surface changes after cleft alveolar bone grafting"9 - results that belonged to the group with unilateral cleft lip and those that belonged to the group with bilateral cleft lip and palate were not segregated; "3D stereophotogrammetric assessment of pre- and postoperative volumetric changes in the cleft lip and palate nose"3 - results that belonged to the group with unilateral cleft lip and palate and those that belonged to the group with unilateral cleft lip alone were not segregated.
The presence or absence of evaluation of intra- and interoperator reliability was analyzed (Figure 4). Four articles3,8,14,18 verified both types of reliability, whereas 11 articles9,10,13,15,17,19-24 did not.
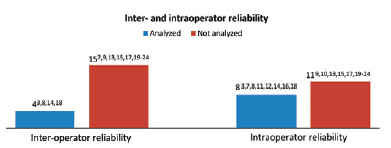
Figure 4 - Distribution of the 19 articles selected according to the presence or absence of analysis of inter- and intraoperator reliability.
Follow-up Time by Treatment
Data on follow-up time were extracted from articles involving stereophotogrammetry after therapeutic intervention (Figure 5). Studies involving surgery presented the shortest period between the procedure and the acquisition of three-dimensional photos. When the approach was nonsurgical- data were included on the duration of treatment. The articles were additionally separated by the type of therapeutic approach.

Figure 5 - Follow-up time of the patient in each of the therapeutic interventions addressed.
DISCUSSION
Nowadays, stereophotogrammetry is the most promising three-dimensional imaging system for accurate diagnoses and face assessments28. Therefore, to understand the advances, limitations, and applicability of this technology, a systematic review was conducted on its application in craniofacial abnormalities.
Systematic reviews are among the study designs with the highest level of evidence, being based on a comprehensive and exhaustive search of primary studies focused on a specific subject 29. In our search, we used the Medline, Cochrane Library, LILACS, and SciELO databases, selected for their relevance among those that had free access. The search was performed using MeSH terms or other words that match the topic of "stereophotogrammetry in craniofacial abnormalities." The words used were "photogrammetry" and "craniofacial abnormalities", using only the first word when the results of the search were lacking or insufficient. Using predetermined exclusion criteria, we selected 19 scientific papers.
Concerning the systems used in the 19 selected articles,it was observed that about 57.9% of studies used the 3dMD® system, with the other 4 systems individually covering minor fractions of similar magnitude. Probably, this finding is justified by the fact that the 3dMD® system has been a pioneer in the market (launched in 2005 6), among the systems capturing the three-dimensional morphology of the face, combining stereophotogrammetry with the projection of a random pattern of structured light. There are several advantages atributed to such a system, especially accuracy3,7,9,10,12,14,16, reproducibility3,11, quick acquisition of images3,8,10-14, and the possibility of capturing the facial texture11,12. When analyzing the advantages listed about the other systems, it appears that the majority are already included in the list for 3dMD®.
As far as the year of publication is concerned, it was found that from 1994- few studies were being produced, until a peak emerged in 2010. This peak was generated by 6 articles, all of which used the 3dMD® system. Furthermore, the 3 studies that used the system to capture three-dimensional cranial images (Cranial 3dMD®) are included among these 7 articles7,8,10. This increase in the number of published papers can be attributed to the effectiveness of the disclosure system and its advantages over the conventional technologies4,5,11. Furthermore, because the system has restricted portability3 and high cost3,11, it is understandable that there is a delay from its launch to its application in routine medical practice, as a result of certain factors that require time, such as technology validation, capture of funds, importation, and familiarity with its use.
Concerning the diseases addressed, 63.2% of the articles studied cleft lip and palate, and nonsynostotic cranial deformities were the second most common condition (15.8%). Although both conditions require a three-dimensional approach for appropriate treatment8,7,10,20,22, nonsynostotic cranial deformities are usually solved with active repositioning of the child, with the use of orthotic helmets reserved for more severe cases. The possibility of surgical resolution of nonsynostotic cranial deformities is very low7,30, with aesthetic improvement being the only aim of surgery31. On the other hand, cleft patients should always undergo surgery, which aims to improve the patient's functional and aesthetic outcome, although the management of this condition is still a subject of debate 32. Thus, the main focus of the scientific community concerning clefts is possibly the difficulty of treating them satisfactorily and evaluating the final results.
In the analysis of the 5 conditions addressed in 19 scientific papers, the use of facial reference points was unanimous. With the exception of 2 studies on swelling after third lower molar extraction23,24, all other articles used anthropometric reference points. Among these anthropometric reference points, those that had higher application were the most widespread and easily located: endocanthion, exocanthion, pronasale, subnasale, wing, cheilion, crista philtri, nasion, and opisthocranion. The clefts, the most commonly used reference points, are located in the middle third of the face and in the upper portion of the lower third of the face. In turn, the analysis of nonsynostotic cranial deformities evaluated cranial and facial key points such as euryon, opisthocranion, inion, nasion, tragion, vertex, cheilion, and alare, which provide general morphological information about the head. In the study of 22q11.214 deletion, facial analysis sought to quantify the "facies" typical of the syndrome, addressing the 3/3 and ears with facial reference points already established. With respect to the list made to evaluate a patient with class III malocclusion 12, no anthropometric points of the middle and lower third of the face covering both such other conditions that the paper studies.
The main difficulty in extracting data on the reference points used in each article was the heterogeneity of the names used to refer to the same facial parameter. While some articles14,18 applied, for the most part, the classifications proposed by Farkas & Munro26 or Kolar & Salter27, other studies7 referred to the points by using a description of its location. An effort to use the same nomenclature is essential to avoid misinterpretations of the work and facilitate the use of information in other articles.
In assessing the quality of the articles, it was found that 63.2% of the studies had a similar design to clinical trials or diagnostic accuracy studies considered to have good level of scientific evidence by the Oxford Centre for Evidence-based Medicine33. Following these criteria, 26.3% of the remaining studies showed low level of evidence, being observational studies, and 16.7% were without evidence, since they were in the form of technical notes.
Additionally, it was found that 63.2% of the articles used control groups; however, the majority consisted of healthy individuals in order to have a standard for comparison of the final results. Only 2 articles used control groups that included subjects having the medical condition of the group to which they were compared; in one of these articles23, placebo was prescribed for the controls and the other used a traditional treatment 7.
The sample size in the studies varied between 10 and 181 individuals. Possibly, this difference is due to the presence of services that already have the technology for some time and others who are only starting their research with the equipment. A fact supporting this hypothesis is that the 2 studies with larger samples (18110 and 1008 patients) have a common origin - the University of Giessen, Germany.
Interestingly, only 2 studies used 2 different conditions to form a group of analysis3,9. Probably, these instances are justified more by the lack of research subjects rather than the lack of knowledge of the authors about the distinction between the conditions.
Since most studies used measurements and digital identification reference points, the evaluation of both intra- and interoperator reliability is necessary for a substantially validated work. However, there were no data on the interoperator reliability in 79% of articles. A possible explanation for this result could be the difficulty of finding persons familiar with the system and available to obtain the measurements.
In the final analysis of this systematic review, we obtained data on the follow-up time of patients in some studies involving a therapeutic approach (68.4%). A great source of errors that can be probed in this data extraction is the time to photograph the patient postoperatively (in 10 of 13 articles with some therapeutic approach involving surgery)- because if the photograph was taken very early, the final appearance may still not be reflected. Concerning this aspect, the largest discrepancy was observed in surgeries involving the nose-which showed the following follow-up times: 9 weeks19; 1 month15; and 1- 33- and 6 months17. Therefore, as the end result of a rhinoplasty can take 6 months to 2 years to show34, the article with the longest follow-up time waited only until the lower limit of the safe range.
Digital stereophotogrammetry can overcome the limitations of the traditional two-dimensional analysis of facial soft tissues. Therefore, high- quality scientific studies are required to validate the use of this method in several conditions that constitute the spectrum of craniofacial abnormalities.
CONCLUSIONS
Digital stereophotogrammetry is a noninvasive, accurate, and easy-to-manipulate technology for the evaluation of treatments and quantification of craniofacial deformities. Currently, the most frequently applied system offering a high number of advantages cited is 3dMD®. However, there is need for more studies with long-term monitoring and on the association of a wider variety of systems.
REFERENCES
1. Gateno J, Xia JJ, Teichgraeber JF. New methods to evaluate craniofacial deformity and to plan surgical correction. Semin Orthod. 2011;17(3):225-34.
2. Hammond P. The use of 3D face shape modelling in dysmorphology. Arch Dis Child. 2007;92(12):1120-6.
3. van Loon B, Maal TJ, Plooij JM, Ingels KJ, Borstlap WA, Kuijpers-Jagtman AM, et al. 3D stereophotogrammetric assessment of pre- and postoperative volumetric changes in the cleft lip and palate nose. Int J Oral Maxillofac Surg. 2010;39(6):534-40.
4. Schendel SA, Duncan KS, Lane C. Image fusion in preoperative planning. Facial Plast Surg Clin North Am. 2011;19(4):577-90.
5. Heike CL, Upson K, Stuhaug E, Weinberg SM. 3D digital stereophotogrammetry: a practical guide to facial image acquisition. Head Face Med. 2010;6:18.
6. Kau CH, Richmond S, Incrapera A, English J, Xia JJ. Three-dimensional surface acquisition systems for the study of facial morphology and their application to maxillofacial surgery. Int J Med Robot. 2007;3(2):97-110.
7. Lipira AB, Gordon S, Darvann TA, Hermann NV, Van Pelt AE, Naidoo SD, et al. Helmet versus active repositioning for plagiocephaly: a three-dimensional analysis. Pediatrics. 2010;126(4):e936-45.
8. Schaaf H, Pons-Kuehnemann J, Malik CY, Streckbein P, Preuss M, Howaldt HP, et al. Accuracy of three-dimensional photogrammetric images in non-synostotic cranial deformities. Neuropediatrics. 2010;41(1):24-9.
9. Krimmel M, Schuck N, Bacher M, Reinert S. Facial surface changes after cleft alveolar bone grafting. J Oral Maxillofac Surg. 2011;69(1):80-3.
10. Schaaf H, Malik CY, Streckbein P, Pons-Kuehnemann J, Howaldt HP, Wilbrand JF. Three-dimensional photographic analysis of outcome after helmet treatment of a nonsynostotic cranial deformity. J Craniofac Surg. 2010;21(6):1677-82.
11. Germec-Cakan D, Canter HI, Nur B, Arun T. Comparison of facial soft tissue measurements on three-dimensional images and models obtained with different methods. J Craniofac Surg. 2010;21(5):1393-9.
12. Hoefert CS, Bacher M, Herberts T, Krimmel M, Reinert S, Hoefert S, et al. Implementing a superimposition and measurement model for 3D sagittal analysis of therapy-induced changes in facial soft tissue: a pilot study. J Orofacl Orthop. 2010;71(3):221-34.
13. Weinberg SM, Naidoo SD, Bardi KM, Brandon CA, Neiswanger K, Resick JM, et al. Face shape of unaffected parents with cleft affected offspring: combining three-dimensional surface imaging and geometric morphometrics. Orthod Craniofac Res. 2009;12(4):271-81.
14. Heike CL, Cunningham ML, Hing AV, Stuhaug E, Starr JR. Picture perfect? Reliability of craniofacial anthropometry using three-dimensional digital stereophotogrammetry. Plast Reconstr Surg. 2009;124(4):1261-72.
15. Singh GD, Levy-Bercowski D, Yanez MA, Santiago PE. Three-dimensional facial morphology following surgical repair of unilateral cleft lip and palate in patients after nasoalveolar molding. Orthod Craniofac Res. 2007;10(3):161-6.
16. Krimmel M, Kluba S, Bacher M, Dietz K, Reinert S. Digital surface photogrammetry for anthropometric analysis of the cleft infant face. Cleft Palate Craniofac J. 2006;43(3):350-5.
17. Devlin MF, Ray A, Raine P, Bowman A, Ayoub AF. Facial symmetry in unilateral cleft lip and palate following alar base augmentation with bone graft: a three-dimensional assessment. Cleft Palate Craniofacial J. 2007;44(4):391-5.
18. Hood CA, Hosey MT, Bock M, White J, Ray A, Ayoub AF. Facial characterization with cleft lip and palate using a three-dimensional capture technique. Cleft Palate Craniofac J. 2004;41(1):27-35.
19. Hood CA, Bock M, Hosey MT, Bowman A, Ayoub AF. Facial asymme-try--3D assessment of infants with cleft lip & palate. Int J Pediatr Dent. 2003;13(6):404-10.
20. Ras F, Habets LL, van Ginkel FC, Prahl-Andersen B. Longitudinal study on three-dimensional changes of facial asymmetry in children between 4 to 12 years of age with unilateral cleft lip and palate. Cleft Palate Craniofac J. 1995;32(6):463-8.
21. Ras F, Habets LL, van Ginkel FC, Prahl-Andersen B. Facial left-right dominance in cleft lip and palate: three-dimensional evaluation. Cleft Palate Craniofac J. 1994;31(6):461-5.
22. Ras F, Habets LL, van Ginkel FC, Prahl-Andersen B. Three-dimensional evaluation of facial asymmetry in cleft lip and palate. Cleft Palate Craniofac J. 1994;31(2):116-21.
23. Uçok C. Stereophotogrammetric assessment of the effect of tenoxicam on facial swelling subsequent to third molar surgery. Int J Oral Maxillofac Surg. 1997;26(5):380-2.
24. Mocan A, Kişnişci R, Uçok C. Stereophotogrammetric and clinical evaluation of morbidity after removal of lower third molars by two different surgical techniques. J Oral Maxillofac Surg. 1996;54(2):171-5.
25. Honrado CP, Larrabee WF Jr. Update in three-dimensional imaging in facial plastic surgery. Curr Opin Otolaryngol Head Neck Surg. 2004;12(4):327-31.
26. Farkas LG, Munro IR. Anthropometric facial proportions in medicine. Springfield: Charles C. Thomas; 1987.
27. Kolar JC, Salter EM. Craniofacial anthropometry: practical measurements of the head and face for clinical, surgical and research use. Springfield: Charles C. Thomas; 1996.
28. Moos KF, Ayoub AF. The surgical correction of dentofacial deformities, past, present and future. Egypt J Oral Maxillofac Surg. 2010;1:2-6.
29. Pai M, McCulloch M, Gorman JD, Pai N, Enanoria W, Kennedy G, et al. Systematic reviews and meta-analyses: an illustrated, step-by-step guide. Nati Med J India. 2004;17(2):86-95.
30. Hutchison BL, Hutchison LA, Thompson JM, Mitchell EA. Plagiocephaly and brachycephaly in the first two years of life: a prospective cohort study. Pediatrics. 2004;114(4):970-80.
31. Rogers GF. Severe deformational plagiocephaly: long-term results of surgical treatment. J Craniofac Surg. 2011;22(1):30-2.
32. WHO Human Genetics Programme. Global strategies to reduce the health-care burden of craniofacial anomalies: report of WHO meetings on international collaborative research on craniofacial anomalies. Geneva: World Health Organization; 2002.
33. Oxford Centre for Evidence-based Medicine. Level of evidence. Disponível em: http://www.cebm.net/index.aspx?o=1025 Acesso em: 11/1/2012.
34. Harsha BC. Complications of rhinoplasty. Oral Maxillofac Surg Clin North Am. 2009;21(1):81-9.
1. Student at the Faculty of Medicine, University of São Paulo (FMUSP), São Paulo, SP, Brazil
2. Master in Plastic Surgery at FMUSP, assistant physician of craniomaxillofacial surgery, Division of Plastic Surgery and Burns, Hospital das Clinicas, Faculty of Medicine, University of São Paulo (HC-FMUSP), São Paulo, SP, Brazil
3. Student at the Faculty of Dentistry, University of São Paulo, São Paulo, SP, Brazil
4. Lecturer in plastic surgery at the FMUSP, associate professor of HC-FMUSP, Head of the Department of Craniomaxillofacial Surgery, Division of Plastic Surgery and Burns, HC-FMUSP, São Paulo, SP, Brazil
Correspondence to:
Nivaldo Alonso
Rua Afonso Brás, 473 - cj. 65 - Vila Nova Conceição
São Paulo, SP, Brazil - CEP 04511-000
E-mail: nivalonso@gmail.com
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: January 24, 2012
Article accepted: June 19, 2012
This work was performed at the Craniomaxillofacial Surgery, Division of Plastic Surgery and Burns, Hospital das Clinicas, Faculty of Medicine, University of São Paulo (HC-USP), São Paulo, SP, Brazil.
[I] 3dMD® (3dMD, Atlanta, GA, USA): company responsible for the production of systems of digital stereophotometry and associated software.
[II] 3dMD Cranial® (3dMD, Atlanta, GA, USA): a digital stereophotometry system for acquiring craniofacial images.
[III] 3dMD Face® (3dMD, Atlanta, GA, USA): a digital stereophotometry system for acquiring facial images.
[IV] 3dMD DSP 400® (3dMD, Atlanta, GA, USA): a digital stereophotometry system for acquiring facial images.
[V] C3D® (Glasgow University Dental School): a digital stereophotometry system.
[VI] Rollei 6006 Réseau® (Rollei Fototechnic GmbH, Braunschweig, Germany): a semimetric camera.
[VII] Nikon FM2® (Nikon Corporation, Tokyo, Japan): a professional photo camera.
[VIII] Genex FaceCam 250® (Genex Technologies Inc., Kensington, MD, USA): a digital stereophotometry system.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket